
Abstract
Background:
Peripheral artery disease (PAD) encompasses conditions with poor outcome and severe suffering, both mentally and physically, yet utilization and research into palliative care interventions remain sparse.
Objective:
The purpose of this study is to identify existing evidence on palliative care intervention for chronic limb threatening ischaemia (CLTI) and abdominal aortic aneurysm (AAA).
Design:
We conducted a PROSPERO-registered systematic review of studies published between 1991 and 2020 in which people with PAD received palliative care interventions and at least one patient outcome was recorded. For the purpose of this study, a palliative care intervention was defined as one which aims primarily to reduce negative impact of PAD on patients' and/or caregivers' physical, emotional, psychological, social, or spiritual condition.
Results:
A total of 8 studies involving 87,024 patients met the inclusion criteria (4 cohort studies and 4 cross-sectional studies). Methodological quality ranged from low to moderate. The small number of studies and study heterogeneity precluded meta-analysis. Regarding our primary outcomes, only two articles recorded patient-reported outcomes. Five articles found an association between palliative care and reduction in health care utilization, a secondary outcome of the study. Most of the studies reported that palliative care was likely underused. Only two of the studies included non-hospital patients.
Conclusion:
Despite high mortality and morbidity associated with PAD, evidence of the effectiveness of palliative care in this group of patients is lacking. There are only a handful of articles on palliative care for people with PAD, and the majority are small, methodologically flawed and lack meaningful patient-reported outcomes. High-quality research of palliative care interventions in patients with PAD is urgently needed to better understand the impact of palliative care on quality of end of life and to develop and evaluate service-level interventions.
Introduction
Peripheral artery disease (PAD)—pathological change of blood vessels outside the heart such as chronic limb-threatening ischemia (CLTI) and abdominal aortic aneurysm (AAA)—has high mortality and morbidity and comes with high symptom burden and psychological distress resulting in a low quality of life (QoL).1,2 Therefore, timely palliative care input, with its focus on management of symptoms, psychosocial support, and assistance with advanced decision making, has the potential to improve the quality of end-of-life (EoL) care for this patient group. PAD is estimated to affect more than 200 million people worldwide, and the prevalence is rising, with the main risk factors including advancing age, diabetes, smoking, hypercholesterolemia, and hypertension, it is likely that the proportion of people affected will continue to grow.1,3 Despite considerable technological advances, PAD still carries a five-year mortality as high as 33.2%. 4 Patients presenting with CLTI have a five-year mortality higher than 50%, higher than Duke's C colorectal cancer. 5
It was 1960 when Saunders published her first article on palliative care for cancer patients, 6 which laid the foundation for the comprehensive pathways available to cancer patients today. Studies have shown that palliative care interventions can reduce pain,7–9 improve communication,7–12 improve mental and physical well-being,7–9,11,12 and reduce hospital burden.7,8,10,11,13 Sixty years have since passed, yet today the role of palliative care in PAD remains underutilized14–16 and based on limited evidence. 8
Comprehensive palliative care should encompass physical, mental, social, and spiritual aspects, 17 and it is likely that vascular patients have a unique set of EoL care goals and needs. For example, it is reasonable to suppose that since ischemic pain has been proven to have peripheral pathophysiology dissimilar to other causes of pain,18,19 CLTI patients experience pain differently and therefore may need alternative analgesic strategies.
The lack of research into palliative care for PAD is reflected by low public awareness of the condition. This is in marked contrast with conditions such as motor neuron disease, cystic fibrosis, and multiple sclerosis, despite PAD being significantly more prevalent. 20 This could, in part, be due to the low socioeconomic status of many of the people suffering from PAD. 21 This characteristic could be another contributing factor to the unique set of EoL care goals in vascular patients.
The purpose of this systematic review was to identify and evaluate palliative care interventions used in PAD to help guide future research.
Methods
Review design
We designed a systematic review protocol in accordance with PRISMA guidelines22,23 and registered it on PROSPERO 24 before commencing the database search. For the purpose of this study, a palliative care intervention was defined as one which aims primarily to reduce negative impact of PAD on patients' and/or caregivers' physical, emotional, psychological, social, or spiritual condition.
Data sources and search strategy
We searched PubMed, PsycINFO, EMBASE, and the clinical trials databases of studies published between January 1, 1991, and January 1, 2020. Index terms and text words used in the search included: “palliative care, advance care planning, advance directive, EoL care, palliative medicine, terminal illness, terminal care, pain management, symptom, death, dignity, patient comfort, religious belief, spiritual care, pastoral care and supportive care.” These were searched in combination with terms encompassing vascular surgery including: “peripheral arter* disease, vascular disease, vascular surgery, endovascular surgery, abdominal aortic aneurysm, and chronic limb ischaemia.”
The search was further refined to only include articles published in English and studies conducted on adult humans. In addition, we filtered out articles not classified as observational studies. The full search strategy is presented in Supplementary Table S1. Finally, we also included articles identified from a manual review of the articles included and researchers' personal archives. The search strategy was designed with the guidance of a research librarian.
Study inclusion and exclusion criteria
We included experimental, quasi-experimental, and observational studies published between January 1, 1991, and January 1, 2020. Populations included patients with PAD who had palliative care interventions and measurement of at least one patient-orientated outcome. Palliative care interventions were defined as any clinical intervention delivered by a palliative care team or professional, aimed at alleviation of physical, mental, spiritual, or social detriment caused by the illness. Studies that included multiple pathologies were also considered if more than 20% of patients were reported to have PAD.
We excluded studies that were not peer reviewed; single palliative surgical procedures; acute postoperative pain interventions; complementary and alternative medicines; no control or comparison group; and review, editorial, abstract, or conference proceedings.
Outcomes
Primary outcomes of interest in this study were pain and symptom management; psychological and spiritual care; social support; meeting patient end-of-care goals; and communication and surgeon education, training, and support in the administration of palliative care. Secondary outcomes of interest were health care utilization and cost.
Study selection and data extraction
Titles and abstracts from the final search were screened by two authors (H.D. and R.L.) using Rayyan. 25 In the second phase, the same two authors independently reviewed full texts of articles identified in phase one for eligibility. A third author (M.A.W.) decided discrepancies between the first two authors. The first two authors were blinded to each other's decisions during both phases.
Study design and methodology, participant demographics, intervention, and outcome data were then extracted by H.D. onto evidence tables (Tables 1 and 2) and checked by M.A.W. Authors of included articles were contacted for missing data.
Summary of Articles
Based on the Newcastle–Ottawa Scale given in Supplementary Table S2.
95% [CI], 95% confidence incidence; [aMR] ¼, adjusted mean ratio; CLI, critical limb ischemia; CSS, cross-sectional study; HS, health status; LOS, length of stay; NIS, nationwide inpatient sample; PAD, peripheral artery disease; PC, palliative care; PCC, palliative care consultation; QoL, quality of life.
Summary of Measured Outcomes
X, Research article reported outcome in corresponding column; —, Research article did not report outcome in corresponding column.
Data analysis
Following selection and data extraction, we performed a narrative synthesis by assessing methodological quality and bias and presenting this, along with study design, palliative care intervention, and outcome, in extensive evidence tables (Tables 1 and 2). Before performing the final search, we determined that the number of studies found, I2 and χ 2 calculated in RevMan, and size and effect of the studies would be taken into consideration to decide whether a meta-analysis would be performed. The processing of the data and decision of whether to carry out a meta-analysis was be carried out by H.D. and R.L., and disagreements would be decided by M.I.B., J.R.d.S., and M.A.W. Due to the small number of studies and heterogeneity, we were unable to perform a meta-analysis.
Quality assessment
We used the Newcastle–Ottawa Scale 26 (NOS) to evaluate the methodological quality, as they were all nonrandomized studies. H.D. and R.L. independently graded the articles against this scale, and differences were resolved by M.A.W. From the NOS rating, studies were assigned an overall quality rating.
Results
Search outcome
Searches identified 2772 articles. After titles and abstracts screening, 23 articles remained—of which, 8 were deemed to meet the inclusion criteria following independent reviews of full text. A flowchart of the literature search along with reasons for article exclusion is shown in Figure 1. Inter-rater agreement was very high (κ = 0.99). Therefore, our final analysis was of eight studies of seven unique interventions, as two of the articles27,28 looked at the same intervention and patient cohort. The seven unique interventions had a total of 87,024 patients in the intervention and control groups.
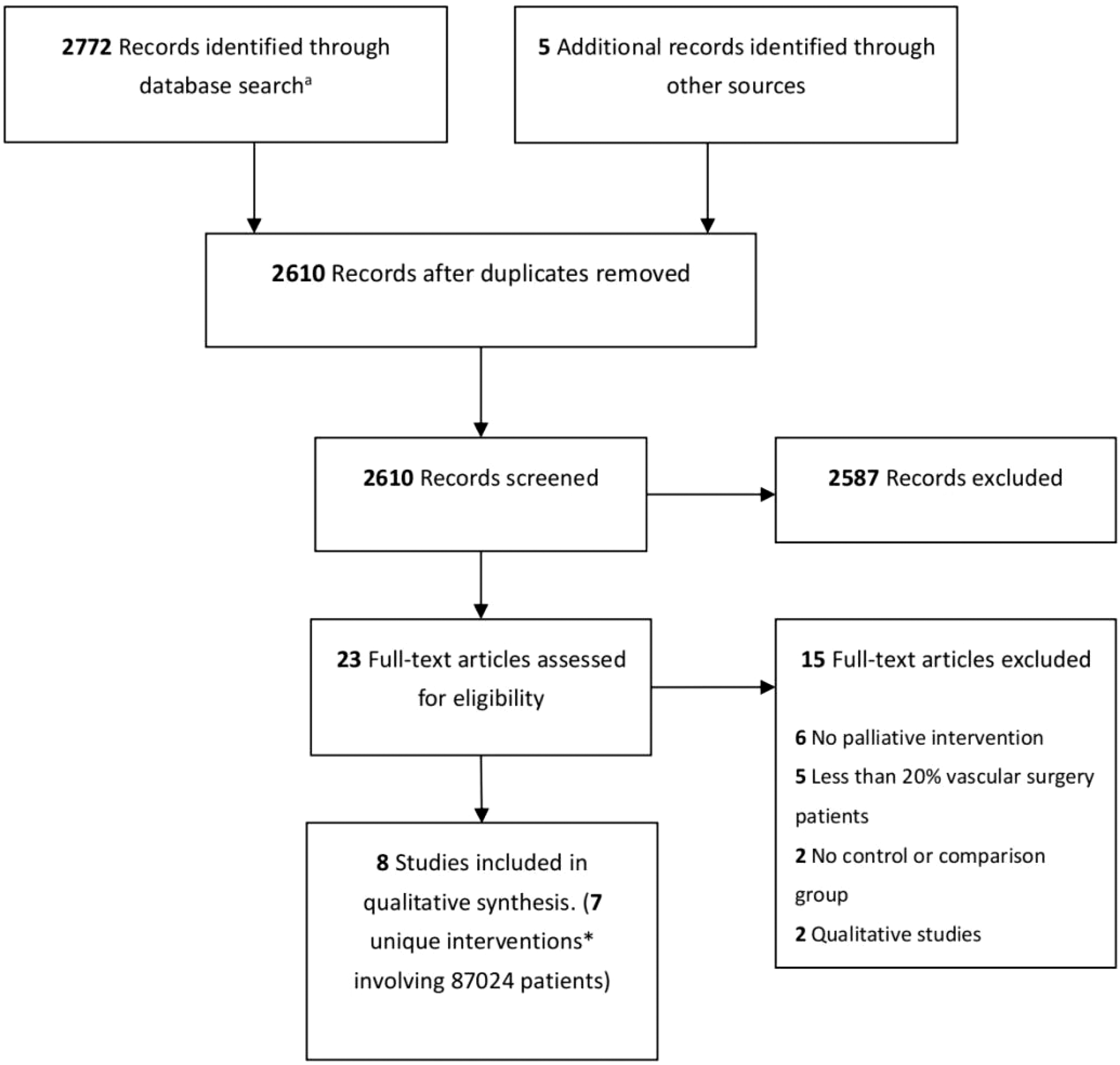
Flow diagram of the literature search. aArticles identified from PubMed (n = 854), EMBASE (n = 387), PsycINFO (n = 9), and Clinical Trials (n = 1522). *Two of the studies were on the same intervention.
Study and patient characteristics
A summary of the eight included studies is presented in Tables 1 and 2. There were six studies from the United States and one each from Canada and Holland.
Study design included: three prospective cohort studies,27–29 one retrospective cohort study, 30 and four retrospective cross-sectional studies.31–34 There were no randomized controlled studies.
The 8 studies included 87,024 patients, with mean ages from 75 to 82 years. The vast majority (95%) of the patients came from two cross-sectional studies.31,32 Of the five studies28,30–33 that reported sex, 59,969 of 86,932 patients (69.0%) were men. Of the three studies31,32,34 reporting race, 59,766 of 83,513 patients (71.6%) were white. Five of the studies30–34 reported that palliative care was, or may be, underused, reporting palliative care rates of 9.3% to 29.9%.
Quality of included studies and risk of bias
Methodological quality of each included cohort study is presented in Supplementary Table S2, showing study design, NOS, 26 and types of bias. Stars awarded range from 0 to 9, with higher numbers denoting higher quality studies. Cohort studies with 6 or more NOS stars were assigned a quality rating of moderate, and studies with 3 to 5 stars were evaluated as low quality. No studies scored less than 3. The studies included in this review ranged from 4 to 8 stars. Selection and performance bias were common, and studies were limited by small sample sizes, nonequivalent comparison groups, and selection and definition of controls. A major limitation of quality was that four of the studies were cross-sectional studies.
Palliative care intervention
The palliative care intervention in five of the studies30–34 was simply whether a palliative care referral or consultation had taken place, with one of these studies 33 also reporting whether family communication on admission had taken place. One study 29 compared minor amputation (toe) and palliative wound care with major amputation (above or below knee) in patients with PAD and foot infection. The intervention of the final study 28 was comparing conservatively with endovascularly and surgically managed CLTI.
Outcome measurements
Pain or symptom burden and QoL were measured in three of the studies.27–29 Barshes et al. 29 reported no reduction in ambulatory status or independence in CLTI patients treated with minor amputation and palliative wound care, in comparison to a 75% and 50% reduction in the control (major amputation) group, respectively. They reported no cases of ascending/systemic sepsis or progressive necrosis in the palliative group, and similar reoperation and mortality between the two groups.
Steunenberg et al. 28 reported that CLTI patients treated conservatively, endovascularly, or with open surgery all significantly gained QoL in multiple domains and health status (HS) at six months following the procedure. Peters et al. 27 reported longer term outcomes for the patients in the Steunenberg et al.'s 28 article, in which they showed that last recorded QoL and HS scores before death did not differ significantly, with the exception of the mental domain in the HS score, from previous scores in any of the three groups. Patients in the surgery group scored higher in the mental domain than the endovascular (p = 0.034) and conservative groups (p = 0.034). 27
Place of death was looked at in one study by de Mestral et al., 30 in which they found the chance of a home death was higher in patients with palliative care referrals. None of the studies reported hospice enrollment, which has been shown to be a marker for EoL care quality in previous studies.35,36
The study by Yefimova et al. 34 was the only article to measure family-reported ratings of hospital care, support, and communication in patients' final months. They found that families of decedents who received palliative care were more likely to rate overall care, EoL communication, and support as excellent.
The most frequently measured outcome, health care utilization, was measured in four of the eight studies,30–33 two of which also calculated cost.31,32 All of the studies found a positive correlation between palliative care and reduction in utilization or utilization and cost.
There were no studies on psychological, spiritual care, or social support.
A comprehensive table of the sources, study design, setting, population, intervention, and results is shown in Table 1. The outcomes measured in each study are presented in Table 2. Study number and homogeneity were not sufficient to meet our predefined criteria, 24 so a meta-analysis was not performed.
Discussion
In this systematic review, we set out to establish what research has been carried out on palliative care interventions for PAD, with a particular interest in QoL, symptom management, psychological and spiritual care, social support, and communication.
We found no randomized controlled studies and that all the existing cohort or cross-sectional design were of low-to-moderate quality.27–34 Of these studies, only four studies recorded any patient-reported outcomes27–29,34—three measuring pain, symptom burden, and QoL,27–29 and one measuring satisfaction of family with care support and communication offered to the patient in the last month of life. 34 The total number of patients in the three studies measuring pain, symptom burden, and QoL was only 218. 29 The study of family ratings of communication, care, and support was larger, at over 1000 patients. 34 All the studies had a high risk for bias, and only two studies30,34 included non-hospital patients. The overall poor study quality has been noted in previous systematic reviews on palliative care interventions in cancer patients 7 and in a systematic review of palliative care for surgical patients. 37
Overall, the majority of studies reported palliative care to be underused; there was an association between palliative care and decreased hospital utilization found in four of the studies30–33 and, generally, palliative care interventions were observed to improve the few patient-reported outcomes that were reported. However, we found little evidence to guide understanding of the use and impact of palliative care services in patients with PAD.
The two fundamental knowledge gap domains are the specific EoL care goals of people living with PAD and the most effective methods of meeting these goals. Due to patients suffering from PAD being more likely to be from a lower socioeconomic background, 21 it is probable that they will have a unique set of EoL care goals—particularly in regard to the social ones. A qualitative article on patients living with PAD awaiting intervention found ongoing struggle for relief from a hard to bear physical, social, and emotional burden, with pain and sleep disturbance being major features. 38 A recent systematic review of pharmacological therapies for management of chronic ischemic pain in CLTI patients, however, found insufficient evidence to make any recommendation of pharmacological agents. 39 These articles did not meet the criteria to be included in our systematic review but highlight the need for further research in this area and the lack of evidence we have for measures currently used to treat pain in this patient group.
This review should be read in the context of the following limitations. Inconsistent literature indexing in the area led to difficulty in identifying articles with the search, which meant that a relatively large proportion of the full texts reviewed were from manual searches and authors' personal collections. This limitation and suggestions for more systematic selection of keywords has been reported in previous systematic reviews on palliative care.37,40 As four of the studies31–34 were retrospective cross-sectional studies from large databases, there is the possibility that patients, in fact, received palliative care interventions from other providers. This would result in palliative care interventions being underreported. Our review is also limited by the inability to conduct a meta-analysis because of heterogeneity in study design, interventions, and outcomes.
Conclusions
We found low-to-moderate quality evidence from nonrandomized studies regarding the use and effectiveness of palliative care for patients with PAD. Before conducting the study, we hypothesized that increased palliative care would result in a better quality of death as a result of less physical, psychological, social, and spiritual suffering; however, there was insufficient evidence to either prove or disprove this theory. Despite proven benefits of earlier integration of palliative care in other advanced diseases, evidence of such integration or its effectiveness is lacking in patients with PAD.
More attention is being paid to palliative care in surgery, and recommendations for future research pathways have previously been made.37,41 However, the palliative care needs of patients living with PAD may be distinct from other surgical patients, as this group often have multiple comorbidities and a high symptom burden. The key questions remaining in this area are the systematic evaluation of palliative care needs; assessment of current facilitators and barriers to referral and integration; patient and medical professional education needs; and the development of a robust method to evaluate patient outcomes.
To address these questions, and pave the way to an integrated, holistic approach to the care of patients with PAD, we propose high-quality research to explore what matters to this group of patients, followed by prospective evaluation of current interventions, adaptation of current strategies, and the development of new ones. Research in this area is urgently needed to enable the integration vascular and palliative care services to provide a parallel service as opposed to a “late transition” from one to the other in their final few days or hours. In addition to helping initiate discussion and collaborative research between vascular surgeons and palliative specialists, we hope that this article will highlight the need for increased funding of this much needed area.
Footnotes
Authors' Contributions
Study design: H.D., D.J.A.S., M.I.B., R.L., M.A.W., L.W., T.W., and J.R.d.S. Data collection: H.D. and R.L. Data analysis: H.D., R.L., and M.A.W. Interpretation of the results: all authors. Writing of the article: all authors. Revision of the article: all authors.
Acknowledgments
We would like to acknowledge Joel Kerry BCs MCLIP and Daniel Park of Leeds Teaching Hospitals NHS Trust Libraries for their assistance designing the search strategy.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.