
Abstract
Background:
Lack of knowledge of palliative care has been identified as a primary barrier to access to care, with a recent survey reporting that Hispanics have the lowest rate of palliative care knowledge compared with other racial/ethnic groups. The purpose of this pilot study was to determine if there were trends toward improved palliative care knowledge after viewing four-minute video of a palliative care patient.
Methods:
We conducted a pre- and posttest pilot study among 50 Spanish-speaking, hospitalized Hispanic patients 40 years old and older in a large public hospital. We used the Palliative Care Knowledge Scale (PaCKS) to assess palliative care knowledge. Two questions measured intention to enroll in palliative care. Paired sample t-tests were conducted to investigate change in PaCKS scores. McNemar's test was used to compare differences in intentions to enroll in palliative care from pretest to posttest. We conducted linear regression analysis to determine factors associated with improved knowledge at posttest.
Results:
PaCKS scores revealed significant improvement in palliative care knowledge following viewing of the video, with scores increasing from an average of 6.4–11.4 at posttest. Intentions to enroll a family member in palliative care increased from 64% at pretest to 64%–98% at posttest. Intentions to enroll oneself increased from 72% to 92%.
Conclusions:
Brief exposure to a relatable role model may be effective in improving knowledge and intentions to enroll in palliative care services. More research is needed to determine if these videos are effective in increasing enrollment in palliative care.
Background
Despite greater health care needs, Hispanics tend to underutilize formal health services.1,2 Many Hispanics, for instance, lack knowledge about hospice and are less likely than White non-Hispanics to use these service.3,4 Hispanics also are more likely to have misunderstandings about hospice care compared to non-Hispanic populations.4,5
Similarly, recent analysis suggests the same barriers exist for Hispanics when it comes to palliative care. The 2018 HINTS survey found significant differences in self-reported palliative care knowledge by ethnic group. While 40% of Whites reported having knowledge of palliative care, only 21% of Hispanic respondents reported having palliative care knowledge. 6 In fact, Hispanics had the lowest rate of self-identified palliative care knowledge of all racial groups. In addition, among Hispanics, 39% of those reporting having palliative care knowledge had actual knowledge in three core palliative care principles. 6 Concerningly, lack of palliative care knowledge has been identified by patients and caregivers as a barrier to home-based palliative care. 7 Anecdotal reports from home-based palliative care providers support this finding; these providers report that some Hispanics referred to home-based palliative care fail to enroll in the care. 8
Available information on palliative care rarely includes diverse populations. In a review of YouTube palliative care educational videos, more than 90% of those appearing in the videos were White. 9 Moreover, simple translation of health information is insufficient to ensure culturally sensitive and appropriate messaging and education. These studies and patient reports accentuate the need for culturally tailored, patient-centered approaches to promoting palliative care health literacy among Hispanic populations.
In recognition of these disparities in palliative care knowledge, several researchers10,11 and national workgroups have called for educational initiatives to improve palliative care awareness. The Institute of Medicine's report on “Dying in America” states the time is right to engage local communities in improving knowledge of palliative care. 12 Specifically the Institute of Medicine recognizes that our society needs to “share stories about end-of-life care experiences that resonate across diverse groups.” 12
Role model stories, theoretically driven stories and videos of real patients, have been shown to be effective in increasing hospice 13 and palliative care knowledge 14 among Black and White community-dwelling older adults. Yet, little is known about their effectiveness in improving palliative care knowledge and intention to enroll in palliative care among hospitalized Hispanics with chronic, life-limiting illness. The purpose of this study was to conduct a pilot test of the effectiveness of a role model video in increasing palliative care knowledge and intentions to enroll in palliative care among Spanish-speaking Hispanics.
Methods
We conducted a pre- and posttest pilot study among 50 Spanish-speaking, hospitalized Hispanic patients in a large, urban, public hospital. This study was submitted to the Institutional Review Board who determined the study to be exempt as it was a benign educational intervention that did not collect identifiable participant information (exemption category 3).
Study eligibility and recruitment
Study eligibility included (1) self-identified as Latino or Hispanic, (2) diagnosed with a chronic life-limiting illness (e.g., cancer or heart, lung, kidney, or liver disease), (3) spoke Spanish as their primary language, and (4) cognitively able to participate. Hospitalized patients were identified by palliative care (before receiving a palliative care consultation) and internal medicine hospital teams and referred to the research coordinator. The research coordinator approached the patient at bedside and provided a study information letter and introduced the study. Patients were asked to identify their primary language to confirm that Spanish was their self-identified primary language. Patients meeting the study eligibility criteria were invited to participate in the study.
Sample size
Based on previous research 14 (cite) conducted among a diverse sample of English-speaking older adults and using two patient role model videos as an educational intervention, we estimated sample size conservatively. With an estimated mean difference of 2.5 (standard deviation [SD] = 5) between pre- and posttest Palliative Care Knowledge Scale (PaCKS) knowledge scores and 80% power, our minimum required number of pairs was 34. To account for missing data and potential of incomplete posttest responses, we aimed for a sample of 50.
Role model video
For the role model video, we interviewed a 66-year-old Hispanic male patient with cancer receiving home-based palliative care. The patient was interviewed alongside his wife. The interview protocol was developed based on two theoretical models: Social Learning Theory 15 that posits that people can learn from those with whom they identify, and the Theory of Reasoned Action, 16 which theorizes that individuals weigh pros and cons before engaging in a new behavior. The video presented a first-person report from a real patient, including information about his family, a brief background on his health, and his and his wife's experiences with and attitudes toward home-based palliative care. We used brief text to define palliative care in one to two sentences. This text was presented along with a voiceover to promote accessibility for those unable to read. The video was condensed to a four-minute synopsis for the purpose of this study.
Study measures
Palliative care knowledge
We used the 13-item PaCKS to assess palliative care knowledge pre- and postvideo viewing. 17 The PaCKS is a valid and reliable instrument and has been successfully used in previous studies of palliative care knowledge.14,18,19 Correct responses were summed for each of the pre-and posttest PaCKS to obtain overall PaCKS scores, with a possible range of scores from 0 to 14.
Intentions to enroll in palliative care
We used two questions to measure intention to enroll a family member or themselves in palliative care (If a family member was extremely ill, I would consider enrolling them in palliative care; If I had a serious illness I would enroll myself in palliative care). These questions have been used in previous research on knowledge and intentions to enroll in hospice 13 and palliative care 14 and have demonstrated sensitivity to change.
Level of acculturation
We measured acculturation using the Brief Acculturation Scale for Hispanics. 20 BASH comprised four items and is a language-based measure of acculturation. Questions ask about primary language used: at home, when thinking, with friends, and in reading material. Responses range from Spanish only to English only. The BASH is a highly reliable and valid instrument, particularly for Mexican Americans. 20
Advance care planning activities
Participants were asked if they had discussed with anyone the care or medical treatment they would want to receive should they become seriously ill in the future (e.g., advance care planning conversation); if they had provided written instructions about their care preferences or medical treatment if they were unable to make decisions themselves (e.g., living will/advance directive); and if they had made any legal arrangements for someone to make decisions about their care or medical treatment if they were unable to make decisions themselves (e.g., a durable power of attorney for health care). They also were asked about their exposure to palliative care, including whether they had ever known someone who had received palliative care or hospice care.
Demographics
We also collected basic demographic information, including age, gender, marital status, religion, income, education, employment, and country of origin. Patients also were asked to list their primary health conditions.
Comments on the videos
We asked participants to tell us what they liked and did not like about the videos. We recorded participant comments verbatim.
Procedures
The research coordinator verbally administered the pretest to each patient. Next, using a tablet, she showed the patient the Spanish language role model video. The video included Spanish language subtitles and voiceovers in Spanish for slides that included text describing and defining palliative care to ensure that reading ability would not interfere with learning from palliative care information presented on the video. At the conclusion of the video, the research coordinator administered the posttest. Any patient questions about palliative care or the video were answered after completion of the posttest. In addition, for those patients requesting additional information about palliative care, the research coordinator provided them with an information sheet after the posttest was completed.
Analysis
We used descriptive analysis to describe the sample, number of patients approached, eligible and agreeing to participate in this study as well as comments participants had about the videos. We also describe the overall PaCKS and intentions to enroll in palliative care item scores. Independent t-tests were conducted to investigate relationships between test scores and participant characteristics. McNemar's test was used to compare differences in intentions to enroll in palliative care from pretest to posttest. Overall change in knowledge was calculated using a paired sample t-test. Finally, we conducted correlation analysis to determine the relationship between education, acculturation, and years in the United States with posttest knowledge scores.
Results
We approached 65 patients for inclusion in this pilot study. Four did not meet eligibility criteria (two did not speak Spanish and two were cognitively impaired), leaving 61 (94%) eligible patients. Among these, three were too sick or too tired, two reported being in too much pain, two were being discharged, and four were not interested in participating. As a result, 77% of patients approached participated in the study. Among these, all were 40 years old and older, with a mean age of 57 (SD = 12.6), with 62% age 50 and older. More than half (58%) were male, and 78% had less than a high school education.
More than half (52%) were married, 18% were single, 18% divorced, and 10% were widowed. Most (74%) reported their religion as Catholic, followed by 18% Christian, and 8% reported having no religious affiliation. Most (68%) were unemployed, with 60% reporting an income <$10,000 a year. Most (78%) were born in Mexico, followed by 10% who were born in Guatemala and 6% in El Salvador. More than 75% of participants had been in the United States for 20 years or more, with an average of 29 years (SD = 13.1) in the United States (Table 1). There was no difference in acculturation level by those born in Mexico versus other countries (p = 0.36).
Participants Characteristics (n = 50)
SD, standard deviation.
The most common health condition reported was cancer (64% of respondents). Half the participants reported that they had engaged in advance care planning conversations, and about a third (32%) reported that they had identified a health care durable power of attorney, while just 18% reported having an advance directive/living will. Self-reported knowledge of palliative care was low, with only 8% reporting that they had heard of palliative care and 4% stating that they knew someone who had received palliative care. Similarly, just 12% reported knowing anyone who had received hospice care (Table 1).
Palliative care knowledge
Baseline PaCKS scores ranged from 0 to 12, with an average score of 6.4 (SD = 3.6). Posttest PaCKS scores ranged from 4 to 14, with an average score of 11.4 (SD = 2.5). Bivariate analysis revealed that there was no significant difference in pretest scores among those who knew someone who had received palliative care or had heard of palliative care compared with those with no exposure to palliative care (t = 0.63, p = 0.53). Similarly, there were no differences in pretest scores among those who had engaged in advance care planning (t = −1.1; p = 0.28), had a living will (t = −0.06; p = 0.95), or a durable power of attorney for health care (t = 0.55; p = 0.58).
Overall analysis of pre- and posttest scores found significant improvement in palliative care knowledge following viewing of the four-minute video, with a mean increase of five in number of correct answers at posttest (t = 10.2; p < 0.001) (Fig. 1).
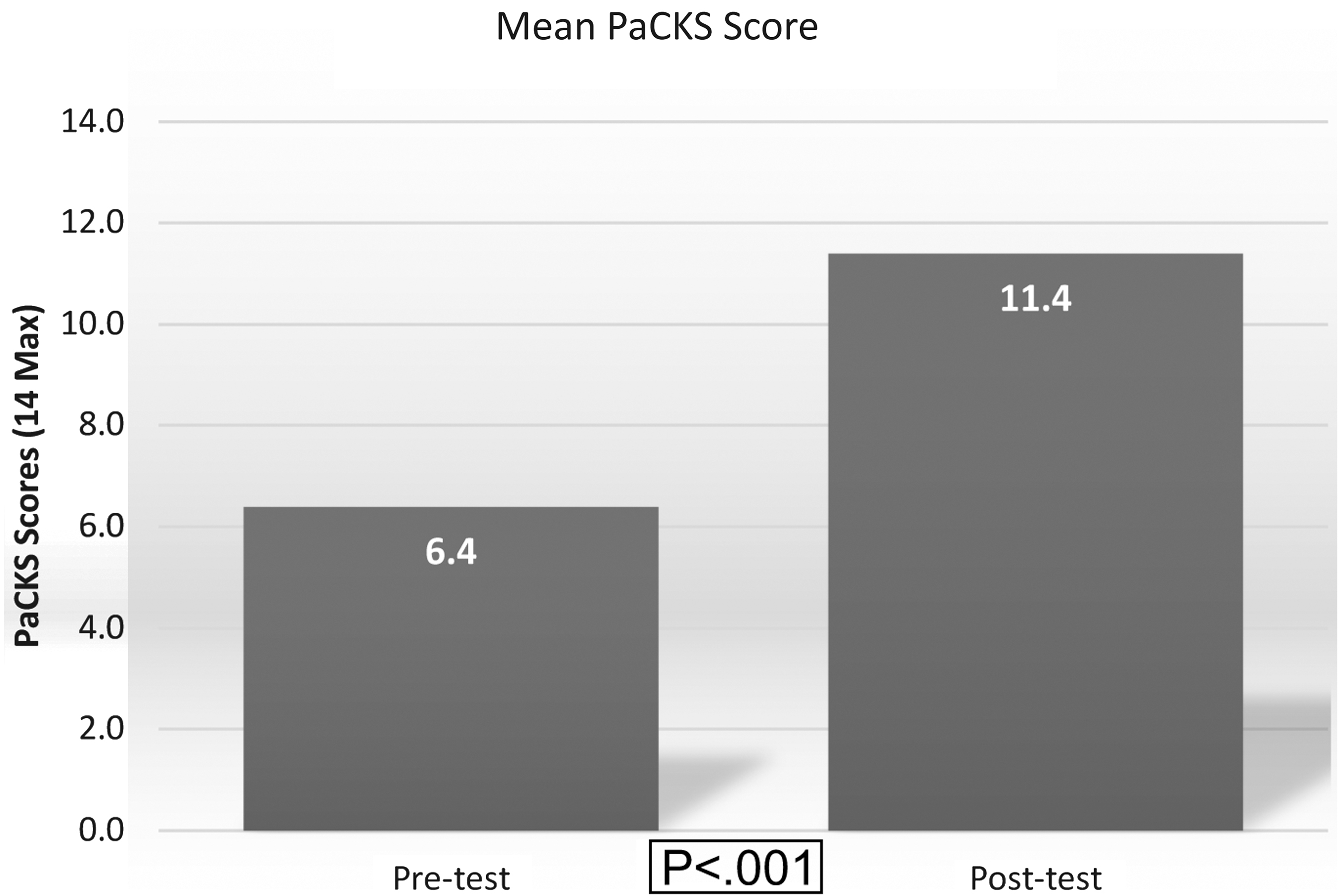
Mean PaCKS score (range 0–14) pre- and posttest (n = 50). PaCKS, Palliative Care Knowledge Scale.
Table 2 contains frequencies of correct responses at posttest. Most frequently missed questions were those stating palliative care is specifically for older adults (60% correct), those with cancer (60% correct), and those in their last six months of life (62% correct) (Table 2).
Palliative Care Knowledge Scale Posttest Frequencies of Correct Responses
PaCKS, Palliative Care Knowledge Scale.
Factors correlated with palliative care knowledge
To examine correlations between age, education level, years in the United States, and acculturation with posttest scores. Results of the correlation revealed that there were no significant association with posttest scores by age (p = 0.23), level of acculturation (p = 0.82), education (p = 0.67), or years in the United States (p = 0.36). Further, we also examined the association between primary medical condition (cancer vs. other condition) to determine if those with similar health conditions as our role model video protagonist had higher posttest scores and found no significant relationship (p = 0.48).
Intention to enroll in palliative care
We found significant differences in intention to enroll both a family member and themselves in palliative care from pretest to posttest. At pretest, 64% agreed that they would likely enroll a family member in palliative care should they have a serious illness. This increased to 98% at posttest (p < 0.001). In terms of enrolling oneself, rates increased from 72% at pretest to 92% at post (p = 0.01) (Fig. 2).
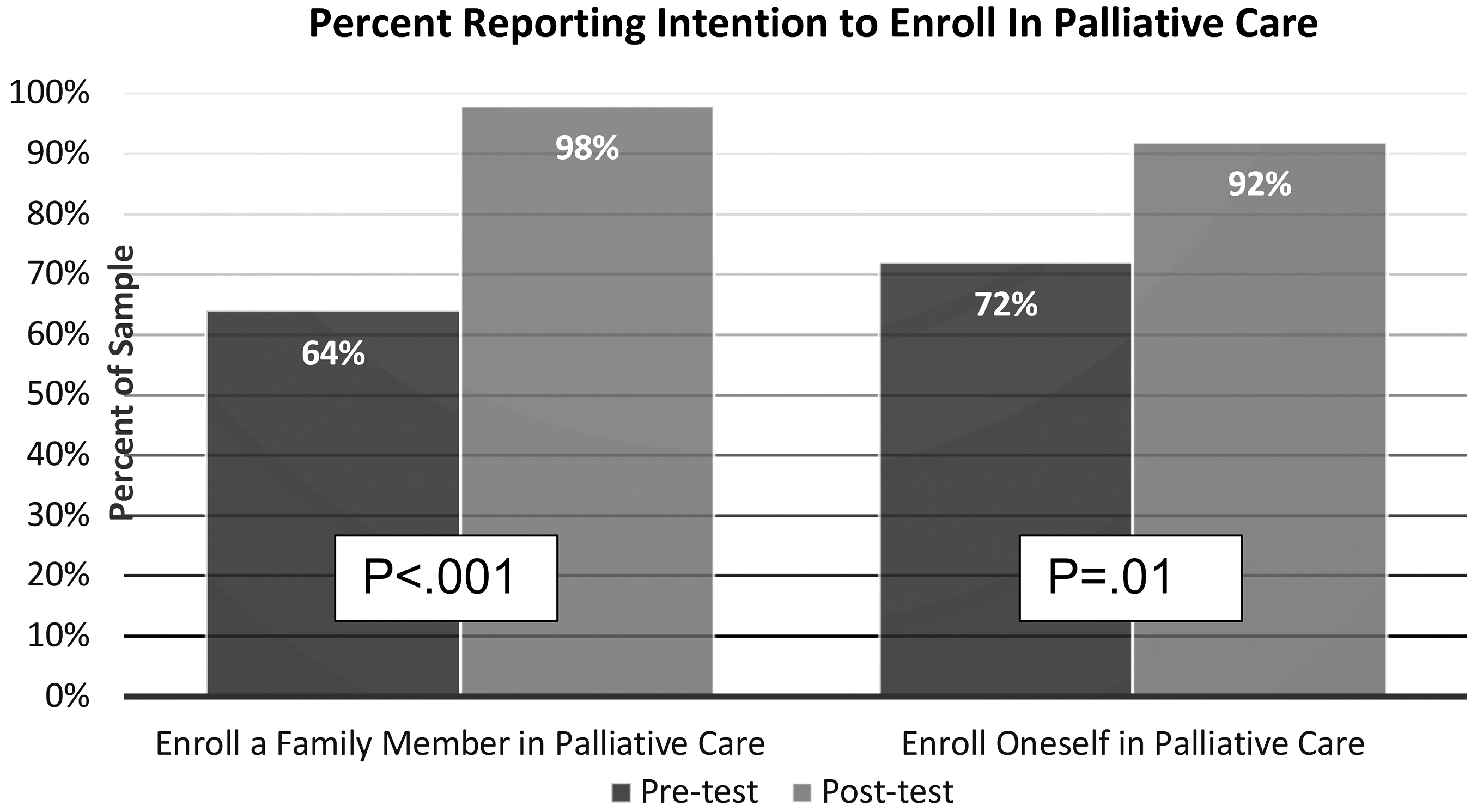
Percent of respondents reporting intentions to enroll in palliative care pre- and posttest (n = 50).
We found no differences in intentions to enroll oneself or family member in home-based palliative care (HBPC) by acculturation level (p = 0.94: p = 0.63, respectively), number of years in the United States (p = 0.72; p = 0.23, respectively), or by country of origin (Mexico vs. other; p = 0.31; p = 0.48, respectively). Those who were Catholic trended toward significance in higher posttest knowledge scores (p = 0.08), while there was no difference in posttest score for those married versus unmarried (p = 0.12).
Participant comments about the videos
Nearly all (n = 49) participants provided positive feedback on the video and just one participant had a negative comment. Positive comments focused largely on the information (n = 12) provided in the video, including the services described (n = 11). Interestingly, about a third commented on the traits of the patient himself, remarking on his “strength,” “courage,” and confidence. Others commented that they liked “everything” (n = 6), the positive outcomes in the video (n = 5), and the ability to relate to the patient (n = 3).
Discussion
Several studies have identified lack of knowledge of palliative care among Hispanics,6,11,21 and this is one of the first studies to examine the effectiveness of a brief intervention aimed at increasing palliative care knowledge among Spanish speaking Hispanics. In a systematic review examining methods for overcoming barriers in palliative care among ethnic/racial minorities, researcher identified just nine studies, and only three of those focused on Hispanic populations. Further, two of three of these studies focused on advance care planning22,23 and the third reported on a patient navigator pilot study that aimed to increase rates of advance care planning, improve pain management, and increase hospice utilization. 24 Thus, none of these interventions was specifically directed toward improving palliative care knowledge.
In our small pilot study, the vast majority referred to the study was eligible, and among these, the majority agreed to participate, demonstrating the feasibility of conducting a palliative care intervention trial among hospitalized Hispanics with chronic, life-limiting conditions. Moreover, the overwhelming number of positive comments made by participants reflect the acceptability of this approach among Hispanics.
Moreover, we found statistically significant improvements in palliative care knowledge. Notably, we found that age, education, and acculturation levels were not correlated with posttest scores, which suggests that use of theoretically driven role model videos may be equally effective in improving palliative care knowledge among those with high and low education and acculturation. This is especially important as previous research has found that those with lower education have lower knowledge of palliative care.6,11 Future studies with larger sample sizes are needed to further explore the relationship between acculturation and palliative care knowledge, while adjusting for baseline knowledge and other socioeconomic variables.
About 40% of participants at posttest believed that palliative care is specifically for older adults and those with cancer. These beliefs may have been due to the fact that we showed participants just one role model video, and that the protagonist in that video was an older man with cancer. This speaks to the need to show patients with more variety in age and disease among role models in future interventions and studies.
Interestingly, 42% of patients believed that palliative care is for people in their last six months of life, despite the apparent good health of the role model in the video and his statement that his nurse describes him to be in “good condition.” Previous research has found that people commonly equate palliative care with hospice,6,7,25 which does have a six-month life expectancy eligibility criterion. Thus, confusion with hospice may have influenced their responses. Alternately, some patients, in particular those referred from palliative care, had been told that they had limited time left to live. This news may also have influenced their perception of palliative care.
Our findings suggest that increasing knowledge of palliative care also was effective in increasing intention to enroll oneself or a family member in palliative care should a serious illness arise, irrespective of years in the United States and acculturation level. This finding is similar to that of Colón 26 who found that acculturation level was not associated with attitudes toward hospice. Our findings of the effectiveness of the role model stories in improving intentions to enroll in palliative care is consistent with previous research demonstrating the effectiveness of role model stories in eliciting behavior change in other public health arenas, including smoking cessation, 27 HIV prevention, 28 and in diet and exercise. 29 Further research is needed to determine if the increase in reported enrollment intentions translate to actual enrollment in palliative care services.
A primary contribution of this pilot study was the effectiveness of such a low-intensity intervention that can be implemented via video in less than five minutes, which speaks to the feasibility of replicating such an intervention in clinical practice. Replication of complex and labor intensive interventions, particularly those without financial incentives, are difficult in health care settings.30–32 The ease of this education effort—provision of a tablet—may facilitate efforts to replicate this approach as well as improve informed decision-making among Hispanic patients referred to palliative care.
While this study was conducted within a hospital setting, it holds implication for physician practice settings as well. Role model videos, such as these, may be shown in physician waiting room areas, or given to select patients to watch in the examination room while they wait for the physician to enter. In addition, these videos can also be shared at Medicare's Annual Wellness Visits, particularly as these visits may signal opportunities for advance care planning conversations for practices and providers. 33 Palliative care providers also can share such videos with perspective patients who are considering enrollment, an important tool given general lack of knowledge and understanding of palliative care experienced by Hispanics. 6
Limitations
This study was conducted among Spanish speaking hospitalized patients within one medical center and thus may not be generalizable to other Hispanics in other U.S. cities. In addition, our small study did not follow patients longitudinally, thus we have no knowledge on the long-term retainment of palliative care knowledge nor do we know if the palliative care knowledge resulted in eventual enrollment in palliative care services. Further research is needed to understand the ability of brief role model stories to impact actual enrollment in palliative care services. Finally, 76% of the samples were from Mexico, thus additional studies are needed to include a broader range of Hispanic nationalities.
Currently, California mandates Medicaid (Medi-Cal in California) managed care programs to provide palliative care to select patients with serious illness, with other states moving to follow.34,35 In addition, increasing numbers of insurance companies also are beginning to offer palliative care programs and services to their beneficiaries.36,37 As these programs continue to expand across the country, it will be important to address ethnic disparities in access to care, particularly those that arise from lack of knowledge of palliative care services. Findings from this study demonstrate that, among Hispanic patients with serious illness, palliative care knowledge and intentions to enroll in palliative care can be influenced through use of role model stories, an outcome that holds widespread implication for palliative care teams, clinicians, and the Hispanic community.
Footnotes
Acknowledgment
We thank the patients who participated in this study.
Funding Information
This work was funded by the James H. Zumberge Faculty Research and Innovation Fund at the University of Southern California. The sponsor had no role in the design, implementation, or reporting of this study.
Author Disclosure Statement
S.E. and S.L. received grant support from California HealthCare Foundation, Patient Centered Outcomes Research Institute (PCORI), and the James H. Zumberge Faculty Research and Innovation Fund at the University of Southern California. S.E. also provided consultation for Independence at Home, a SCAN Foundation Program, and served on the Board of the Social Work Hospice & Palliative Care Network. A.D.S. and C.v.Z. received grant funding from the California HealthCare Foundation. C.v.Z. received grant funding from the Rita and Alex Hillman Foundation. She also provided expert testimony for Manning, Kass, Ellrod, Ramirez, and Trester LL and served on a PCORI-funded Data Safety Monitoring Board.