
Abstract
Introduction:
Our academic ambulatory palliative care program has counseled, monitored, and certified patients for cannabis as part of routine palliative care practice for six years.
Objective:
We describe the population certified for cannabis and policies, procedures, and medicolegal challenges in our palliative care clinic.
Methods:
We performed a retrospective review of patients, qualifying diagnoses for cannabis certification, reasons for referral, and number of annual certifications.
Results:
Between 2015 and 2021, we certified 1711 patients for cannabis. The most common indications were cancer (64%), pain (24%), and neuropathy (9%). Other three months in 2021, 28% of new referrals to our practice were certified for cannabis and 15% of patients were referred explicitly for cannabis certification.
Conclusion:
Despite legal and practical challenges to implementing a medical cannabis program, our palliative care program has fully integrated cannabis as part of our standard outpatient clinical practice.
Introduction
The passage of a 2015 law in Georgia allowed possession of cannabis in the form of low 9-tetrahydrocannabinol (THC) oil (≤5% THC) for patients with select chronic and/or life-limiting illnesses who are certified by a treating physician.1–3 In response, our academic ambulatory palliative care practice began certifying and counseling patients for cannabis shortly after the law was passed.
As a practice, we acknowledged that research on the potential benefits and harms of cannabis in seriously ill populations is in its infancy4–12 ; however, we believed that there was substantial evidence supporting the use of cannabis for the treatment of chronic pain, nausea, and anorexia to warrant open conversations about our patients' current or intended use of cannabis.13,14 We felt it was incumbent on our team to provide guidance and monitoring on our patients' cannabis use to mitigate potential harms.15,16
Descriptive data regarding our patients' perceptions of the benefits and harms of cannabis, as well as concerns regarding access and legality of cannabis, can be found in previous publications.17,18 In this report, we share the qualifying diagnoses for medical cannabis from our patient population certified for cannabis; policies and procedures for what we call our “palliative cannabis consultation” that we believe can serve as a guide for other palliative care practices; and practical guidance for programs seeking to integrate cannabis consultations into their routine practice, highlighting our program's successes and challenges.
Palliative Care Population Certified for Cannabis
Between 2015 and 2021, we certified 1711 patients for cannabis with the most common indications being “cancer, when such diagnosis is end stage or the treatment produces related wasting illness or recalcitrant nausea and vomiting” (n = 1090, 63.7%), “intractable pain” (n = 403, 23.6%), and “peripheral neuropathy, when symptoms are severe or end stage” (n = 65, 8.9%). The remaining patients (n = 65, 3.8%) had Crohn's disease, Parkinson's disease, sickle cell disease, multiple sclerosis, or mitochondrial disease.
The law does not describe objective criteria for “severe or end-stage” neuropathy nor “recalcitrant nausea and vomiting,” leaving the clinician to use clinical judgment when deciding whether the patient qualifies for certification. Certifications have grown over time from 8 in 2015 to a peak of 481 in 2019
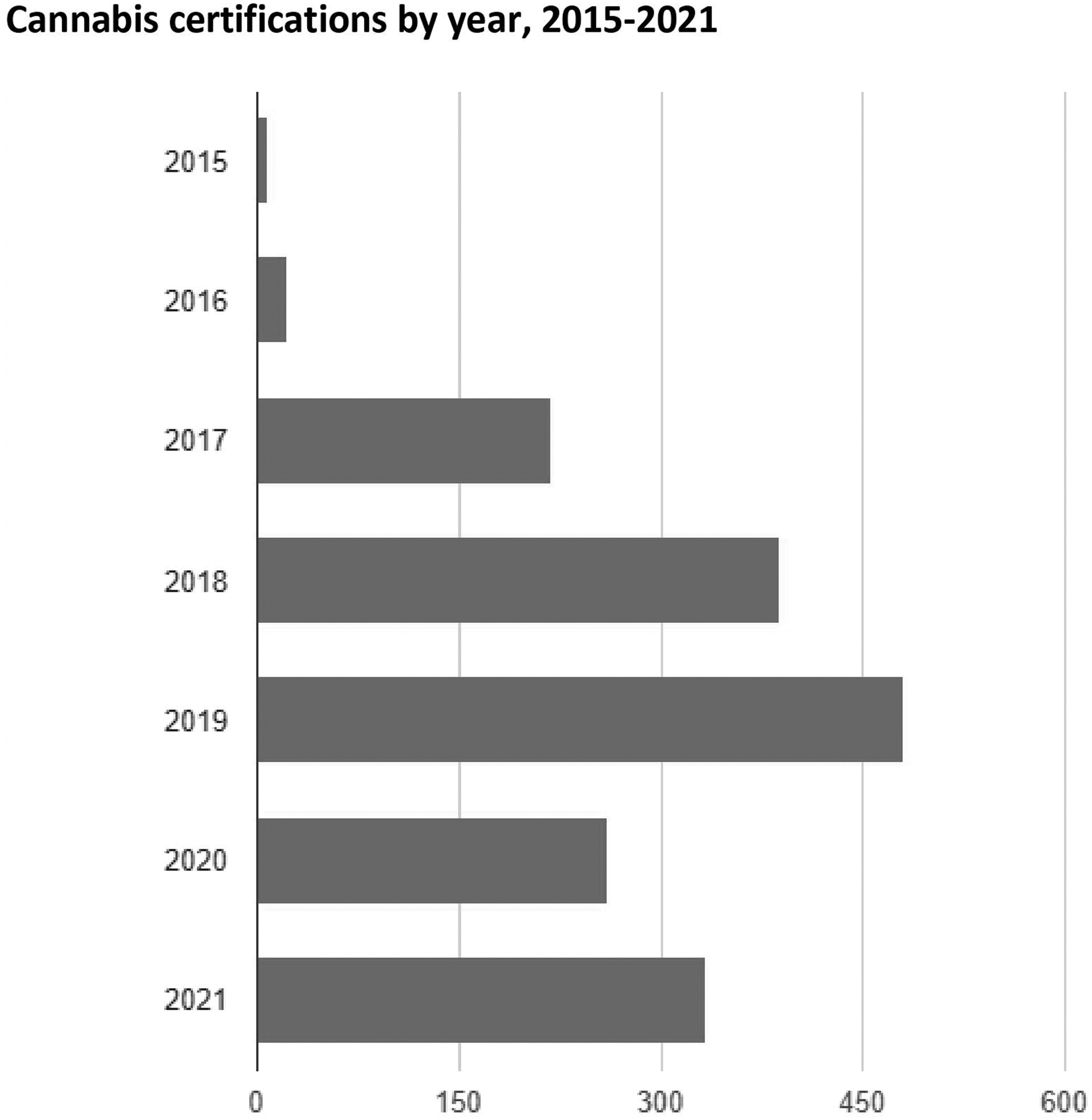
Cannabis certifications by year, 2015–2021. Counts/frequency: 2015 (8, 0.5%), 2016 (22, 1.3%), 2017 (218, 12.7%), 2018 (388, 22.7%), 2019 (481, 28.1%), 2020 (261, 15.3%), and 2021 (333, 19.5%). Between January and October 2021, 333 patients were certified.
We reviewed new referrals to our palliative care practice between July and October 2021 as a snapshot of our patient population
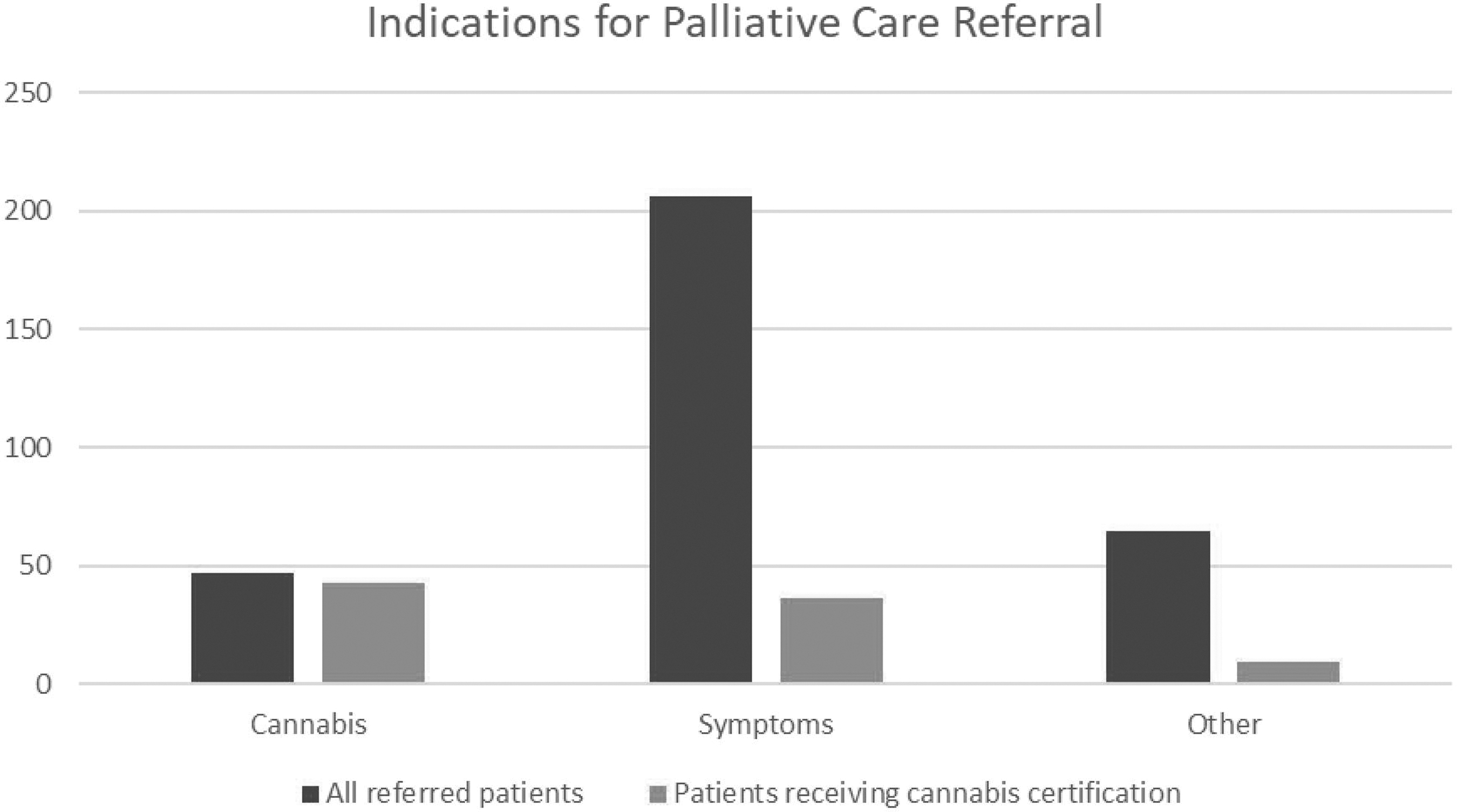
Cannabis certifications based on reason for palliative care referral. Between July and October 2021 (three months total), 318 new patients were seen by our outpatient palliative program. Patients were referred either for symptom management, cannabis consultation, or “other” (diagnosis of a serious medical illness or goals of care). Among patients referred for cannabis certification (n = 47), 91.5% were certified for a card; for symptom management (n = 206), 36 (17.5%) were certified; and for “other” (n = 65), 13.8% were certified.
Patients referred to our practice for certification who were not certified either lacked a qualifying condition, chose not to pursue it after discussion with their physician, or preferred to use dronabinol instead. Among patients referred for symptom management (206), 36 (17.5%) were certified. Nine (13.8%) patients referred for a serious medical illness or goals of care were certified. We certified patients for a low THC oil card by registering them on an online database with the Georgia Department of Public Health that would issue them the card.
“Palliative Cannabis Consultation” Policies and Procedures
To ensure our practice was operating within state law, our clinic staff met regularly with institutional leadership and compliance managers. We initially considered administering a cannabis treatment agreement form,19,20 similar to an opioid treatment agreement form, but learned that this was not in accordance with our state law. Instead, we created an information sheet for patients based on extant literature detailing the policies and procedures of other practices in North America.4,7,20–22 We underscored that cannabis is a Schedule 1 drug per the Drug Enforcement Agency (DEA) and plant-derived cannabis is not approved by the Food and Drug Administration (FDA) as treatment for any condition other than select pediatric seizure disorders.
We addressed risks from cannabis use, including potential negative effects on cognition, motor skills, memory, and respiratory problems.13,23 We discouraged the use of e-cigarettes or other vaping-related forms of cannabis inhalation, as well as use during pregnancy or while breastfeeding. 24 We emphasized that withdrawal could occur if cannabis is stopped after regular use. 15 Table 1 highlights the points that we address during a routine cannabis consultation and includes references we use to inform the conversation.
Topics Addressed during a Routine Cannabis Consultation
Per recommendations from the Food and Drug Administration and the Centers for Disease Control, we do not recommend use of vaped THC or CBD products.47 However, we recognize that our patients may continue to choose to use vaped cannabis for rapid symptom management and thus include this guidance in our consultation.
CBD, cannabidiol; THC, tetrahydrocannabinol.
We provide general guidelines for dosing oral cannabis that generally resemble the way in which we counsel patients on opioid use: start low and go slow to minimize side effects.4,25 This guidance is based on peer-reviewed publications intended to provide practical guidance for clinicians on dosing and administration of cannabis to treat chronic pain.7,15,21,22,26–28 We counsel patients on adverse effects including drowsiness, fatigue, dizziness, dry mouth, anxiety, nausea, and paranoia 25 ; and we ask them to reach out to our clinic about any benefits or harms that they may experience.
Furthermore, we inform patients on a calcineurin inhibitor about potential drug interactions with cannabis formulations containing cannabidiol (CBD). 29 For patients using immune checkpoint inhibitors as part of their cancer regimens, we discuss emerging evidence that CBD may worsen the efficacy of their cancer drug, though we may still certify patients after counseling using a shared decision-making approach.30–32
Successes and Challenges in Implementing an Integrated Cannabis Program into Outpatient Palliative Care
Many of our colleagues outside of palliative medicine have referred patients with chronic and life-threatening illnesses to our clinic specifically for a cannabis consultation, making cannabis a “gateway drug” for palliative care referrals. We consider this study a form of harm reduction as we prefer clinician oversight and input on our patients' cannabis use. A success of this clinic is that we have been able to integrate cannabis into standard clinical care without compromising any of the core components of palliative care delivery.33,34
There are numerous challenges to operating a cannabis consultative arm of a palliative care program. Among them, we have no validated tools to assess whether our patients have a cannabis use disorder (CUD) as current assessments were designed to identify abuse and dependence among users who were not certified to use it medically. 15
To date and to our knowledge, none of our patients have been formally diagnosed with a CUD; however, a significant minority of our patients are concerned about cannabis withdrawal (19%) and dependence (14%). 17 This is consistent with a recent large national survey that found 11% of medical cannabis users met criteria for cannabis dependence based on self-report. 35 Thus, further research is necessary to describe the harms—including risk of dependence and substance use disorder—among patients using cannabis for medical indications.
Another challenge is the lack of a robust evidence base to provide guidance on the benefits and risks of cannabis use, particularly for patients with progressive life-limiting illnesses.12,36,37 Legislation and patient and clinician advocacy have resulted in a system in which physicians are asked to counsel and monitor patients on cannabis therapy without sufficient evidence to guide their recommendations. 38 As practices see more patients earlier in the course of their disease, 39 it is crucial for clinicians to be able to advise patients on both the immediate- and long-term risks associated with cannabis use. We recommend that palliative care programs collect and share real-world data on the demographics and outcomes of their patients who use cannabis.10,16
Finally, our patients frequently report significant improvement in their pain, sleep, appetite, and overall sense of well-being, 17 and their caregivers are often very thankful when our patients feel better. We have anecdotally seen many patients wean off opioids and reduce polypharmacy that we believe warrants dedicated research. Of course, not all of our patients benefit from cannabis, and some report drowsiness, fatigue, weight gain, and paranoia. Based on our often-rewarding experiences working with our patients, we believe further research is warranted to better describe the benefits and harms of cannabis in palliative care populations.
Conclusion
Over six years, our palliative care program has integrated cannabis certification, counseling, and monitoring into our routine practice. Challenges to this study include delivering medical care without a robust evidence base in a constantly changing legal milieu with which we need to remain compliant. Future study includes investment in palliative care-led controlled trials with standardized cannabis products, collection of real-world data, and supporting collaboration between the many ambulatory sites 40 that are engaging with cannabis-related work within palliative care.
Footnotes
Funding Information
This study was supported by an Emory University's Department of Medicine FAME (Fostering the Academic Mission in the Emory Department of Medicine) grant.
Author Disclosure Statement
No competing financial interests exist.