
Abstract
Background:
How children die in pediatric intensive care units (PICUs) has been poorly described, and support for parents during this traumatic experience could be improved. Better information on perceptible signs of the end of life (EOL) in children may help mitigate the trauma.
Objective:
To describe the most common perceptible EOL signs in PICU patients.
Methods:
A prospective study in a PICU. Health care providers observed 28 children expected to die and noted the perceptible signs.
Results:
The most common perceptible signs were desaturation and bradycardia. Twenty-seven patients had at least one change in physical appearance. Gasping was noted in 12 patients.
Conclusion:
Perceptible signs of the EOL were different from those reported in children dying in other units or in adults. Sharing information about signs of EOL with parents may prepare them and enable them to better support their child.
Introduction
In developed countries, child death is rare and often occurs in a pediatric intensive care unit (PICU).1–5 In PICUs, more than half of parents experience complicated grief, 6 which can be made easier with open and honest communication between parents and the medical team. 7 Several reports have suggested that signs that appear at the end of life (EOL) can cause distress in parents8,9 and staff. 10 The American College of Critical Care Medicine suggests that parents should be informed about these signs to help them support their child. 7 Despite extensive literature on EOL care in PICUs, no description of perceptible EOL signs has been published.
The objective of our prospective study was to describe perceptible signs of the EOL in children dying in the PICU with the goal of educating staff about the most common and/or potentially distressing signs so that they can provide better information and support to parents.
Methods
We conducted a single-center, prospective, observational study in a 20-bed medical-surgical PICU in France. The study was approved by the institutional review board of the hospital. The duration of inclusion was set so 30 patients could be observed.
Inclusion criteria were age <18 years, hospitalization in the PICU, and expected to die within five days after withdrawal of life-sustaining treatments (WLST) or treatment failure, which was defined as the probable occurrence of death despite maximum active treatment. T0 (time zero) was defined as the moment when PICU staff informed the parents of the high probability of death. Parents were informed about the study verbally and in writing and had to give their oral consent for participation. Noninclusion criteria were brain death, unexpected rapid death before parents could be informed, inability to inform the parents of the study, parental refusal, and exclusion criteria were child still alive five full days after T0, or child discharged alive from the PICU.
Each child included in this study was observed by the staff from T0 to death. Signs potentially associated with EOL that could be perceived by the parents were drawn up following a review of the literature11,12 and from professional experience in a case report form. The staff recorded whether the signs were present at T0, worsened over time, and/or appeared after T0. Further details on methodology are provided in Appendix A1.
All treatments and invasive devices were recorded at T0 and at the time of death, as well as the presence of the parents during the EOL and at the time of death. Qualitative data (e.g., number of children presenting cyanosis) were described as numbers and percentages and quantitative data (e.g., dose of midazolam) as medians and ranges.
Results
From April 2017 to December 2019, 121 children died in the unit (PICU mortality rate was 3.9%). Twenty-eight of these children were included in this study (Fig. 1). All parents who were approached agreed to participate. One patient who died after being transferred to another unit was excluded.
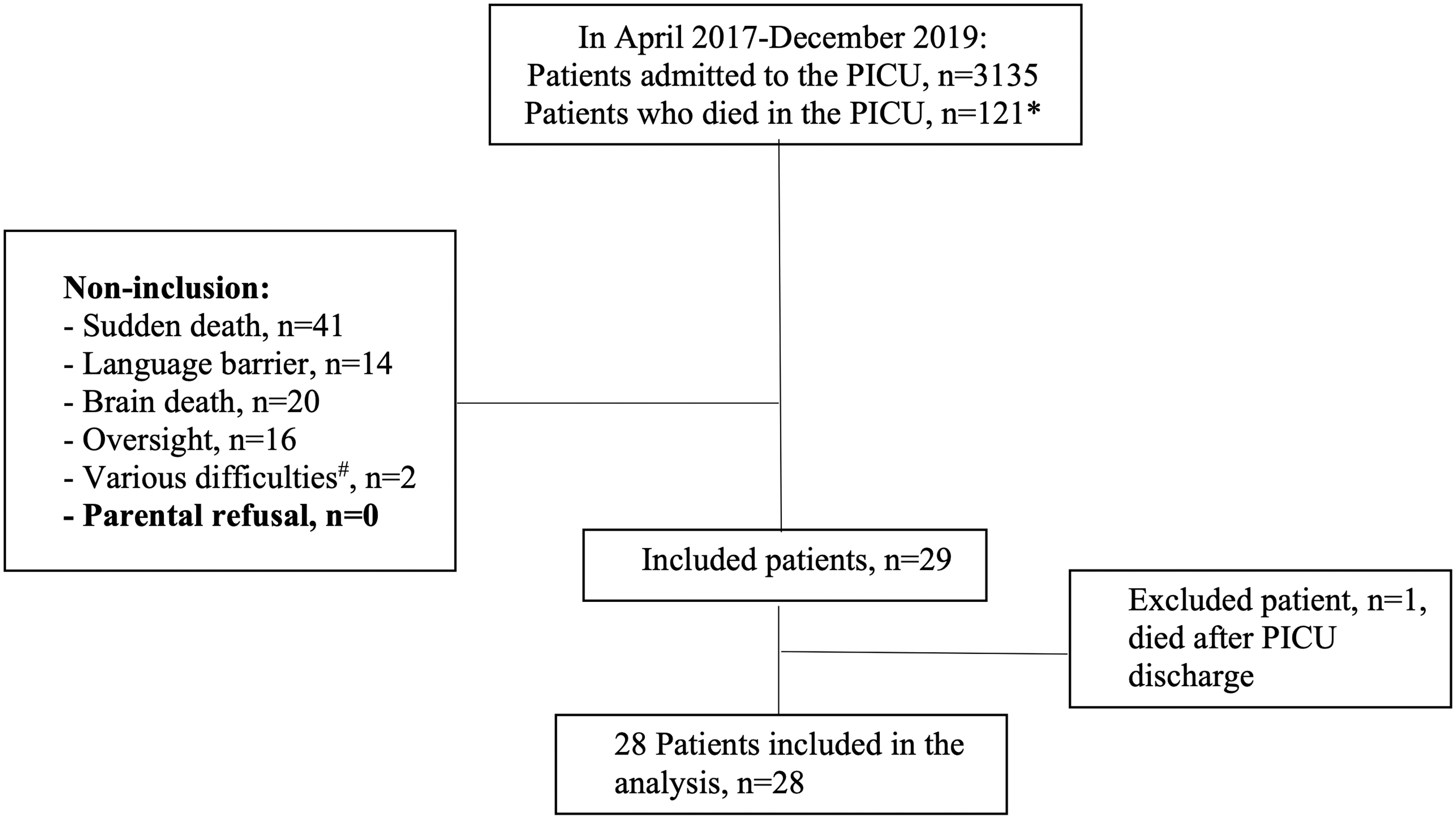
Patient inclusion. *This number does not include the patients who died outside the unit. #For one patient, the parents had a strained relationship with the staff, and it was felt that the level of trust was not sufficient to suggest the study. The other patient died after spending more than eight months in the unit, and the staff felt unable to distance themselves sufficiently to conduct the study.
Table 1 details the main characteristics of the patients, including age, sex, reasons for PICU admission, and cause of death. Table 2 presents perceptible signs of EOL and details the signs present at T0 and signs that appeared or worsened between T0 and death. The most common signs appearing or worsening after T0 were desaturation (n = 21, 8%) and bradycardia (n = 18, 6%), along with changes in general appearance, including pallor (n = 15, 5%), cold skin (n = 13, 5%), cyanosis (n = 12, 4%), edema (n = 11, 4%), and marbling (n = 10, 4%). Pain was present at T0 in 4 (14%) children and remained present at the time of death in 1 child, and there was impaired consciousness nonrelated to sedation in 13 (46%) children at T0 and in 16 (57%) children at the time of death.
Main Characteristics of the Study Patients (n = 28)
Values are given as n (%) or median [range].
Defined using the classification in the ANZPIC registry. 17
Out-of-hospital cardiac arrest, n = 2; inborn error of metabolism, n = 2; syndrome or malformation, n = 1; hypovolemic shock, n = 1.
Cardiac arrest out of hospital, n = 2; inborn error of metabolism, n = 1; hypovolemic shock, n = 1.
LOS, length of stay; PICU, pediatric intensive care unit; WLST, withdrawal of life-sustaining treatments.
Perceptible Signs of the End of Life among Study Patients (n = 28)
Values are given as n (%).
Pain was assessed using the Comfort B or EDIN scale.
Recorded until death in 24 patients.
Recorded until death in 27 patients.
Only 22 patients had their blood pressure measured at T0 and only 1 patient until death.
EDIN, Echelle Douleur Inconfort Nouveau-né, neonatal pain and discomfort scale.
Supplementary Table S1 lists the medical devices, monitoring, and treatment at T0 and the time of death. At least one parent was present for some of the time between T0 and time of death for all patients, and at least one parent was present at the time of death for 25 (89%) patients.
Discussion
This is the first prospective study describing the perceptible signs of the EOL in children dying in the PICU. To obtain a representative population, we used broad eligibility criteria, including neonates and adolescents, postoperative and nonsurgical patients, and patients with and without a decision of WLST. Although we excluded patients who died before the parents could be informed of the study and those with brain death, our population is comparable with other PICU populations described in the literature with regard to mortality rate, age, causes of PICU admission, proportion of patients with chronic disease, and causes of death.11–14 Given that patients with unexpected rapid death or brain death were excluded, the proportion of patients with WLST decisions was high compared with previous studies of patients dying in the PICU (90% vs. 50–70%).11–13,15
Studies reporting EOL signs in adults during the last 15 days of life, 16 studies on the quality of death,17,18 and studies in children1,19,20 have reported different signs than those observed in this study. Patients in this study had a wide variety of medical conditions, many of which required invasive life-sustaining treatments with high doses of sedative analgesics, making it difficult to compare the results with those of other populations.
Few recommendations exist on maintaining or not the cardiorespiratory support during EOL, but they tend to suggest to stop it.7,21 Whether this helps the parents is still debated. This is probably due to the lack of studies on the subject, as well as arguments against and for. Such as the risk for the relatives to be only concerned about the vital parameters rather than the child himself, 7 and the possibly stressful experience of the “scope countdown,” opposed to the reassuring impression of control and knowledge of the precise stop of the heart, and thus of the precise time of death, which is the accepted definition for a major part of the population. The ward where this study was carried out has no protocol on the subject. Some parents were proposed turning off the monitoring, as the monitoring can be turned off in the room and the alarms left on only at the nursing station. However, cardiac monitoring was maintained until death for all patients except one. This allowed parents' access to information on their child's heart rate and/or saturation.
Changes in general appearance were frequent and are easily perceived by the parents, who may feel they no longer recognize their child. Furthermore, changes in physical appearance directly affect the parent–child relationship, as shown in a study on parental physical proximity in EOL care in the PICU, these physical changes may lead parents to distance themselves from their child and experience difficulties in providing closeness, which they may later regret. 22 A study in a neonatal intensive care unit found that nursing staff were also disturbed by changes in the physical appearance of their patients. 10
Gasping was recorded after T0 in half the patients who were not receiving neuromuscular blocking agents at T0 (n = 10/20). Gasping has been shown to cause distress in parents and staff.8,9 Apart from desaturation, there were relatively few respiratory signs in the children in this study, unlike other studies of EOL signs in adults or children outside the intensive care unit.1,23,24 This may be explained by the deep sedation and analgesia in this study group.
Our study has some limitations, as we chose to prospectively inform the parents of the study before the death of their child, and therefore, children who died unexpectedly were nonincluded. However, by definition, the sudden death of a child cannot be anticipated, and parents will not be able to receive information concerning the perceptible signs of EOL. In addition, other methodological biases, such as respondent subjectivity, may have interfered with our results.
Another limitation would be the impact on the expression of the signs perceived during EOL of the child's age, cause of death, treatments used, and other factors. We have tried to minimize them through certain methodological choices described in Appendix A1. However, the aim of the study was to observe the most frequent perceptible signs during EOL in the PICU to anticipate them with the parents. Given the number of patients included, it did not seem feasible and relevant to assign each of the symptoms to a subgroup of patients according to the factors influencing the appearance of the signs.
All parents informed about the study agreed to allow their children to participate. This was unexpected, as informing the parents several hours in advance that death was expected may have heightened their distress, although it also helped them prepare for their child's death. The fact that parents were happy to engage encourages prospective studies of children dying in the PICU.
Conclusion
In this population of 28 children dying in a PICU, the most common perceptible signs of EOL were desaturation, bradycardia, and changes in the general physical appearance. Gasping was also frequent. We know that some of these signs can be distressing for parents, even if the precise impact on parental grief is unknown. Further studies are required to evaluate the impact of EOL signs and giving parents information on EOL signs on parental grief.
Footnotes
Acknowledgments
We thank the Fondation de France for funding our study, the entire team of the Pediatric Intensive Care Unit, and the Dr Guilmin Crepon from the Pediatric Clinical Epidemiology Investigation Center of the Robert-Debré University Hospital.
The study has been performed in the pediatric intensive care units of the Hôpital Robert Debré, Paris, France.
Funding Information
The Fondation de France (Registration No. 00069160) supported this research. The funding source had no role in the design or conduct of the study; the collection, analysis, or interpretation of the data; the writing of the article; or the decision to submit the article.
Author Disclosure Statement
No competing financial interests exist.
Appendix A 1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.