
Abstract

Dear Editor:
Clinically significant depressive symptoms are prevalent in people with advanced life-limiting illnesses and extremely short prognoses (i.e., days to weeks). 1 Nonetheless, management can be challenging due to insufficient time for intervention effects, while co-existing symptom burdens (e.g., fatigue and dysphagia) and organ dysfunctions limit intervention tolerability.2,3 Currently, systematic review evidence for depression interventions in the specific setting of extremely short prognoses is lacking.
We conducted a systematic review to determine what interventions were effective for clinically significant depressive symptoms in people with advanced life-limiting illnesses and extremely short prognoses (PROSPERO registration: CRD42019125119). We searched for randomized controlled trials (RCTs) of nonpharmacological and pharmacological interventions (January 1994–June 2021) using MEDLINE (OVID), PsycINFO, Embase, CINAHL, and CareSearch. Inclusion criteria for studies were ≥18 years old with advanced life-limiting illnesses, extremely short prognoses (absolute survival <2 months or a functional status indicative of ≤4 weeks median survival [e.g., Karnofsky Performance Status ≤40 or Eastern Cooperative Oncology Group Grade 4]), and clinically significant depressive symptoms, defined by a validated depression-specific tool or diagnostic criteria (e.g., Diagnostic Statistical Manual). We excluded studies that were not English language, peer-reviewed, RCT, and studies without clinically significant depressive symptoms in the inclusion criteria for randomization or pre- and post-intervention depression outcome measures. We hand-searched reference lists of systematic reviews and contacted authors for full texts and data. Quality assessment was planned using the Scottish Intercollegiate Guidelines Network Methodology Checklists for controlled trials for individual studies, and Grading of Recommendations Assessment, Development and Evaluation across studies.
Of 6107 screened articles, none met the eligibility criteria (Fig. 1). The primary reason for RCT full-text exclusion related to target population issues (n = 100; 41.3%): 55 did not include extractable data for the subgroup with extremely short prognoses; 11 did not have depressive symptoms in their inclusion criteria during randomization; 33 were excluded due to both reasons; and 1 due to the contentious nature of diagnosing depressive disorder in the dementia population.
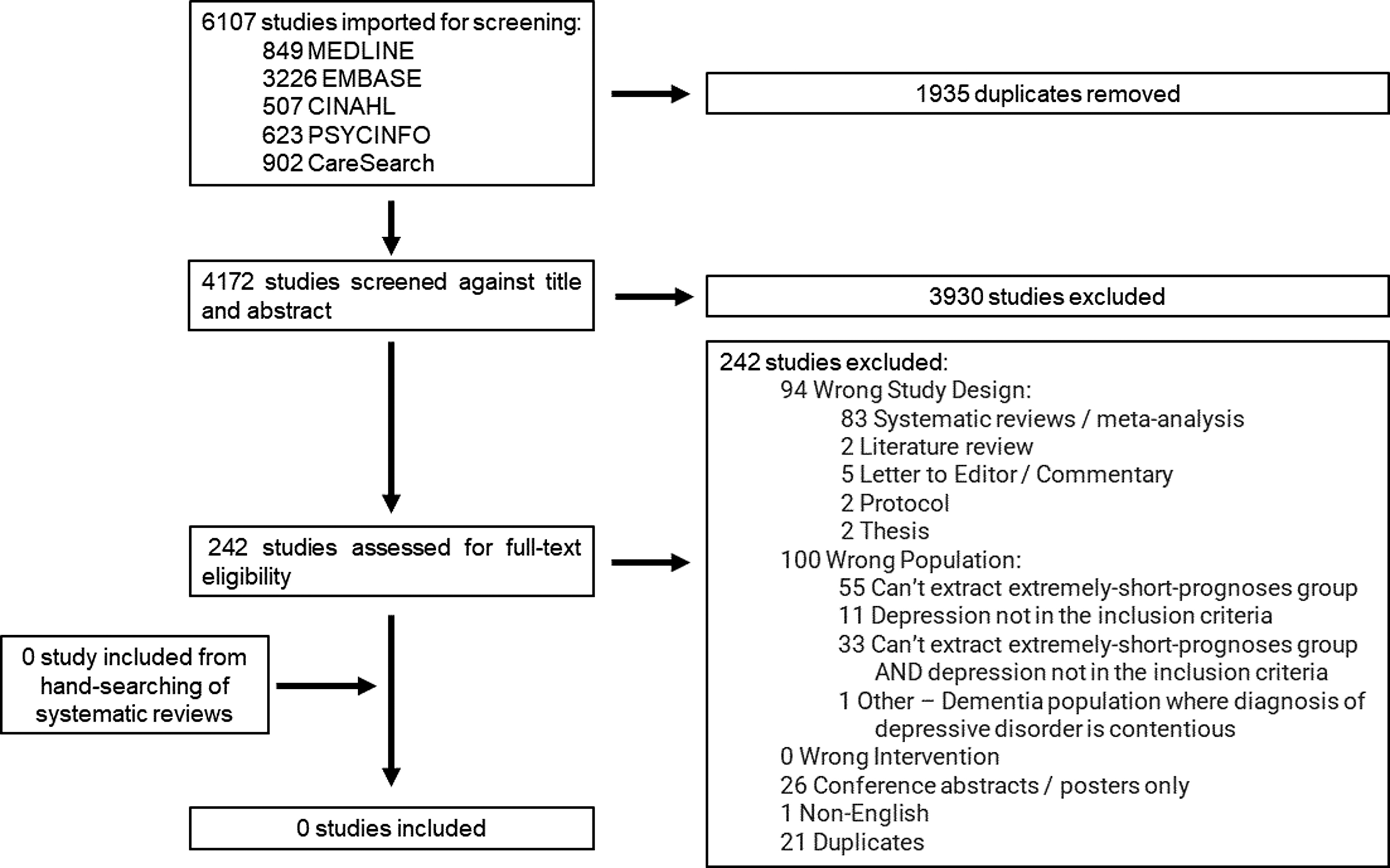
PRISMA flow diagram. Out of 6107 studies identified and 242 studies assessed for full-text eligibility, no study was identified as eligible for analysis.
Our review demonstrates that clinicians do not currently have RCT data to inform the use of any nonpharmacological or pharmacological interventions for depression in patients with extremely short prognoses. Consequently, when considering interventions for depressive symptoms for people in the last days to weeks of life, clinicians should exercise caution when extrapolating data from the broader literature and carefully assess potential benefits and harms after initiating any therapy. 4
Researchers in this field need to consider including and explicitly identifying people with extremely short prognoses and clinically significant depressive symptoms using validated methods before randomization in their studies. To improve the feasibility of generating evidence for this group, researchers may consider alternative trial designs (e.g., n-of-1 or Bayesian response-adaptive randomization). Non-RCT designs can also be considered, using death or set levels of functional status as anchor points, following participants prospectively until death.
Overall, this review highlights the evidence gap for interventions for clinically significant depressive symptoms in the extremely short prognosis setting, and the implications for clinicians and researchers striving to optimize depression care at the end of life.