
Abstract
Background:
Telenovelas show significant promise as a mode of education that could potentially enhance hospice family caregivers' (HFCG) ability to manage distress or pain for themselves and the care recipient.
Objectives:
We sought to understand HFCGs' perceived benefits and challenges of NOVELA using the Levels of Kirkpatrick as a conceptual framework.
Setting/Subjects:
HFCGs from two hospices in the Mid-Atlantic region of the United States.
Measurements:
Semistructured interviews were conducted to understand perceptions of HFCGs on the benefits and challenges of the NOVELA intervention.
Results:
Participants (N = 20) in our study were mainly homebound, well educated, White female, and adult children of people with advanced cancer who reported mild anxiety and moderate self-efficacy at baseline. Three unique themes were identified: acceptability of NOVELA, usability and relevance of NOVELA, and the effect of NOVELA. According to our conceptual model, the intervention positively affects all three adult learning categories: reaction, learning, and behavior.
Conclusion:
Our findings suggest that HFCGs support the proposed NOVELA intervention and it appears to be an acceptable educational tool during hospice care (NCT04533594).
Introduction
Research has shown that hospice family caregivers (HFCGs) have unmet needs for information and skills related to patient care, pain and symptom management, and self-care.1,2 Despite these needs, interventions for HFCGs are rare. 3
Video is an increasingly utilized medium for patient and family education as it provides visual and relatable information that can better capture complex medical and emotional scenarios.4–6 Telenovelas, a form of television drama used widely in Latin American countries, are a creative approach to video education that use storytelling to teach about health. 7 The use of telenovelas in hospice shows significant promise as a mode of education that could potentially enhance HFCG's caregiving ability to manage personal distress or pain for the care recipient.8,9
We have produced a four-chapter telenovela video series, “To Care,” (Fig. 1) as part of a theory-based educational intervention, NOVELA (short for telenovela). 10 Built upon extensive preliminary work, 11 To Care was designed to validate family experiences and identify potential solutions.

Screenshot of To Care. To Care, is a dramatic video that portrays the journey of one hospice family caregivers (standing on the left) as she struggles, while caring for her husband (in bed) who is receiving hospice care (standing on the right) and faces the decision to receive hospice care, manage pain, make health care decisions, and anticipate the dying process. Averaging five minutes, each episode addresses one of these challenges. (Image used with permission from the author.)
Feasibility studies can qualitatively examine participant's reactions to a specific intervention. 12 This study aims to explore NOVELA's feasibility by addressing the following research question: What were HFCGs' perceived benefits and challenges of NOVELA?
Materials and Methods
Conceptual framework
NOVELA was derived from social, cognitive, and self-efficacy theories to explore whether NOVELA increases self-efficacy and decreases HFCG anxiety. 10 To evaluate NOVELA, we modified the Levels of Kirkpatrick13,14 to conceptually frame and synthesize intervention experience and outcomes based on three adult learning categories: reaction, learning, and behavior.
Design
This pilot study used a semistructured interview, following the Levels of Kirkpatrick framework, 13 to evaluate the educational intervention.
Participants
Study participants were HFCGs of patients who were receiving care from one of two hospice sites in the mid-Atlantic United States. Inclusion criteria included the following: (1) HFCGs older than 18 years and (2) access to an Internet device. Exclusion criteria included the following: (1) patients with a Palliative Performance Score of <20% and therefore likely to die within hours or days and (2) HFCGs unwilling to be recorded. After hospice admission, HFCGs who did not opt out from being contacted were referred by hospice staff and contacted by research staff within 48 hours to be screened for eligibility. If eligible and willing to participate, participants completed an oral informed consent and were scheduled for their first intervention visit. The full trial protocol was approved by the Johns Hopkins University Institutional Review Board and is registered at clinicaltrials.gov (NCT04533594).
Intervention
Caregivers met with a trained interventionist through synchronous web conferencing four times over a four-week period, each lasting an average duration of 13.5 minutes (range 8.0–25.7). Participants used a personal web-enabled device (computer, smartphone, or tablet). During the visits, the interventionist introduced the purpose and topic of the video, facilitated video viewing, and then answered questions and reinforced the main messages for each topic.
Data collection and sources
Research staff used a semistructured interview guide (Table 1) to explore participants' experiences with the intervention either at study completion or 14–30 days after their patient's death. For the study period November 2020–June 2021, the exit interviews were conducted from January to June 2021 and all were recorded and transcribed.
Interview Guide Topics and Questions by Kirkpatrick Level
Data analysis
We used thematic analysis in which coding of transcripts involved sorting the data into large-level categories with NVIVO 12Pro. Interview guide topics and questions were used to develop the codebook a priori (available upon request), which comprised 13 unique codes. Exit interviews were coded using a deductive coding approach with a semantic level of interpretation, 15 whereby two team members (K.N. and M.A.S.) independently coded transcripts and suggested additional codes that emerged in the interviews. Peer debriefing, memos, and an audit trail were used to enhance study rigor. Any discrepancy was discussed and addressed to achieve consensus. Codes were grouped and themes synthesized across groups of codes.
Descriptive statistics for HFCG and patient characteristics were computed with SPSS®v2416 using frequencies and percentages for categorical variables, and means and standard deviations for continuous variables.
Results
Caregiver and their care-recipient characteristics are summarized in Table 2. Participants were mostly females (75%), from White/Caucasian race (55%), with more than high school education (65%), and with a mean age of 58 years. Most were taking care of their parent (40%) or spouse (20%). Most care recipients resided in their own home (95%) and had a cancer diagnosis (55%).
Caregiver and Care Recipient Characteristics
Pancreatic and upper gastrointestinal cancer (GI) = liver, gastric, esophageal, carcinoid, etc. Multisystemic = connective tissue disease, ulcer disease, diabetes, multiple contributing conditions.
— = does not apply.
Other race = Hispanic.
Other marital status = separated, divorced, and widowed.
Other relationship with patient = grandchild and grandparent.
Other cancer = breast, colon/rectal/anal, leukemia and fallopian tube cancer.
SD, standard deviation.
Figure 2 presents the flow diagram of participant recruitment and interview completion. Of 47 referrals received from 2 hospice sites, 20 HFCGs consented and participated. Attrition due to death after consent was 4% (n = 2), resulting in 18 participants who received at least 1 intervention session, but only 10 HFCG watched all 4 videos and 16 completed exit interviews. The average length of interviews was 13.21 minutes (range 7.3–32.2). After coding 16 interviews, there was no new information and we considered that saturation; thus, no further exit interview was performed.
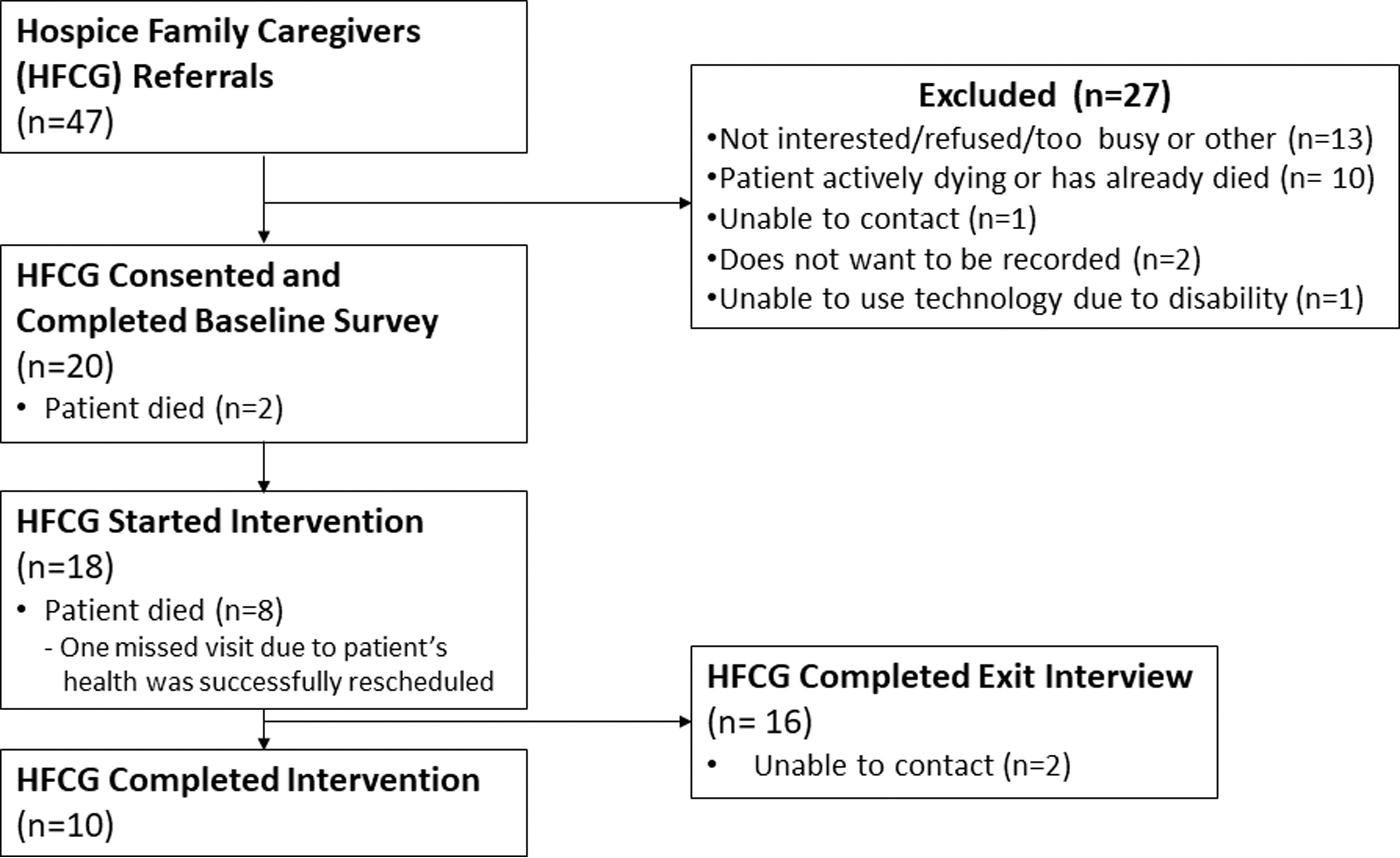
Enrollment, intervention delivery, and exit interview flow diagram. Out of 47 HFCG referrals received from hospice agencies, 20 HFCG enrolled to participate, of which 18 received at least 1 intervention session and 16 completed exit interviews.
Three major themes were derived from qualitative analysis of data: (1) perceptions of NOVELA, (2) relating to NOVELA, and (3) effect of NOVELA. Table 3 highlights principal exemplar quotes by theme and unique code.
Qualitative Findings by Unique Codes
Perceptions of NOVELA
Every participant noted at least one benefit of either the videos themselves or the facilitated discussion that followed. Several shared that they “feel less alone” having watched other caregivers going through similar experiences. Accordingly, they felt the overall intervention reinforced using social support outlets when needed (e.g., hospice provider, family, and friends). Still, several participants highlighted challenges with the intervention, which included the following: technological difficulties, timing in disease trajectory that intervention occurred (e.g., close to patient's death), difficulty finding respite care to complete the virtual meetings, and lack of relevance of videos to the care recipients' condition(s).
Relating to NOVELA
Each of the content areas was important in different ways, but participants indicated they learned the most from the pain management content and discussion. Many participants (n = 14) remembered the content of videos by relating to a particular character. Some caregivers (n = 2) perceived less benefit if they were already experienced caregivers or if the video content did not relate to the disease process of their loved one. “For me, it was being in a really different situation. Because my husband's issue is Parkinson's, and that's cancer.” (Female caring for husband).
Effect of NOVELA
Participants discussed the impact of the intervention on their own perspectives. Several reported changes in attitudes, anxiety, and even modest intention-to-change behavior to engage others in the care of care-recipient. “[…] I'm not sure, except that towards the end, anxiety and worries were not as bad because he had made a decision that he wanted to go on and I was there with them. So, your video was like, ‘make him comfortable, be able to support what's going on, but just make sure the primary objective is to be comfortable’” (Female caring for mother).
Discussion
The purpose of this pilot study was to qualitatively examine HFCGs' reactions, learning, and intention-to-change behavior after NOVELA delivery to explore HFCGs' perceived benefits and challenges. The three themes identified speak to the acceptability (perceptions of NOVELA), practicality (relating to NOVELA), and limited-efficacy testing (effect) of NOVELA, which are three key elements of feasibility studies. 12 Thus, HFCGs' views demonstrated that NOVELA was feasible and acceptable.
Consistent with literature on the acceptability of hospice telehealth visits,17–21 HFCGs' experiences with telehealth visits in our study were generally positive in terms of reaffirming their caregiver role and social support needs, but technology was a challenge. However, overall caregivers were able to adapt to the use of technology for the delivery of the intervention.
It was hard for participants to distinguish which changes were elicited by study participation and which changes resulted from just being a caregiver or from receiving hospice care. A study with palliative patients and caregivers reported that participants found it helpful to talk about their experience with nurse coaches. 22 Likewise, our study showed that interactions with the interventionist motivated HFCGs to share their struggles and inspired them to enact certain behaviors. Further study is needed to explore the impact of NOVELA components on HFCGs, hospice providers' perspectives on its implementation, and ultimately care recipients' health outcomes.
This study has notable limitations. The sample size was small, which was appropriate for a feasibility study. However, data saturation was reached during data analysis, despite the small sample size. 23 The study design employed limited evaluation to some aspects of feasibility and acceptability, not efficacy of NOVELA. The sample was mainly White females, which decreases the generalizability of our results. However, our sample characteristics reflect demographics often displayed in family caregiving studies 21 and for hospice in general. 24 Finally, the interviews were conducted by the interventionist and social desirability bias may have led to less discussion of challenges or criticism of the experience.
Conclusion
HFCGs play a vital role for care recipients at the end of life, yet are sorely underrepresented in hospice-related research. Results from our analysis reveal that NOVELA appears to be a promising and acceptable educational tool for HFCGs. They also underscore the unique challenges of this population, which has been noted at length in existing literature. Further exploration of NOVELA among diverse HFCGs will be invaluable for supporting their needs and health outcomes of care recipients.
Footnotes
Authors' Contributions
All listed authors have sufficiently and significantly contributed to this study and to the preparation of the article.
Disclaimer
The content of this report is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Acknowledgments
We would like to thank Gilchrist Hospice, Seasons Hospice, and their family caregivers for their participation in this project.
Funding Information
Research reported in this publication was supported by the National Institute of Nursing Research (5U2CNR014637-09) through the Palliative Care Research Cooperative (PCRC) pilot project award.
Author Disclosure Statement
No competing financial interests exist.