
Abstract
Background:
The COVID-19 pandemic created surges of rapidly deteriorating patients straining health care necessitating the evaluation of novel models of palliative care (PC) integration to reduce patient suffering and hospital strain.
Objective:
To evaluate an integrated PC model's effect on code status change.
Design:
This is an observational retrospective study.
Setting:
Urban quaternary referral center in the southeastern United States from April 6th to August 20th, 2020.
Patients:
All patients admitted to our medical intensive care unit and stepdown unit were diagnosed with COVID-19.
Measurements:
Code status change, multivariate regression on patient characteristics.
Results:
In total, 79.7% (98/123) patients were full code at admission. After PC consultation, 33.3% (41/123) patients remained full code, 13.0% (16/123) were do not resuscitate (DNR), and 53.6% (66/123) changed to DNR/do not intubate (DNI). An ordinal logistic model determined that consultation location (odds ratio [OR] 3.35, p = 0.017) and patient age (OR 1.09, p < 0.001) were predictive of code status change to DNR/DNI.
Conclusion:
Within an integrated PC model, PC consultation was associated with code status change. The effect of an integrated PC model warrants further study in comparison with a traditional PC model in a similar patient cohort.
Background
The SARS-COV-2 that caused the COVID-19 pandemic has created surges in demand for health care services, including palliative and end-of-life care.1–3 Because of its morbidity, mortality, and potential for rapid clinical decompensation during the first wave of the pandemic, COVID-19–related hospitalizations necessitated early goals-of-care (GOC) discussions with infected patients.4–9 Prior studies advocated for appropriate palliative care (PC) utilization, particularly in high-risk patients. 5 The majority of literature on the impact of PC focused on the need for PC to partner in the care of COVID-19 patients, however, few articles provided guidance on how PC can optimally partner with COVID-19 teams.5,10
Our institution developed an integrated model that encouraged primary teams to proactively consult PC for patients at risk of COVID-19 complications. In this integrated model, all COVID-19 admissions during the first wave of the pandemic triggered a joint decision-making process with the primary team determining collaboratively with a PC specialist whether a formal PC consultation was indicated. Our goal was to retrospectively review the demographics, patient characteristics, and outcomes of COVID-19 patients admitted to our institution in our step-down unit and medical intensive care unit (MICU) who received a PC consultation through this integrated PC consultation model.
Methods
This retrospective study included all consecutive adult admissions with confirmed COVID-19, defined as a positive reverse transcription polymerase chain reaction (RT-PCR) SARS-COV-2 nucleic acid test, who received a PC consultation and were hospitalized between April 6th and August 26th, 2020, at an urban, quaternary care academic medical center located in the southeastern United States. Our institutional review board approved the study and waived the need for informed consent. No funding was procured for the creation of this study. Deidentified demographic data were collected from the electronic medical record (EMR) and stored in a secure password-protected REDCAP database.11,12
All PC consultations generated during the inclusion period resulted from a collaborative phone or web-based conference between the PC team and either the primary MICU-based critical care team or stepdown unit-based hospital medicine team. PC consultation was encouraged for all patients at higher risk of COVID-19 complications including but not limited to age ≥70 years, frailty, presence of organ transplant, chronic lung disease, active malignancy, end-stage heart failure, liver disease, renal failure, dementia, or residence at a long-term care facility.
The primary outcome was to determine which patient characteristics if any were associated with a change in code status after PC consultation. In addition, patient characteristics were collected including demographics, comorbidities, time to PC consultation, hospital length of stay (LOS), discharge disposition, and functional status at time of admission, measured by Eastern Cooperative Oncology Group (ECOG) score.
Code status was defined as “full code” [pursue all life-sustaining treatments (LSTs) including intubation and cardiopulmonary resuscitation (CPR)], “do not resuscitate (DNR) only” [pursue all LSTs excluding CPR], “do not resuscitate/do not intubate (DNR/DNI)” [forgo CPR and intubation], or “unknown.” Patients with an “unknown” code status were treated as “full code” unless a new code status order was entered into the EMR.
All statistical analyses were performed on Stata version 16.2. Descriptive analyses were conducted. The Kruskal–Wallis/Wilcoxon rank sum test and Pearson chi-squared/Fisher exact test were performed to compare continuous or categorical variables by groups as appropriate. A multivariate ordinal logistic regression model was also fitted to determine which variables were associated with code status change. The covariates in our regression modeling were age, location of consultation, ECOG, presence of chronic lung disease, presence of “other” diseases, presence of chronic neurological disease, and number of comorbid conditions. “Other” disease included patients with immunocompromising conditions, organ transplants, and immunosuppressive medications. An example of our data extraction survey can be found in the Supplementary Data.
Results
A total of 123 patients were identified during the study period. As described in Table 1, the median age was 71.2 (range 33–97). Sixty-four percent (79/123) of patients were white, 22% (27/123) were black, and 8% (10/123) were Hispanic. Eighty-eight percent (108/123) spoke English as their primary language and 10.6% (13/123) spoke Spanish. Table 2 shows seventy-nine percent (98/123) of admitted patients were identified as full code on admission. In total, 2.4% (4/123) patients were DNR and 17% (22/123) were DNR/DNI. After PC consultation, 57 patients changed their code status from full code as shown in Table 3. Thirteen patients changed their code status from full code to DNR, and 44 patients changed their code status from full code to DNR/DNI.
Demographics of 123 Patients
Clinical Characteristics of 123 Patients
Other comorbidities included history of spinal cord injury, quadriplegia, tetraplegia, paraplegia, history of organ transplant (kidney, lung, heart, and liver), chronic tracheostomy/percutaneous endoscopic gastrostomy tube dependence, history of rheumatological conditions on immunosuppressives, HIV/AIDS, intellectual disability, and hypothyroidism.
DNI, do not intubate; DNR, do not resuscitate; ECOG, Eastern Cooperative Oncology Group; LTC, long-term care.
Outcomes
PC, palliative care.
Table 4 shows in total, 30.9% (38/123) of patients died while inpatient, with 71% (27/38) of the deceased patients presenting initially as full code. Of these 27 patients who were initially full code, after PC consultation, only 3 patients remained full code at the time of death. Of the 38 patients who died while hospitalized, 39% (15/38) died in the stepdown unit, and 61% (23/38) died in the MICU. Of the 15 patients located on the stepdown unit, 14 changed their code status from full code to DNR/DNI after PC consultation and 1 changed their code to DNR. Of the 23 patients who died in the MICU, 12 arrived intubated on a ventilator, and after PC consultation, only 3 remained full code.
Outcomes of Deceased Patients
MICU, medical intensive care unit.
Results of multivariable ordinal logistic regressions are shown in Table 5. Patients who were admitted to the MICU at the time of consultation had an increased odds of a code status change (OR 3.35, p < 0.05). Age (OR 1.09 for every year >33 years, p < 0.05) and patients with chronic lung disease (OR 3.74, p < 0.05) were also associated with an increased odds of changing code status. Age (OR 1.09 for every year >33 years, p < 0.05) was also associated with an increased odds of changing code status with chronic lung disease trending towards statistical significance (OR 3.74, p = 0.053). Chronic neurological disease (OR 0.214, p < 0.05) was the only characteristic associated with a decreased odds of code status change. ECOG score at admission directly correlated with median time to PC consultation with higher ECOG scores being associated with a later PC consultation (ECOG 2: 2 days, ECOG 3: 2.5 days, ECOG 4: 4 days, p < 0.05).
Results of Multivariable Ordinal Logistic Regression Model
MICU patient location: stepdown floor is the reference group (binary).
Age: 33 years is the reference group (continuous).
Chronic lung disease: no chronic lung disease is the reference group (binary).
“Other disease”: no “other disease” is the reference group (binary).
ECOG: 2 is the reference group (categorical with three values).
No. of comorbid conditions: 0 is the reference group (continuous variable).
Chronic neurological disease: no chronic neurological disease is the reference group (binary).
We noted a statistically significant association between patient characteristics and time to PC consultation in Figure 1. Patients who were full code with a longer time to PC consultation and an inverse association between age and time to PC consultation. Increasing age was associated with earlier PC consultation time. Patients in the MICU had a longer time to PC consultation (t = −3.87, p < 0.05) than stepdown unit patients. Differences in gender, marital status, religion, race, residential facility (RF), or insurance were not associated with code status outcomes.
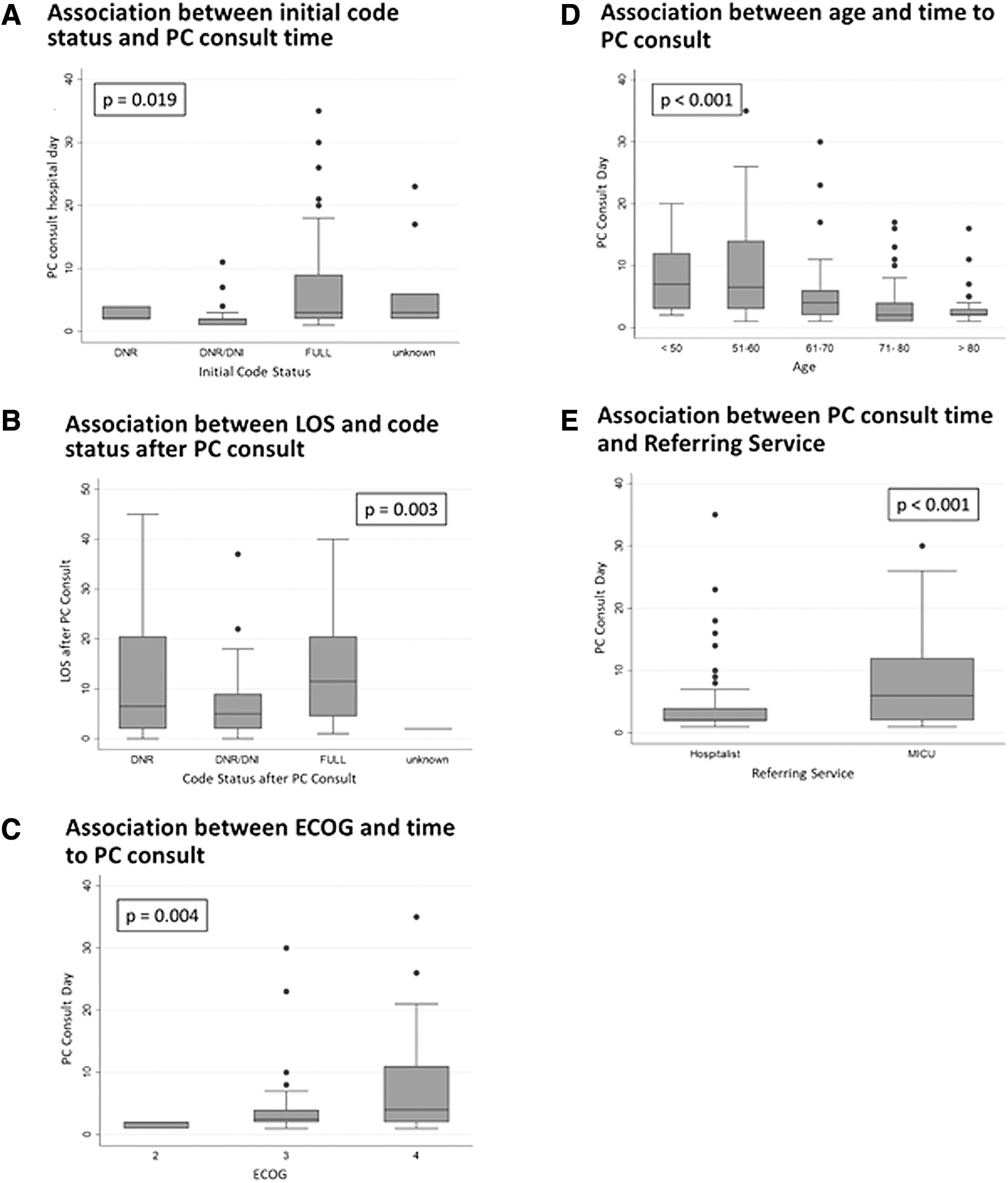
Secondary analysis. Box plots with p values are displayed showing the association between
Discussion
In our retrospective review, PC consultation was associated with a 51.8% (43/83) transition from full code to DNR or DNR/DNI status. PC consultation reduced resource utilization as evidenced in patient mortality with only 3 of the 38 deceased patients remaining full code. Most significantly, 14 of the 15 patients on the stepdown floor changed their code status to DNR/DNI and 1 of the 15 patients changed code status to DNR before the time of death resulting in improved goal-concordant care and resource utilization. Patients who received PC consultations while in the MICU had the highest odds to change their code status to DNR/DNI.
Older patients tended to get PC consultations earlier in their admission than their younger counterparts, with 29.7% of patients (33/111) presenting from nursing RFs, and 90.7% (30/33) of RF inhabitants >61 years of age. Median time to consultation was shortest for those patients in the 71–80 years of age group. This is not surprising, as age was a trigger for referral to PC given the evidence age plays in poorer outcomes, and older patients are found disproportionately in RFs.13,14
Multivariable regression modeling found an association between code status change from full code to DNR or DNR/DNI with patients who had chronic lung disease, increased age, MICU consultation location, and “other” diseases. When reviewed, 31.7% (20/63) of patients with “other” diseases were on immunosuppressive medications for solid organ transplants or for rheumatological conditions, with the next largest percentage 15.9% (10/63) associated with patients experiencing spinal cord or brain injuries, and chronic debility with 80% (8/10) presenting from nursing facilities.
Interestingly, a higher ECOG score and initial admission to the MICU delayed PC consultation. Chronic neurological illness was protective against code status change to DNR/DNI. We suspected patients with chronic illness tolerate a worse quality of life, and patients with impaired functional status required family members to be coordinated to discuss GOC.
From our literature review, this is the first study to use multivariate logistic regression to examine variables associated with a code status change. It is important to note that this study was a retrospective review of patients who required hospital admission for COVID-19 infections early in the pandemic from a single institution in the southeastern United States. It is, therefore, difficult to generalize our findings to other institutions across the country and across all severity of COVID-19 infections. In addition, advances in therapies, including vaccination, continue to occur and may impact those patients affected by this pandemic. Our study also lacked a control group to compare the effect of an integrated versus traditional consultation model.
Conclusion
The impact of an integrated approach warrants further study in comparison with a traditional PC model in similar patients to determine whether an integrated model is more effective at changing code status and decreasing LOS. As this pandemic continues for an unknown duration, our longitudinal findings may provide insight into how PC can be appropriately utilized to effectively meet the demands of future patients with COVID-19.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.