
Abstract
Context:
Parkinson's disease (PD) is the second most common neurodegenerative disorder worldwide. Oral medications for control of motor symptoms are the mainstay of treatment. However, as the disease progresses, patients with PD may develop dysphagia that prohibits them from safely taking oral medications. Currently there are no clinical guidelines for managing distressing motor symptoms in patients with PD and severe dysphagia, which can therefore be quite challenging.
Objectives:
To provide an exhaustive summary of current literature on pharmacological interventions for patients with PD who do not have safe oral access in managing distressing motor symptoms. Indication, route, doses, frequency, outcome, and adverse effects will be discussed.
Methods:
A scoping review using Medline, Embase, CENTRAL, CINAHL, AgeLine, and PsycINFO databases (1946–2021) was conducted. Articles examining patients with PD and dysphagia who are eligible to receive palliative care or at end of life were included. Studies that included patients who were also on oral PD medications or received device-aided therapy were excluded from this review.
Results:
A total of 3821 articles were screened for title and abstract, 259 were selected for full-text review, and 20 articles were selected for data extraction. These included five case reports, one retrospective cohort study, one book chapter, and 13 narrative reviews. There are very few articles addressing the issue of treatment of patients with advanced PD who are unable to take oral medications. Although rotigotine patch and apormorphine injections are most frequently recommended, there are no clinical trials in this patient population to support those recommendations.
Conclusion:
This study highlights a need for further research examining the efficacy and dosing of nonoral medications in advanced PD with dysphagia.
Introduction
Parkinson's disease (PD) is the second most common age-related neurodegenerative disorder after Alzheimer's disease, affecting ∼6.1 million people worldwide. 1 Currently, there are no disease modifying therapies available for PD.1,2 Therefore, management of PD and associated symptoms is largely supportive in nature. 2
The primary features of PD are motor symptoms such as bradykinesia, resting tremor, rigidity, and postural instability, which become progressively more disabling over an average of 15 years. 3 Oral carbidopa/levodopa remains the mainstay of treatment for management of motor symptoms in PD. Although numerous medications have been developed in recent years, none is more effective than carbidopa/levodopa, and almost all are available exclusively in oral formulations. 4 At the final stages of the PD, all medications become less effective due to decline of dopaminergic neurons in the substantial nigra as well as a progressively lower capacity to store and convert exogenous dopamine. 5
Dysphagia occurs in up to 95% of patients with PD and, in advanced disease, may prohibit the intake of the oral medications that patients require to control their motor symptoms.6,7 While more invasive interventions including a nasogastric tube placement or percutaneous endoscopic gastrostomy are available to ensure continuity of medication delivery, these are often not concordant with patients' goals of care with advanced disease or at end of life (EoL). In some cases, oral intake is restricted at EoL due to concordant medical issues such as bowel obstruction or altered level of consciousness. 8 In the absence of medication, uncontrolled motor symptoms can cause significant distress and disability.9–12
Alternative formulations to conventional oral medications have been developed: transdermal rotigotine patch, subcutaneous apomorphine, and rectal carbidopa/levodopa to name a few.13–15 Importantly, none of these medications were developed for use in the setting of dysphagia; rather as an adjunct or alternative to oral carbidopa/levodopa when motor symptoms are inadequately controlled. 16 The rotigotine patch has been widely studied and has shown its effectiveness when used in addition to oral medications in advanced PD.16,17 Device-aided therapies such as deep brain stimulation (DBS) and levodopa-carbidopa intestinal gel (LCIG) are treatments that do not rely on oral medications, but they are invasive and not suitable for a patient at EoL.4,14
Palliative care seeks to provide comfort, treat symptoms, and enhance quality of life. In the PD population, managing distressing motor symptoms can be challenging, particularly when the use of standard medications is limited by dysphagia. Despite the high motor symptom burden experienced by patients with advanced PD and the high rate of severe dysphagia, there are currently no evidence-based guidelines for treating motor symptoms in patients with end-stage PD and severe dysphagia. The existing guidelines use only expert consensus. In the absence of identifiable clinical guidance for this patient population, we felt a scoping review was warranted.
Objectives
The objective of this scoping review is to explore and provide an exhaustive summary of the current literature on existing noninvasive pharmacological interventions for patients with late to end-stage PD with motor symptoms without safe oral access. By summarizing the current literature, we can offer an evidence-based guidance in palliative care management for these patients and identify gaps in the current literature to inform future studies.
Methods
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews reporting (PRISMA-ScR) guidelines. 18
Search strategy
The following databases were searched by a health sciences librarian (L.S.) during the electronic component of the scoping review: Medline and Medline in Process through Ovid (1946 to February 19, 2021), Embase Classic + Embase through Ovid (1947 to February 19, 2021), the Cochrane Library—CENTRAL through Ovid, APA PsycINFO through Ovid (1806 to February Week 3, 2021), CINAHL through EBSCOHost (1947 to February 21, 2021), and AARP AgeLine through EBSCOHost (searched February 21, 2021).
A search strategy for palliative care, Parkinson's disease (PD; or parkinsonism), and motor symptoms (or dysphagia) as outlined in Supplementary Figure S1 was developed in Medline, and then translated into the other databases, as appropriate. All databases were searched from dates of inception to February 21, 2021. There were no publication restrictions. All references were entered into an Endnote file for processing (n = 5872). Detailed search strategy and full list of search terms are presented in Supplementary Figure S1.
Study selection
Inclusion criteria consisted of adult (>18 years of age) patients with end-stage PD (or parkinsonism) who had motor symptoms and dysphagia, who were followed by or eligible for palliative care. Primary research, review articles, and gray literature were considered for inclusion. Both qualitative and quantitative studies were included. Studies that included patients with diagnoses other than PD (or parkinsonism) and those that included patients with early PD and high functional status were excluded.
Importantly, studies that examined patients who were also on oral levodopa or other oral Parkinson's medications were excluded. Studies that used DBS, LCIG, transcranial magnetic stimulation, and focused ultrasound were excluded as it was felt that these were intensive and invasive procedures not appropriate for palliative or EoL care. Finally, studies not published in English, articles in which full text was not available, commentaries, editorial, correspondences, conference or poster abstracts, and clinical trial protocols were also excluded. Full list of inclusion and exclusion criteria are shown in Table 1.
Inclusion and Exclusion Criteria
DBS, deep brain stimulation; EoL, end of life.
Titles, abstracts, and full texts of studies identified through the literature search were uploaded into Covidence software. 19 Four reviewers (W.J.K., P.E., C.L.W., and J.Z.) independently performed title and abstract screening as well as full-text screening to determine study eligibility, with each reference reviewed by two reviewers. Conflicts in screening were discussed and resolved between two reviewers (W.J.K. and J.Z. or C.L.W.) without the need for third-party arbitration. Studies that did not meet the a priori inclusion and exclusion criteria above were excluded.
Data extraction
One reviewer (W.J.K.) independently completed data extraction, and this was validated by two reviewers (C.L.W. and P.E.). General study information as well as population demographics was first recorded in an Excel spreadsheet, and summarized in Tables 2 and 3. 20
Characteristics of Included Studies
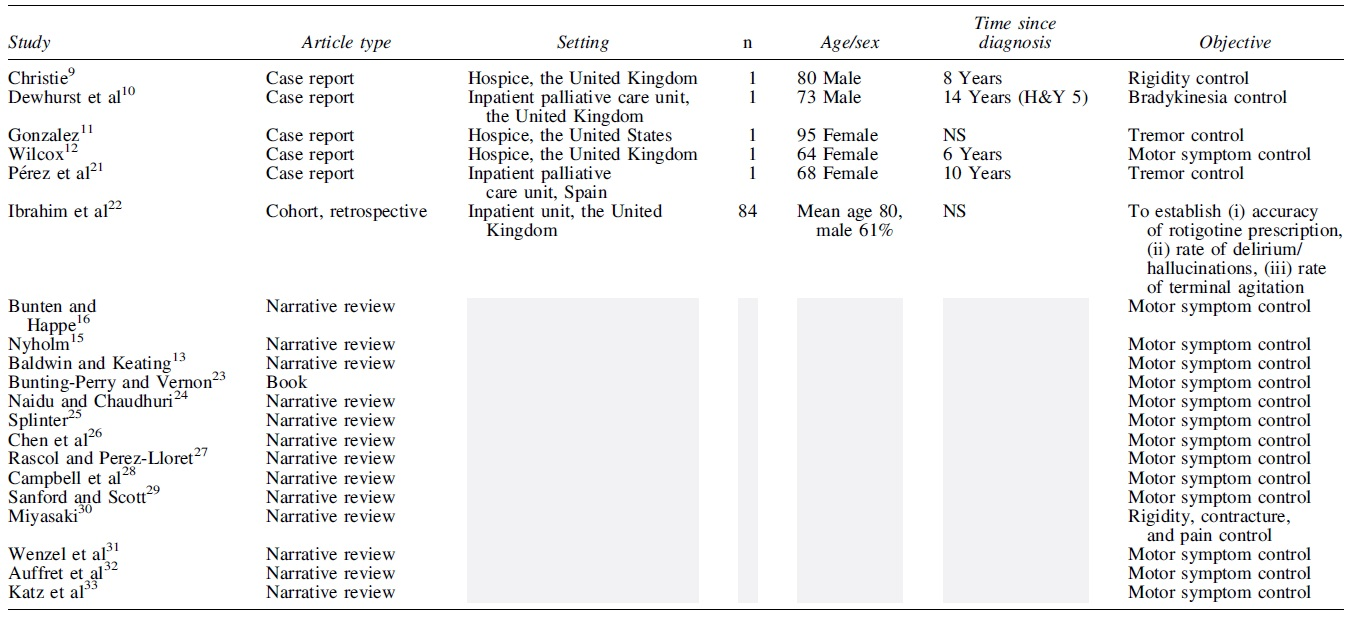
H&Y, Hoehn and Yahr stage; n, number of participants; NS, not specified.
Interventions and Outcomes of Included Studies
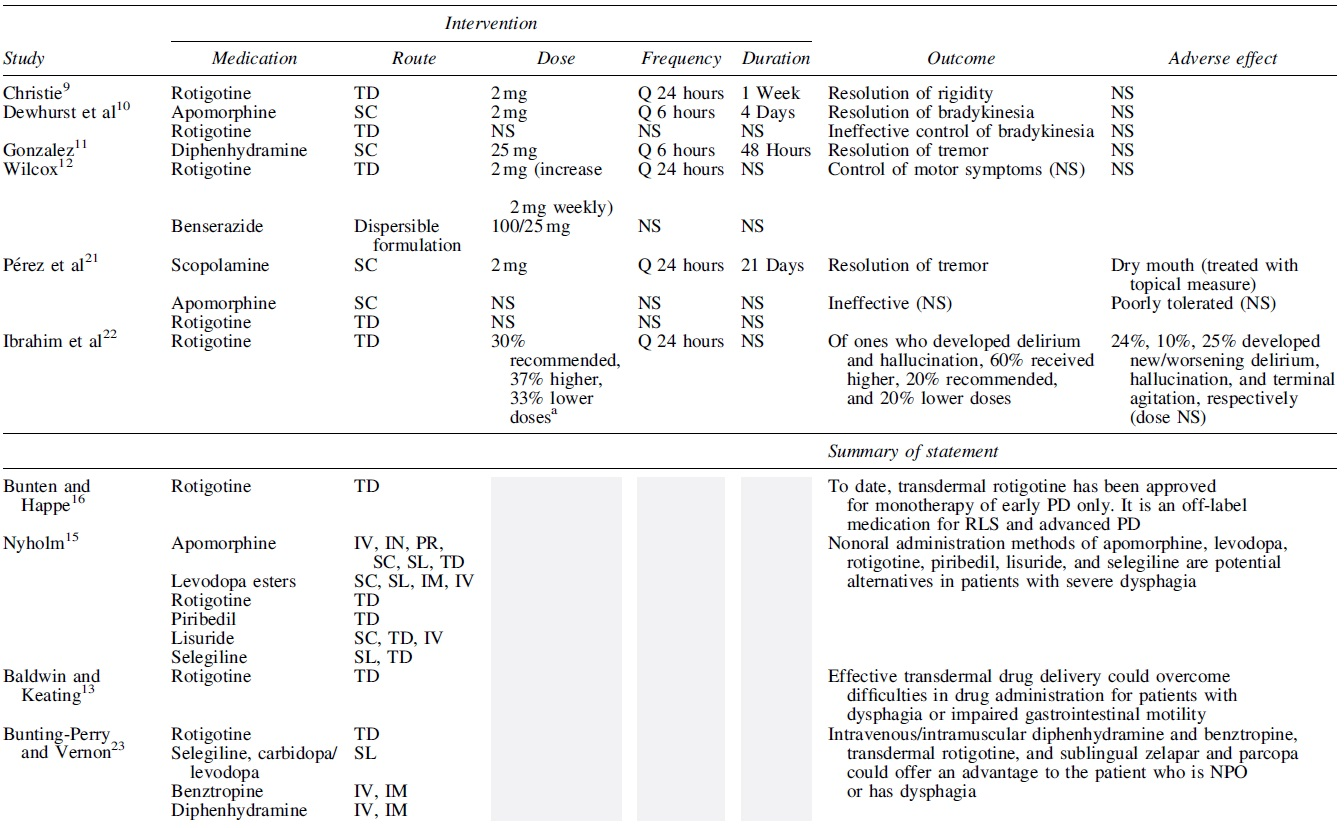

Data pertaining to time since PD diagnosis, medical context, treatment objective, pharmacological intervention, route, dose, frequency and duration, outcome measures were extracted and tabulated. No formal quality assessment was performed for this scoping review; however, any major methodological/quality concerns were recorded during the process of data extraction. All conflicts in data extraction were discussed between reviewers and resolved without the need for available third-party arbitration.
Results
Study inclusion
The initial literature search identified 5872 articles. After the removal of duplicates (2051 articles), 3821 articles underwent primary title and abstract screening, and 259 articles progressed to full-text screening. Two hundred thirty-nine articles were excluded after full-text screening: 20 were based on wrong patient population notably not in palliative or EoL care setting, 63 demonstrated patients who were also on oral levodopa treatment, 52 were conference or poster presentation abstracts, 11 were clinical trial protocols, 15 showed wrong outcome that is unrelated to assessing symptoms of PD, 4 used oral route of administration, 3 used wrong intervention such as device-aided therapy, 3 discussed nonmotor symptoms, 8 were not in English, one was commentary, and full text was unavailable for two articles despite additional searches through different library resources independent of the primary search.
An online search of the gray literature was conducted. The gray literature search did not result in the inclusion of any additional articles. Ultimately, a total of 20 articles were included in the scoping review. The process of record identification and screening is summarized in Figure 1.
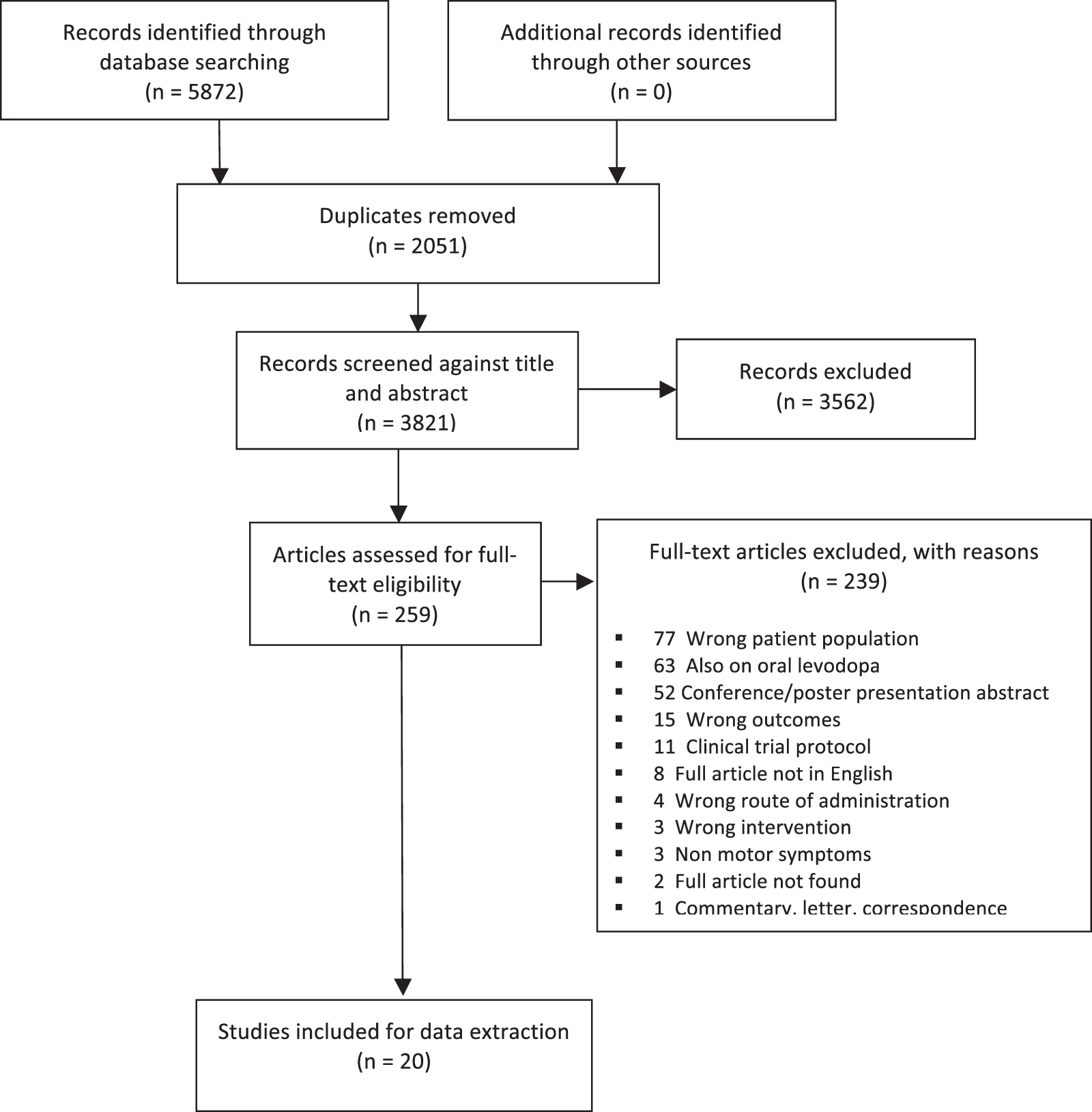
Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram.
Study demographics
This scoping review included a total of 20 studies: 5 were case reports, 1 was retrospective cohort study, 1 was a book chapter, and 13 were narrative reviews as shown in Table 2.9–13,15,16,21–33 Of the primary research studies, three different countries were represented. Five case reports demonstrated clinical cases of five patients with end-stage PD, receiving EoL care (n = 1 per study), and a retrospective cohort study involved a total of 84 patients with advanced PD.9–12,21,22 Reported clinical cases were from settings of a hospice (n = 3) and an inpatient medical unit (n = 2).9–12,21 The cohort study was in the setting of an inpatient unit. 22 A book chapter and 13 narrative reviews did not illustrate particular patient cases, but discussed few previously published primary research studies or displayed available general medication information.13,15,16,23–33
Case reports
As shown in Tables 2 and 3, five distinct clinical cases showed an effective use of rotigotine transdermal patch (one case), subcutaneous apomorphine (one case), diphenhydramine (one case), benserazide (one case), and scopolamine (one case) in patients with advanced PD with dysphagia, receiving EoL care.9–12,21 Ineffective use of transdermal rotigotine (two cases) and subcutaneous apomorphine (one case) was also reported.10,21
Christie reported a case of an 80-year-old male with advanced PD and complete dysphagia due to an advanced gastro-esophageal cancer. Her rigidity resolved with rotigotine transdermal patch monotherapy, and the patient had no adverse effects. 9 Similar effect was seen in the case of a 64-year-old female with PD and history of breast cancer and gastric secondary malignancies limiting the ability to take oral medications. Rotigotine patch and benserazide dispersible formulation effectively managed distressing motor symptoms (not specified) without adverse side effects. 12
Rotigotine transdermal patch was ineffective in two cases. In the case of a 73-year-old male with advanced PD, severe urosepsis, and distressing bradykinesia, rotigotine patch was ineffective in resolving eyelid closure and dysphagia despite upward titration. Subcutaneous apomorphine administration as monotherapy resulted in improvement of these symptoms. 10
Pérez et al. reported a case of a 68-year-old female with advanced PD, metastatic gastric cancer with bowel obstruction, and severe tremor. 21 Rotigotine patch was also ineffective in managing distressing tremor, and subcutaneous apomorphine caused severe nausea and vomiting, which is a known adverse effect of apomorphine. 14 Adequate relief of tremors was achieved with subcutaneous scopolamine. Its side effect of dry mouth was effectively treated with topical measures. 21
Subcutaneous diphenhydramine, another anticholinergic agent, promptly resolved severe tremors of all extremities within few hours in a 95-year-old female with advanced PD, receiving EoL care. 11 No adverse effect was reported. 11
Cohort study
The retrospective cohort study by Ibrahim et al. describes the dosing and effectiveness of rotigotine transdermal patch when used to replace oral dopaminergic agents in patients with advanced PD and dysphagia. 22 The OPTIMAL drug conversion calculator (calculator 2) was used to determine a correct conversion of oral PD medications to rotigotine patch.34,35 Of the 84 patients (76 with idiopathic PD and 8 with atypical parkinsonism), 30% received the recommended dose while 37% received a higher dose and 33% received a lower than recommended dose. 22 Of all the subjects, 24% developed new or worsening delirium. Of these, 60% received a higher than recommended dose, 20% received the recommended dose, and 20% received a lower than recommended dose of the rotigotine patch.
Of all of the subjects, 10% developed new or worsening hallucination (dose not specified). Of the 40 patients who died in hospital, 25% had terminal agitation (dose not specified). 22 The authors concluded that acute conversion of oral dopaminergic agents to transdermal rotigotine remains problematic despite the availability of validated tools, and that inappropriate dosing may precipitate or worsen delirium or hallucinations. 22 The effectiveness for motor control was not discussed.
Narrative reviews and book chapter
As shown in Tables 2 and 3, 13 narrative reviews and one book chapter described use of pharmacological agents and formulations for patients with advanced PD and dysphagia.13,15,16,23–33
Ten reviews discussed use of rotigotine transdermal patch.13,15,16,23–29 Bunten and Happe stated that rotigotine patch is approved for monotherapy of early PD only, but an off-label use is practiced for advanced PD. 16 Campbell et al. also suggested unlicensed indication of rotigotine patch for patients with advanced PD and dysphagia. 28 Naidu and Chaudhuri suggested a use of rotigotine patch for a small number of PD patients who may be acutely ill or unable to take oral treatment (also in the pre/postsurgical period). 24
Splinter discussed the use of rotigotine as an alternative route for patients with dysphagia. Importantly, these discussions were informed by reviewing primary studies where rotigotine was used in addition to oral levodopa.17,25 Chen et al 26 and Rascol and Perez-Lloret 27 expanded a discussion of the once-daily transdermal rotigotine patch in conveying valuable benefits for patients with dysphagia and referenced to Christie. 9 Other reviews including Baldwin and Keating, 13 Bunting-Perry and Vernon, 23 Nyholm, 15 and Sanford and Scott 29 also discussed transdermal rotigotine as an alternative method for patients with dysphagia, which is “very common in PD.” The efficacy, dose, and adverse effects were not discussed.
Three reviews described the use of apomorphine, a nonselective dopamine agonist.15,31,32 Nyholm presented a list of commercially available formulations of apomorphine in intravenous, subcutaneous, intranasal, rectal, sublingual, and transdermal forms. 15 Wenzel et al. discussed apomorphine injection as a useful option for monotherapy when the delay in effect of levodopa is due to gastrointestinal dysfunction. However, this is based on an ongoing clinical trial using apomorphine as adjunctive to oral levodopa. 31
Finally, Auffret et al 32 in their narrative review described a case of a 73-year-old male with advanced PD who was unable to tolerate oral medications. It highlighted a pragmatic use of apomorphine subcutaneous injection, which resulted in alleviation of discomforting motor symptoms.10,32 The authors also acknowledged that more studies are needed to confirm the benefit of apomorphine injections, but stated that it deserves to be considered in terminal PD and palliative care. 32
Bunting-Perry and Vernon mentioned sublingual selegiline and carbidopa/levodopa, and intravenous/intramuscular formulations of benztropine and diphenhydramine, offering an advantage to the patients who is nil per os or has dysphagia. 23 Katz et al. also proposed carbidopa/levodopa disintegrating tablets and rectal carbidopa/levodopa as possible alternatives for PD patients with pill dysphagia.33,35 Miyasaki discussed Botulinum toxin injection for PD patients in palliative care with severe rigidity to avoid contractures and pain.30,36
Discussion
This scoping review was performed to provide an exhaustive summary of current literature on interventions for patients with PD without safe oral access in managing distressing motor symptoms.
Through exhaustive search strategy and stepwise search analysis according to PRISMA-ScR guidelines, 18 20 articles were selected for data extraction from initially identified 5872 articles. These included 5 case reports, 1 retrospective cohort study, 1 book chapter, and 13 narrative reviews. The current literature does not provide clear evidence for the use of alternative pharmacological agents and formulations for patients with advanced PD and dysphagia in the palliative care setting.
Rotigotine transdermal patch has been widely recommended throughout a number of narratives and anecdotal clinical cases. Although rotigotine patch has been approved as monotherapy in treating motor features in early PD,14,17 its effect as monotherapy in advanced PD or at EoL in patients not tolerating oral carbidopa/levodopa concurrently has not been studied. 16
Off-label use of rotigotine patch in advanced PD is a consensus opinion, although there are currently no established guidelines on treating motor symptoms in patients with end-stage PD and severe dysphagia.37–41 Incorrect conversion of oral carbidopa/levodopa or other oral dopaminergic agents to rotigotine patch may result in distressing delirium, hallucination, and terminal agitations. 22 If used, it is important for the standardized method to be used when converting oral PD medications to rotigotine and for delirium risk to be taken into account.
Another promising alternative is subcutaneous apomorphine. Intermittent injection of apomorphine is an effective rescue therapy to oral carbidopa/levodopa. 42 The efficacy of continuous subcutaneous apomorphine infusion as monotherapy has been established in non-palliative care patients recently.43,44 The most commonly reported adverse effects, occurring in up to 70% of patients treated with subcutaneous apomorphine, were local skin nodules at the injection site. 43 Less commonly, sedation, nausea/vomiting, visual hallucination, and orthostatic hypotension were reported.15,43 These adverse effects were not reported in the studies that were identified in our scoping review.10,21 There are no direct comparison studies of subcutaneous apomorphine to transdermal rotigotine or other alternatives.
This is the only study to extensively review the topic of noninvasive pharmacological interventions for patients with advanced PD and dysphagia. We screened ∼4000 articles and carefully followed the ethology outlined by PRISMA-ScR. This study has some limitations. First, given the nature of the included studies, a formal quality assessment was not completed. However, it should be noted that all included case reports relied on a single participant for each medication.
This limits our ability to draw any meaningful conclusions with respect to potentially effective medications. Although this scoping review focused on identifying studies on existing noninvasive pharmacological interventions for patients with advanced PD with motor symptoms without safe oral access, a number of the identified narrative reports based their recommendations on primary studies in other clinical contexts such as patients concurrently taking oral carbidopa/levodopa. In addition, the focus of our study in the specific population with dysphagia in palliative care setting likely excluded studies looking at patients in other contexts such as peri/postoperative setting and illness resulting in dysphagia.
The latter could provide valuable information on alternatives to oral route in patients with dysphagia and distressing motor symptoms of PD. We also excluded invasive therapies such as PEG tube, LGIC, and DBS as they would not be suitable or consistent with treatment goals for a patient receiving palliative care, but could be beneficial for patients with advanced PD and dysphagia. There is a clear need for more research looking at noninvasive pharmacological interventions for patients with advanced PD and dysphagia.
It would be important to quantify the efficacy of medications in controlling motor symptoms and to describe side effects. In this population, the high frequency of cognitive impairment may make subjective assessments of motor symptoms and quality of life difficult. However, quantitative measurement of rigidity and tremor using sensors could be implemented. In addition, since quality of life is a key goal of providing palliative care, estimates of quality of life could be rated by proxy care partners as an additional indicator.45,46
Conclusion
In conclusion, this scoping review illustrates that there is currently no clear evidence for alternative pharmacological agents and formulations for patients with advanced PD and dysphagia, receiving EoL care. The rotigotine patch is the most frequently recommended medication based on studies in nonpalliative PD patient populations. Future prospective cohort studies are warranted to assess the effectiveness and side effects of available medications for patients with advanced PD in the palliative care setting who are unable to take oral medications.
Footnotes
Authors' Contributions
The corresponding author is responsible for ensuring that the descriptions are accurate and agreed by all authors. W.J.K. collected, synthesized the data, and drafted the article for intellectual content. C.L.W., P.E., and J.Z. revised the article for intellectual content. For the study selection, four reviewers (W.J.K., C.L.W., P.E., and J.Z.) independently performed title and abstract screening as well as full-text screening to determine study eligibility, with each reference reviewed by two reviewers. Conflicts in screening were discussed and resolved between two reviewers (W.J.K. and J.Z. or C.L.W.) without the need for third-party arbitration.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or nonprofit sectors. This research did not require ethics approval.
Author Disclosure Statement
The authors have no conflict of interest to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.