
Abstract
Background:
Patients with life-limiting cancers are commonly prescribed opioids to manage pain, dyspnea, and cough. Proper prescription opioid disposal is essential to prevent poisonings and deaths.
Objective:
We examined opioid disposal practices of patients referred to a Canadian outpatient palliative care clinic (OPCC). The primary objective was to determine the prevalence of OPCC patients who did not routinely dispose their opioids. The secondary objectives were to examine their methods of opioid disposal and to identify patient characteristics associated with routine disposal of opioids.
Design and Setting:
This cross-sectional study involved a retrospective chart review of new, adult patients who were seen in a Canadian OPCC (September 2018–August 2019) and completed a survey about opioid-related constructs: source of prescriptions, use, storage, disposal, and knowledge about associated harms.
Results:
Among the 122 study participants, half (58/111, 52.3%) reported that they did not routinely dispose their opioids. The most common method of disposal was by giving them to pharmacists (69/88, 78.4%). Cannabis use (odds ratio [OR]: 3.7, 95% confidence interval [CI]: 1.1–11.8) and neuropathic medication use (OR: 3.0, 95% CI: 1.2–7.2) were positively associated with routine disposal of opioids. Conversely, reports of an increased amount of opioid use in the past six months were negatively associated with routine disposal of opioids (OR: 0.38, 95% CI: 0.16–0.88).
Conclusion:
The high prevalence of people with life-limiting illnesses who do not routinely dispose their opioids requires increased attention. Interventions, such as education, are needed to reduce medication waste and opioid-related harms.
Introduction
Between 2016
Analgesics, such as opioids, are among the most common wasted medications.9,10 Medication waste refers to any expired or unused medications generated by prescribers, dispensers, and patients. 11 When medications are discarded, economic losses are incurred from operational waste and contribute to the high costs associated with health care.11,12 Discarded medications in sewage water and leachate can also alter environments, contaminate drinking water, and cause animal deaths.13–15
Symptom management in the context of life-limiting illnesses is a common indication for opioid prescribing. 16 The proportion of patients receiving palliative care who are provided opioids generally increases as death approaches, with reported frequency at the end of life varying from 25% to 99%.17,18 Despite the large quantities of opioids dispensed, limited information exists about unused opioids and their disposal by patients receiving palliative care. To our knowledge, there are only four published studies, conducted in the United States and Japan, about unused opioids and their disposal in the context of palliative care.19–22
Given the paucity of information, we aimed to conduct the first study that would examine the opioid disposal practices of patients with life-limiting cancers in a Canadian outpatient palliative care clinic (OPCC). Our primary objective was to determine the prevalence of outpatients with life-limiting cancers who did not routinely dispose their opioids. Our secondary objectives were to examine their opioid disposal methods and to identify characteristics associated with routine disposal of opioids. Based on previous studies, we hypothesized that the prevalence of patients who do not routinely dispose their opioids would be between 49% and 60%.19–22 We also hypothesized that only a minority of patients would properly dispose their opioids by returning them to their pharmacy.
Methods
Setting
Princess Margaret Cancer Centre (PM) is Canada's largest cancer center that provides care for people in the city of Toronto and elsewhere in the province of Ontario. The PM palliative care program includes an OPCC that provides palliative care to ∼1300 new patients annually. 23 Oncologists refer patients with advanced cancer and estimated prognoses of less than two years to this interdisciplinary clinic to improve their quality of life through assessment and management of physical and psychosocial concerns.24,25
The overall process for the OPCC initial consultation is shown in Figure 1. When patients attend their appointment, they are asked to complete an intake form about their medication history and priorities for the visit, and the Edmonton Symptom Assessment Scale (ESAS) to screen for the presence and intensity of common symptoms experienced by patients with advanced cancer.23,24 Following the completion of these forms, a nurse reviews them and obtains a medical and social history.23,24 If the patients report that they are taking prescription opioids, then they are given the Opioid Safety Survey to complete before they are assessed by their palliative care physician.
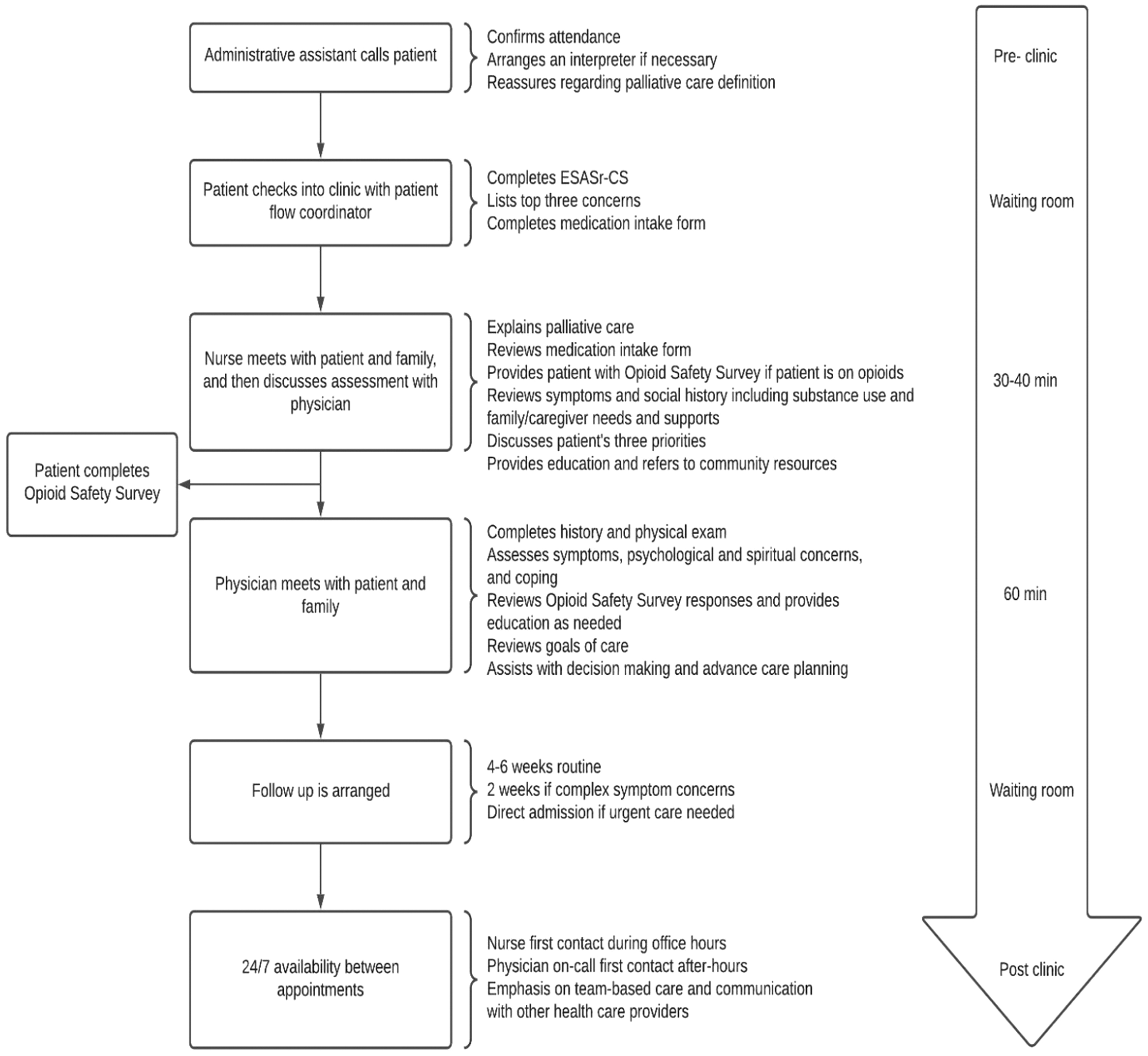
Overview of initial outpatient palliative care consultation. Reproduced and adapted with permission under CC BY-NC (Zimmermann & Lau, 2019). ESASr-CS, Edmonton Symptom Assessment System revised-Constipation, Sleep.
In response to the opioid crisis, the OPCC implemented the routine use of the Opioid Safety Survey in September 2018 to assess new patients' practices and knowledge related to opioids. Supplementary Appendix SA presents the Opioid Safety Survey. The survey is composed of 25 questions, where the first 3 are screening questions for opioid use disorder based on the Patient Drug Use Questionnaire (PDUQ). These questions from the PDUQ were found to have the highest predictive value for the presence of addiction in patients with chronic pain receiving long-term opioid therapy.26,27 The remaining 22 questions assess the following opioid-related constructs: source of prescriptions, use, storage, disposal, and knowledge about associated harms.
These questions were originally developed for adult patients with cancer assessed in a U.S. tertiary cancer center's supportive care clinic and emergency department.20,21 Its use recently expanded to parents of pediatric patients with cancer in the cancer center's child and adolescent center. 28 In the PM OPCC, after patients complete the survey, their responses are reviewed by their palliative care physicians. If concerns about opioid storage, use, and/or disposal are identified, the physicians provide the patients with verbal and written education that is consistent with Government of Canada recommendations. 29
Study participants
The study participants were patients who received initial consultations in the OPCC. All patients referred to the OPCC are 18 years or older and have advanced cancer diagnoses with estimated prognoses of ≤2 years. Patients were included in this study if they were taking opioids and completed the Opioid Safety Survey.
Study design
This cross-sectional study involved a retrospective chart review of patients who received initial OPCC consultations and completed the Opioid Safety Survey between September 1, 2018, and August 31, 2019. A consecutive chart review was completed of all patients on prescription opioids who received initial consultations in the OPCC and completed the Opioid Safety Survey. The following data were extracted from the patients' medical records: demographics, medical conditions, medications, substance use, ESAS scores, and Opioid Safety Survey responses.
Ethics
University Health Network Research Ethics Board (REB) approval was obtained on December 14, 2018. A consent waiver request was completed and approved by REB because obtaining consent was not possible given the limited prognoses of the study participants.
Missing data
The Opioid Safety Survey was distributed only once to patients at their initial OPCC consultations. A record of the number of missing responses for each of the questions was maintained. We excluded the patients (n = 7) who responded to less than three questions as they likely only answered the first three questions screening for opioid use disorder. A sensitivity analysis was conducted to compare the patients who were included and excluded from the study. These two groups were comparable except that included patients had higher mean ESAS pain scores (5.8 [standard deviation, SD 2.6] vs. 3.9 [3.4], p = 0.045) and were more likely to be on nonopioid analgesics (55/122 [45.1%] vs. 0/7 [0%], p = 0.02).
Statistical analysis
We used IBM SPSS Statistics Version 27.0 to conduct statistical analysis. Descriptive statistics were calculated to determine the proportion of people who did not routinely dispose their opioids and to describe their demographics, medical histories, survey responses, and ESAS scores. These statistics include mean, median, SD, and confidence intervals (CIs). The exact binomial method was used to calculate 95% CIs. We conducted exploratory univariate analyses to identify potential predictive variables for routine disposal of opioids. Specifically, we compared the characteristics of people who did and did not routinely dispose their opioids using two-sample unpaired t tests for continuous variables, Mann–Whitney–Wilcoxon test for rank-based data, and chi-squared test or Fisher's exact test for categorical variables.
We then conducted a multivariable logistic regression analysis to examine the associations of demographics, clinical characteristics, and survey responses with nonopioid disposal. Variables for which the abovementioned univariate analyses demonstrated an association significance level of p < 0.20 were included in the variable selection process. Model fit was analyzed with an overall regression F-statistic throughout the process of backward stepwise selection. Variables with a significance level of p < 0.10 in the final multivariable model were retained.
Post hoc analysis
Distribution of the Opioid Safety Survey was integrated into the initial OPCC consultation process. If the OPCC nurses identified in the intake that patients were on prescription opioids, then they would provide the patients with the Opioid Safety Survey to complete before their assessment by a palliative care physician. During our study time period, there were likely patients on prescription opioid who could have completed the Opioid Safety Survey but were not provided it by the nurses. Therefore, we completed a post hoc analysis to estimate the proportion of patients who could have been included in the study and to compare their characteristics with the study participants to identify any significant differences; and to estimate the proportion of patients who would have been excluded from the study due to inability to communicate in English, severe cognitive impairment, and/or severe physical symptoms.
Using simple randomization, we generated a random sample of 120 patients who received initial OPCC consultations within the study time period. From the electronic patient records and palliative care charts, we conducted a chart review to collect the same data as the study participants. We conducted data analysis using descriptive statistics to determine the proportion of patients in the random sample who could have completed the Opioid Safety Survey. We also determined the proportion of patients who were unable to communicate in English, proportion of patients with severe cognitive impairment (as documented in the patients' charts), and proportion of patients with severe physical symptoms (ESAS scores 7 to 10). Furthermore, we compared the demographics and medical characteristics of the random sample patients who could have completed the Opioid Safety Survey with those of the actual study participants to identify any significant differences between the two samples that would suggest sampling and selection biases.
We used two-sample unpaired t tests for continuous variables, Mann–Whitney–Wilcoxon test for rank-based data, and chi-squared test or Fisher's exact test for categorical variables.
Results
During the study period, a total of 1133 patients received an initial palliative care consultation in the OPCC. Figure 2 provides a summary of the study participant inclusion process. The Opioid Safety Survey was administered to 303 patients by the OPCC nurses. Of these patients, 129 patients reported being on prescription opioids at the time of their consultations (129/303; 42.6%). After excluding 7 patients who responded to less than three survey questions, our study included a total of 122 participants.

Summary of study participant inclusion process.
Table 1 summarizes the study participant characteristics. Their average age was 64.5 (SD 12.6) years, ranging from 29 to 90 years of age; and 46.7% (57/122) were female. Approximately a third of participants (45/122; 36.9%) reported that they immigrated to Canada. The most common primary cancer diagnosis was gastrointestinal (28/122; 23.0%), and histories of chronic pain and concurrent mental illness were reported by 20.5% (25/122) and 19.3% (16/83) of participants, respectively. Regarding substance use, 16.5% (20/121) reported current use of cannabis, where 35.0% (7/20) used cannabidiol (CBD) only, 15.0% (3/20) a CBD/tetrahydrocannabinol (THC) combination, and 10.0% (2/20) THC-only products in the form of oils, capsules, e-cigarettes, and gummies.
Study Participant Characteristics
Eighty-three participants had documented psychiatric history.
One hundred participants had documented smoking history.
Ninety-five participants had documented alcohol history.
One hundred twenty-one participants had documented cannabis history.
Data available for 121 participants.
SD, standard deviation.
Opioid disposal
Almost all the study participants (111/122, 91.0%) responded to the survey question about whether or not they routinely dispose their opioids. The participants who did and did not respond to this survey question did not differ significantly in terms of their demographics and medical characteristics. Although the majority of participants (92/114; 80.7%) reported that they were aware of proper disposal methods for opioids, half of the participants (58/111; 52.3%) reported that they did not routinely dispose their opioids. The most common method of opioid disposal was returning them to their pharmacist (69/88, 78.4%). Compared with participants who did routinely dispose their opioids, participants who did not routinely dispose their opioids were less likely to be using neuropathic adjuvant medications (13/58 [22.4%] vs. 23/53 [43.4%], p = 0.025) and cannabis (5/58 [8.8%] vs. 13/53 [4.5%], p = 0.038).
In terms of characteristics, they did not differ according to age, sex, residence, primary language, primary cancer types, histories of chronic pain and psychiatric conditions, and smoking and alcohol use (Table 2). In addition, their symptom burden was comparable according to ESAS individual symptom, and physical, psychological, and total symptom distress scores (Table 3).
Comparison of Characteristics Between Participants Who Do and Do Not Routinely Dispose Opioids (Total N = 111) a
Eleven participants did not respond to the Opioid Safety Survey question #9 about routine disposal of opioids.
Comparison of Edmonton Symptom Assessment System Revised—Constipation Sleep Mean Scores Between Patients Who Do and Do Not Routinely Dispose Their Opioids
TSDS is defined as the sum of the individual scores from each of the ESAS symptoms except for constipation and sleep. TSDS calculated for 108 respondents who completed all ESAS questions. TSDS ranged from 3.00 to 87.00.
PHS is defined as the sum of the scores from pain, nausea, tiredness, drowsiness, nausea, shortness of breath, and lack of appetite. PHS was calculated for 108 respondents who completed all ESAS questions. PHS ranged from 2.00 to 57.00.
PSS is defined as the sum of the scores from depression and anxiety. PSS was calculated for 108 respondents who completed all ESAS questions. PSS ranged from 0 to 20.00.
ESAS, Edmonton Symptom Assessment Scale; PHS, physical subscore; PSS, psychological subscore; TSDS, total symptom distress score.
Regarding Opioid Safety Survey responses, participants who did not routinely dispose their opioids were more likely to respond that they did not dispose just in case they needed them in the future (39/57 [68.4%] vs. 17/51 [33.3%], p < 0.001). Participants who did and did not routinely dispose their opioids did not differ in terms of other variables including their opioid prescriber, storage, and unsafe opioid use (defined as sharing or losing their opioids). 19 Table 4 presents the survey responses of all study participants and comparisons of the survey responses between people who did and did not routinely dispose their opioids.
Opioid Safety Survey—Responses of All Participants and Comparison of Responses Between Participants Who Did and Did Not Routinely Dispose Their Opioids
The denominator is the number of respondents who answered both the listed survey question and survey question #9 about routine disposal of opioids.
In a multivariable regression model, cannabis use (odds ratio [OR]: 3.7, 95% CI: 1.1–11.8) and neuropathic medication use (OR: 3.0, 95% CI: 1.2–7.2) were positively associated with routine disposal of opioids. Conversely, participants who responded “Yes” to the PDUQ question, “Have you had to increase the amount of opioids you take over the past 6 months?” were less likely to routinely dispose their opioids (OR: 0.38, 95% CI: 0.16–0.88). Table 5 summarizes the multivariable logistic regression model of factors associated with routine disposal of opioids.
Multivariable Logistic Regression Model of Factors Associated With Routine Disposal of Opioids
CI, confidence interval; OR, odds ratio.
Impact of physician and pharmacist education
More than half of the study participants (68/116; 58.6%) reported that they received education from their pharmacists or physicians about disposal of their opioids. Participants who reportedly received education from physicians or pharmacists about opioid disposal were more likely to be aware of proper disposal of their opioids (68/68 [100%] vs. 26/48 [54.2%], p < 0.001). They were more likely to dispose their opioids by giving them to pharmacists (49/68 [72.0%] vs. 18/48 [37.5%], p < 0.001); and less likely to dispose their opioids by flushing them down the toilet (0/68 [0%] vs. 2/48 [4.2%], p < 0.001) and throwing them away in the trash (0/68 [0%] vs. 9/48 [19.8%], p < 0.001).
Furthermore, participants who received physician or pharmacist education about opioid disposal were more likely to conduct pill counts to see how many were left (39/68 [57.4%] vs. 14/48 [29.2%], p = 0.002) and to have knowledge about drug take-back programs (29/68 [44.6%] vs. 8/48 [16.7%], p = 0.002).
Post hoc analysis
From the random sample of 120 patients who received initial OPCC consultations between September 1, 2018, and August 30, 2019, we identified that 39/120 (33%) patients could have completed the Opioid Safety Survey if they were provided it. When we compared the demographics, medical and medication histories, and symptom scores of these patients with the study participants, we found that the two groups were comparable except for their chronic pain histories and use of neuropathic adjuvants. Table 6 summarizes the comparisons of the characteristics between the study participants and random sample of eligible patients. The study participants were less likely to have histories of chronic pain ([25/122 (20.5%) compared with 11/39 (28.2%)]; p = 0.006) and more likely to be prescribed neuropathic adjuvants (37/122 [30.3%] compared with 3/39 [7.7%]; p = 0.005).
Comparison of Characteristics Between Study Participants and Random Sample of Eligible Patients
Data about smoking history were available for 110 study participants and 30 eligible study sample patients.
Data about alcohol history were available for 105 study participants and 31 eligible study sample patients.
Data about cannabis history were available for 121 study participants and 39 eligible study sample patients.
For the remaining 81/120 (67.5%) patients, they would have been excluded from the study due to the following reasons: 57.6% (68/118) were not on opioids at the time of their OPCC consultation; 17.5% (12/120) could not read or write in English; 6.2% (7/113) had severe cognitive impairment; and 81.6% (93/114) had severe physical symptoms. Seven (5.8%) of the participants had more than one exclusion reason.
Discussion
In this study, 52.3% of patients with life-limiting cancers referred to the PM OPCC between September 2018 and August 2019 did not routinely dispose their opioids. This finding is consistent with other studies about patients with cancer who receive palliative care. In a U.S. tertiary cancer center, 53% of its supportive care outpatients and 53% of patients surveyed in its emergency department were found to not routinely dispose their opioids.19,21 Likewise, in a Japanese palliative care unit for adult patients with advanced cancers, 62% of patients reported that they did not dispose their unused medications when they were surveyed at the time of readmission to the unit. 22 This high prevalence of nondisposal of opioids is concerning given that prescription opioids account for 18% to 24% of opioid-related deaths in Canada and the United States.1,2
The most common method of disposal, reported by 78.4% of study participants, was giving their unused opioids to pharmacists. In contrast, previous studies reported that patients most commonly disposed their opioids by flushing them down the toilet (18–24%) or throwing them in the trash (11–17%).19,21,22 Almost all participants in this study (81%) reported that they were aware of proper disposal methods for opioids, whereas in other studies, only 22% to 26% of participants reported having this knowledge. These findings may reflect the impact of the response efforts to the U.S. and Canada opioid crises that include public education campaigns about proper opioid disposal to reduce opioid-related health harms.30–33
In our study, more than half of the participants reported receiving education about disposal of opioids from their pharmacists or physicians. In other studies, only 11% of patients with cancer surveyed in an emergency department and 40% of patients with acute and chronic noncancer pain stated that they received education about opioid disposal.21,34 Education about disposal may influence patients' behaviors around opioid safety. In our study, we found a positive association between receiving pharmacist or physician education about disposal of opioids and patients reporting that they have knowledge about proper disposal methods, drug take-back programs, and conducting pill counts.
These findings are consistent with a study conducted in a U.S. supportive care clinic, where patients reported being more aware of proper disposal of medications after the clinic started delivering personalized education and a handout on safe opioid use, storage, and disposal to patients when they received an opioid prescription. 20 Future intervention studies should be conducted to evaluate the impact of education on patients' behaviors around use and disposal of opioids.
Education can be incorporated into patients' interactions with health care professionals. Our study found that participants who reported use of neuropathic adjuvants and cannabis were over three times more likely to routinely dispose their opioids. To our knowledge, this study is the first to identify these associations. A potential explanation for this finding is that people who are prescribed adjuvant analgesics and cannabis may have a longer history of opioid use, and therefore may have more interactions with health care professionals over time. The correlation between intensity of education provided over time and opioid disposal practices should be explored in subsequent studies.
Another area that should be explored in future research is the relationship between opioid use disorder and disposal of opioids. Our study found that patients who routinely disposed their opioids were less likely to respond “Yes” to the opioid use disorder screening question, “Have you had to increase the amount of opioids you take over the past six months?” This finding may suggest that people who routinely dispose their opioids are less likely to have problematic opioid use. However, this finding should be interpreted with caution as this screening question has not been validated for use in palliative care; as patients with life-limiting illnesses approach the end of their lives, they often require increasing opioid doses to relieve worsening symptoms. 17 Studies are needed to develop and validate tools to identify opioid-related health harms in palliative care. 35
An important study finding was that 50.9% of the participants shared that they did not dispose their opioids in case they need them in the future. This reason for keeping opioids has been reported in numerous other studies including those about patients with cancer and U.S. adults with history of recent prescription opioid use.19,21,36 Studies suggest that the main motivation for keeping unused medications is to have immediate access to effective pain therapy for future management of the same or a different condition for which the opioids were originally prescribed. 34
Other reasons for keeping the opioids include having them available for family and friends in case they need them; lack of knowledge about how to dispose opioids; concerns about the environmental impact of opioid disposal; and the inconvenience of disposing the unused opioids.34,37 Given the universality of this reason for nondisposal of opioids, it is imperative that there is increased understanding of why people feel the need to keep medications for future use, especially in countries with universal access to health care.
Limitations
This study has limitations. The Opioid Safety Survey was routinely distributed by nurses to all new PM OPCC patients on prescription opioids; therefore, social desirability bias and recall bias may have occurred. Data collection was limited by the availability and quality of information documented in the patients' charts. Regarding the survey, the first three questions were based on the PDUQ, which has not been validated as an opioid use disorder screening tool in the palliative care population. The remaining questions all had a similar structure where the participants were asked to respond “yes” or “no” to a statement. These dichotomous questions may not have captured the complexities of the constructs that they intended to measure.
Lastly, the findings of this single-site study may not be generalizable to other settings and populations outside of the OPCC. However, this limitation may be mitigated because the OPCC is a high-volume clinic where nine palliative care physicians see ∼1500 new patients on an annual basis. In addition, PM is an international referral center that accepts patients outside of Toronto.
Conclusion
This is the first Canadian study to describe opioid disposal practices in a palliative care context. There is a high prevalence of people with life-limiting illnesses who report that they do not routinely dispose their opioids. Medication waste can result in nonmedical use of opioids, opioid-related hospitalizations and deaths, negative environmental impacts, and significant economic costs. Further studies are required to improve understanding of opioid disposal in the context of palliative care, including the impact of patient education and best methods to disposal of opioids while still ensuring that patients have access to opioids for symptom management.
Footnotes
Acknowledgments
We would like to thank the Princess Margaret Cancer Centre palliative care nurses and physicians for their support of this study. This article presents the findings from Dr. Jenny Lau's Master of Science thesis project that is available online through ProQuest Dissertations Publishing.
Authors' Contributions
J.L.: Conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, visualization, and project administration. C.Z.: Conceptualization, methodology, resources, and writing—review and editing. P.S.: Conceptualization, methodology, resources, and writing—review and editing. A.D.F.: Conceptualization, methodology, resources, writing—review and editing, supervision, and project administration.
Funding Information
No funding was received for this article.
Author Disclosure Statement
A.D.F. receives an unrestricted educational grant to maintain the online opioid self-assessment program from the Canadian Generic Pharmaceutical Association (CGPA). The funding organization had no role in the preparation, review approval, or data analyses of the course content. A.D.F. is the inventor of the App Opioid Manager. The App is owned by UHN, the hospital where A.D.F. is, and A.D.F. does not receive any profits from the App sales. A.D.F. has a YouTube monetized channel and receives payment for advertisements on the channel. There are some videos related to opioids in her channel. All other authors report no competing interests.
Supplementary Material
Supplementary Appendix SA