
Abstract
Background:
Characteristics of patients undergoing outpatient evaluation for advanced cardiac therapies are largely unknown.
Objective:
To describe demographics, baseline quality of life, and frailty of patients undergoing evaluation for advanced therapies at the time of presentation for evaluation in an outpatient cardiac palliative care clinic and examine key quality of life differences across patients.
Design:
Retrospective chart review to report baseline demographics and quality of life.
Settings/Subjects:
Patients at a large academic medical center in the United States referred for advanced cardiac therapies in 2021.
Measurements:
Depression and anxiety were measured using the Hospital Anxiety and Depression Scale; quality of life was measured using the Functional Assessment of Chronic Illness Therapy–Palliative care (FACIT-Pal) tool; and frailty was measured using the Fried Frailty Phenotype. Differences in quality of life by disease etiology, demographic characteristics, and frailty were assessed.
Results:
Fifty-four patients were seen in the outpatient cardiac palliative care clinic for advanced therapy evaluation. Most were Caucasian (80%) and male (74%). Patients traveled an average of 61 minutes to the clinic. All but five lived in a rural, medically underserved, or health professional shortage area. Forty percent scored abnormal or borderline abnormal for anxiety; 22% scored abnormal or borderline abnormal for depression. The FACIT-Pal mean score was 129 (standard deviation 23), with emotional and functional well-being domains contributing most to poor quality of life. Seventy-one percent were frail. Patients with a nonischemic etiology had a 3.32 times higher rate of anxiety than nonischemic patients (95% confidence interval = 1.05–10.54, p = 0.041).
Conclusion:
As patients undergoing transplant evaluation have high levels of depression, anxiety, and frailty, interdisciplinary care teams will be needed to properly manage the needs of this complex population. These results can inform efforts to integrate palliative care into advanced cardiac therapy and improve patients' experiences.
Introduction
Advanced cardiac therapies, including mechanical circulatory support (MCS) and heart transplantation, are important treatments for a subset of patients with end-stage heart failure. In the United States, 3817 heart transplants were performed in 20211 and 3198 left ventricular assist device (LVAD) implantations were performed in 2019. 2 Patients being considered for MCS and/or transplantation undergo an interdisciplinary evaluation. Rigorous physical and psychosocial evaluations are performed to ensure patients are healthy enough to undergo the surgery and have the mental wellness, and psychosocial stability needed to be a candidate for these procedures. Owing to the high prevalence of symptoms and behavioral health needs among these patients, palliative care can be integral in evaluating and helping to address patients' needs throughout the advanced therapies journey. When integrated into transplant programs, palliative care providers play an important role in assessing patients' values and helping patients manage uncertainty when facing critical medical decisions. In this context, palliative care has been integral to interdisciplinary mechanical support teams, particularly since the Centers for Medicare and Medicaid Services mandated their involvement for LVAD evaluations in 2015. 3 Despite the requirement for palliative care integration into MCS teams, there is no explicit requirement for palliative care integration into cardiac transplantation. However, owing to the prevalence in MCS teams, palliative medicine providers have become more involved in this evaluation process in recent years, particularly in inpatient settings.4,5
Of note, patients with advanced heart failure are known to have high levels of anxiety and depression.6–8 However, although the Society of Thoracic Surgeons' INTERMACS Database collects some quality-of-life data, 2 detailed baseline data for patients undergoing evaluation for advanced therapies, including MCS and heart transplantation, are largely unpublished. In addition, as a significant proportion of these patients are evaluated in inpatient settings, little information is available about the characteristics and needs of patients evaluated for advanced cardiac therapies seen by palliative care in outpatient settings.
Funding and staffing outpatient cardiac palliative care clinics has proved challenging across the country, thus understanding baseline characteristics of outpatient cardiac transplant patients can help advance research in palliative care and help palliative care leaders advocate for interdisciplinary team care for these patients. Improving our knowledge about the characteristics of this complex patient population can help provider teams delivering care to this vulnerable group of patients to better manage symptoms, advocate for resources for outpatient cardiac palliative care, and develop efficient referral workflows.
With this aim in mind, we conducted a retrospective chart review of a cohort of heart transplant patients being seen in an outpatient palliative care clinic as part of their advanced cardiac therapy evaluation process. Our goal was to better understand their baseline functional characteristics, mental health status, and factors affecting social determinant of health and basic demographic characteristics. Statistical comparisons between patients with different disease etiology, frailty levels, and demographic characteristics were conducted to determine differences with potential clinical significance.
Methods
Study design
This study was conducted by reviewing the charts of patients referred for advanced cardiac therapy evaluation and seen in an outpatient cardiac palliative care clinic during 2021 at a large Midwestern academic medical center (AMC). All charts were reviewed by the primary author, a board-certified palliative care physician with 10 years of experience in cardiac palliative care, and involved recording whether the primary diagnosis concerned ischemic or nonischemic cardiomyopathy and values for quality-of-life indicators. The study was approved by the institutional review board of the AMC.
Study setting
The outpatient palliative care clinic described in this study has been in place for three years at the AMC and has been fully integrated into the advanced cardiac therapy evaluation process since January 2021. Descriptive characteristics of the outpatient clinic staffing and other aspects of the palliative care program, as suggested by Rogers et al., 9 are summarized in Table 1.
Characteristics of Academic Medical Center Cardiac Palliative Care Program
AMC, academic medical center; FTE, full-time equivalent.
Measures
Baseline quality of life was measured on different dimensions using the Hospital Anxiety and Depression Scale (HADS), the Functional Assessment of Chronic Illness Therapy–Palliative Care (FACIT-Pal) scale, and Fried's Standardized Phenotype of Frailty. The HADS anxiety and depression subscores range from 0 to 21, with higher scores indicating worse symptoms. The FACIT-Pal scale ranges from 0 to 184; the higher the score, the better the quality of life. Fried Frailty Phenotype was measured in each patient at the initial outpatient clinic visit using three subjective questions, a timed 15-foot walk, and an evaluation of hand grip strength with a dynamometer. 10 Fried Frailty Phenotype is the method of measuring frailty preferred by the American Society of Transplantation. 11
Demographic information was also recorded for each patient including age at the time of first visit, gender, race, religious preference, survival status, driving distance, whether they resided in a Medically Underserved Area (MUA) or Health Professional Shortage Area (HPSA), and whether they lived in a rural area. Etiology of the patient's heart failure was recorded in the demographics for comparison because ischemic and nonischemic cardiomyopathy can have varied age of onset and reflect different social determinants of health before diagnosis. Patients' residential addresses were used to determine whether patients lived in an MUA and/or an HPSA based on public data provided by the Health Resources and Services Administration. 12 Rural status definitions were provided by the Federal Office of Rural Health Policy. 13 Driving distance from the AMC was calculated using Google Maps during the clinic's hours of 08:00 AM to 05:00 PM.
Analysis
Statistical analysis was performed with R version 4.0.2. 14 Demographic and baseline data were analyzed using descriptive statistics including frequencies and means. An analysis of quality-of-life indicators and other characteristics comparing ischemic and nonischemic patients was performed using Fisher's exact tests, Pearson's chi-squared tests, and Wilcoxon rank sum tests. A proportional logistic regression model was used to test the relationship between primary diagnosis and the levels of anxiety and depression on the HADS scale. Pearson's chi-squared tests and Wilcoxon rank sum tests were used to analyze associations between Mental Health HPSA and patient anxiety, depression, emotional well-being, and FACIT-Pal total score.
Similarly, the association between gender and mental health status as measured by the indicators of anxiety, depression, and emotional well-being was tested using Fisher's exact test and Wilcoxon rank sum test. Finally, the relationship between frailty and the other quality-of-life indicators was explored by looking at the HADS anxiety and depression levels by the patient's level of frailty using Pearson's chi-squared tests and the FACIT-Pal total and social well-being subscale scores by the patient's level of frailty using Kruskal–Wallis tests.
For these tests, HADS scores were categorized as “normal” (scores 0–7), “borderline abnormal” (scores 8–10), or “abnormal” (scores 11–21); Fried's frailty scores were categorized as “not frail” (score of 0), “pre-frail” (scores 1–2), or “frail” (scores 3–5). A correlation analysis between the raw scores of the HADS and Fried's frailty scales, as well as the FACIT-Pal total and subcomponent scores, was carried out using Pearson's correlation coefficient with Holm-adjusted p values to account for multiple comparisons. 15 Missing values were handled by pairwise deletion and an alpha level of 0.05 was adopted throughout the analysis.
Results
Characteristics of patient population
Across the AMC, the heart transplant team received 108 referrals for heart transplant evaluation and successfully completed 43 transplants and 17 LVADs in calendar year 2021. Palliative care successfully completed 58 evaluations in the outpatient setting. This represented 54 unique patients and four reevaluations; the data from the reevaluations were not included in this study. The outpatient cohort had a mortality rate of 2% at the end of the calendar year.
Table 2 provides the demographics of the outpatient palliative care cohort. The average age was 57 years, and the majority of patients were identified as Caucasian (80%) and male (74%). Approximately one-third of patients lived in rural designated areas, and the average travel time to the outpatient clinic was 61 minutes. Thirteen percent of patients lived in an MUA and 43% lived in an HPSA-designated area that included mental health, dental, and primary care health professional shortages (Fig. 1). There were no significant differences in demographics between ischemic and nonischemic etiology of heart failure. We found no association between patient gender and mental well-being.
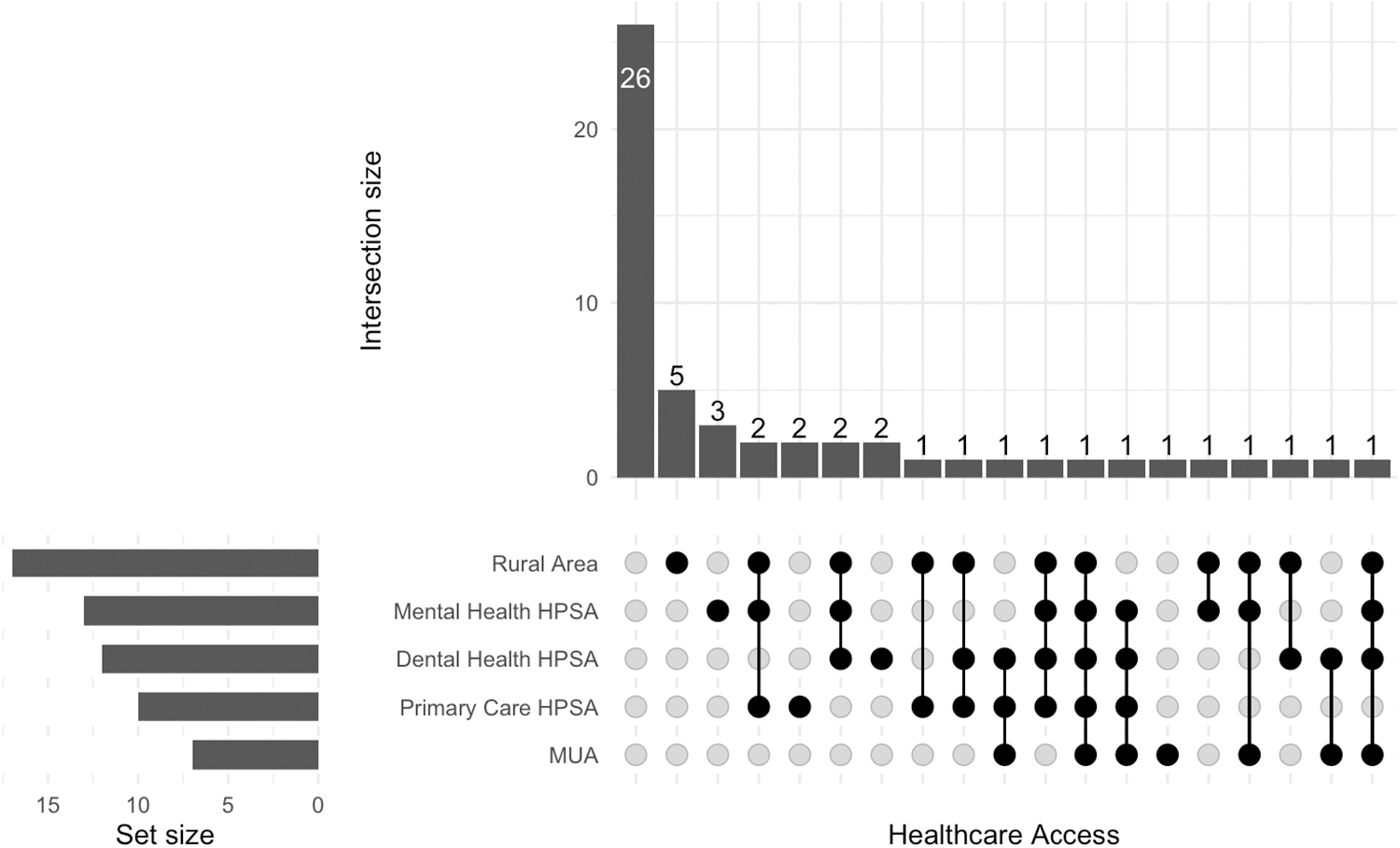
MUAs and HPSAs in outpatient palliative care patients undergoing evaluation for advanced cardiac therapies. Areas characterized by one or more of the rural, HPSA, or MUA designations. The intersection sizes of the vertical bar chart represent the number of patients living in areas featuring the combination of designations indicated by the dot matrix. The sets in the horizontal bar chart represent the total size of each designation. HPSA, Health Professional Shortage Area; MUA, Medically Underserved Area.
Demographics of Outpatient Palliative Care Patients Undergoing Evaluation for Advanced Cardiac Therapies
Fisher's exact test; Pearson's chi-squared test; Wilcoxon rank sum test.
CM, cardiomyopathy; SD, standard deviation.
Quality-of-life indicators
Baseline quality-of-life scores are summarized in Table 3. Forty percent of the sample had borderline or significant anxiety (HADS anxiety subscale [HADS-A] score >8) and 22% had borderline or significant depression (HADS depression subscale [HADS-D] score >8). For patients with a nonischemic diagnosis, the odds of having non-normal (i.e., borderline abnormal or abnormal) HADS-A score were 3.32 times higher than that for patients with an ischemic diagnosis (95% confidence interval = 1.05–10.54, p = 0.041). There were no statistically significant differences in HADS-D scores between the ischemic and nonischemic patient groups.
Quality of Life and Frailty in Outpatient Palliative Care Patients Undergoing Evaluation for Advanced Cardiac Therapies
Fisher's exact test; Wilcoxon rank sum test.
FACIT-Pal, Functional Assessment of Chronic Illness Therapy–Palliative care; HADS, Hospital Anxiety and Depression Scale.
FACIT-Pal scores and subscale scores are visualized in Figure 2. The FACIT-Pal mean score was 129 (range = 78–170, standard deviation = 23, with higher scores indicating a better quality of life) in our advanced therapies evaluation population. There were no significant differences in the quality-of-life indicators for patients in the ischemic and nonischemic groups.
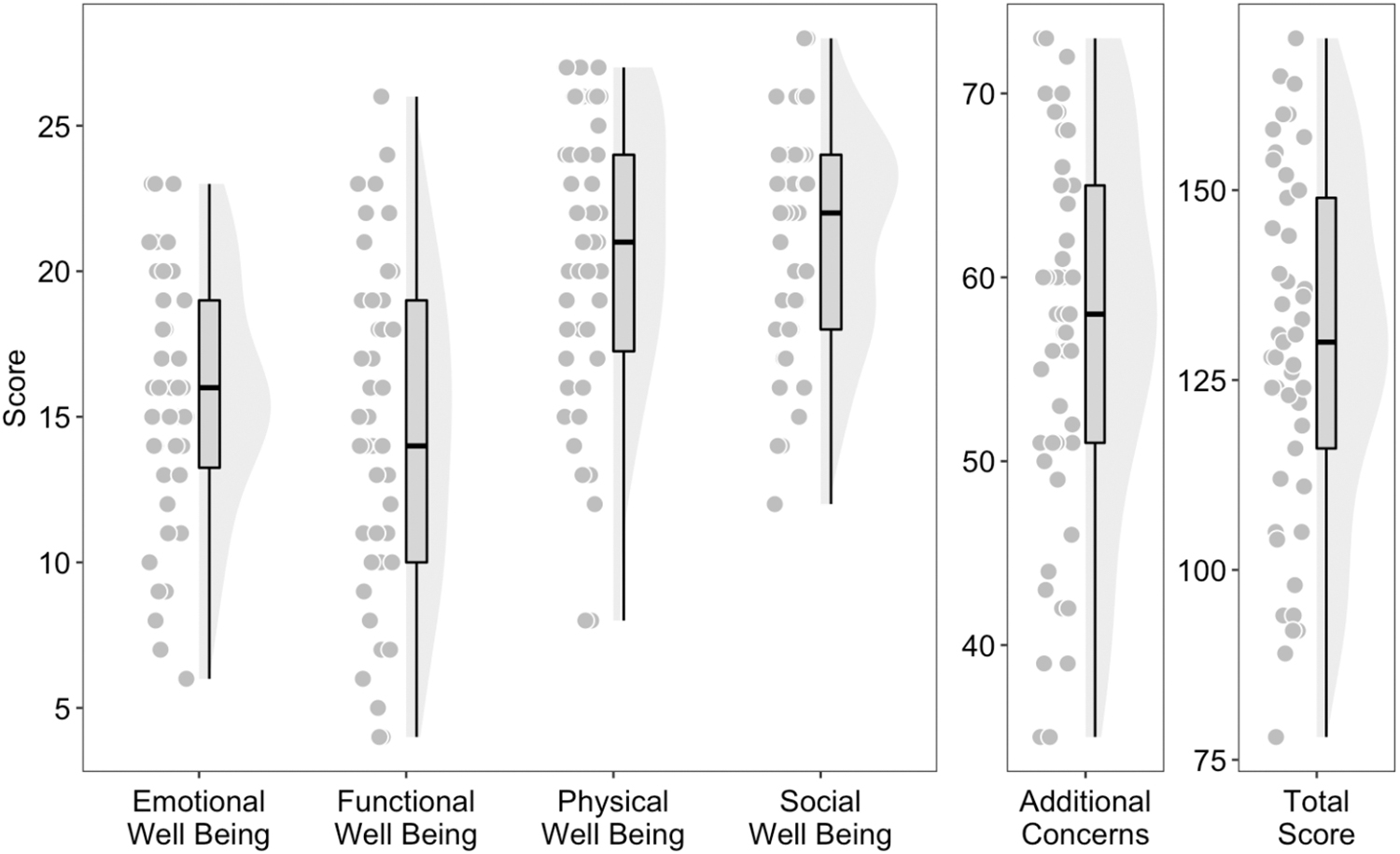
Distribution of FACIT-Pal scores and subscale scores. Subscale and total FACIT-Pal scores are summarized with boxplots. Each boxplot is augmented with the individual scores on the left and their full distribution on the right. Theoretical ranges for the emotional well-being subscale: 0–24; for the functional, physical and social well-being subscales: 0–28; for additional concerns: 0–76; for the total FACIT-Pal: 0–184. In all cases, a higher number indicates better quality of life. FACIT-Pal, Functional Assessment of Chronic Illness Therapy–Palliative care.
Seventy-one percent of patients were frail (Fried Frailty Phenotype score 3–5), and 25% were pre-frail (Fried Frailty Phenotype score 2–3) as given in Figure 3. Despite a higher prevalence of frailty in the nonischemic group, there was no statistical difference in frailty between ischemic and nonischemic etiologies. Patients who were frail had, however, significantly lower levels of social well-being as measured by the FACIT-Pal subscale [χ 2 (2) = 6.73, p = 0.03], as well as lower total FACIT-Pal scores [χ 2 (2) = 6.88, p = 0.03], but they had no differences in their levels of depression or anxiety.
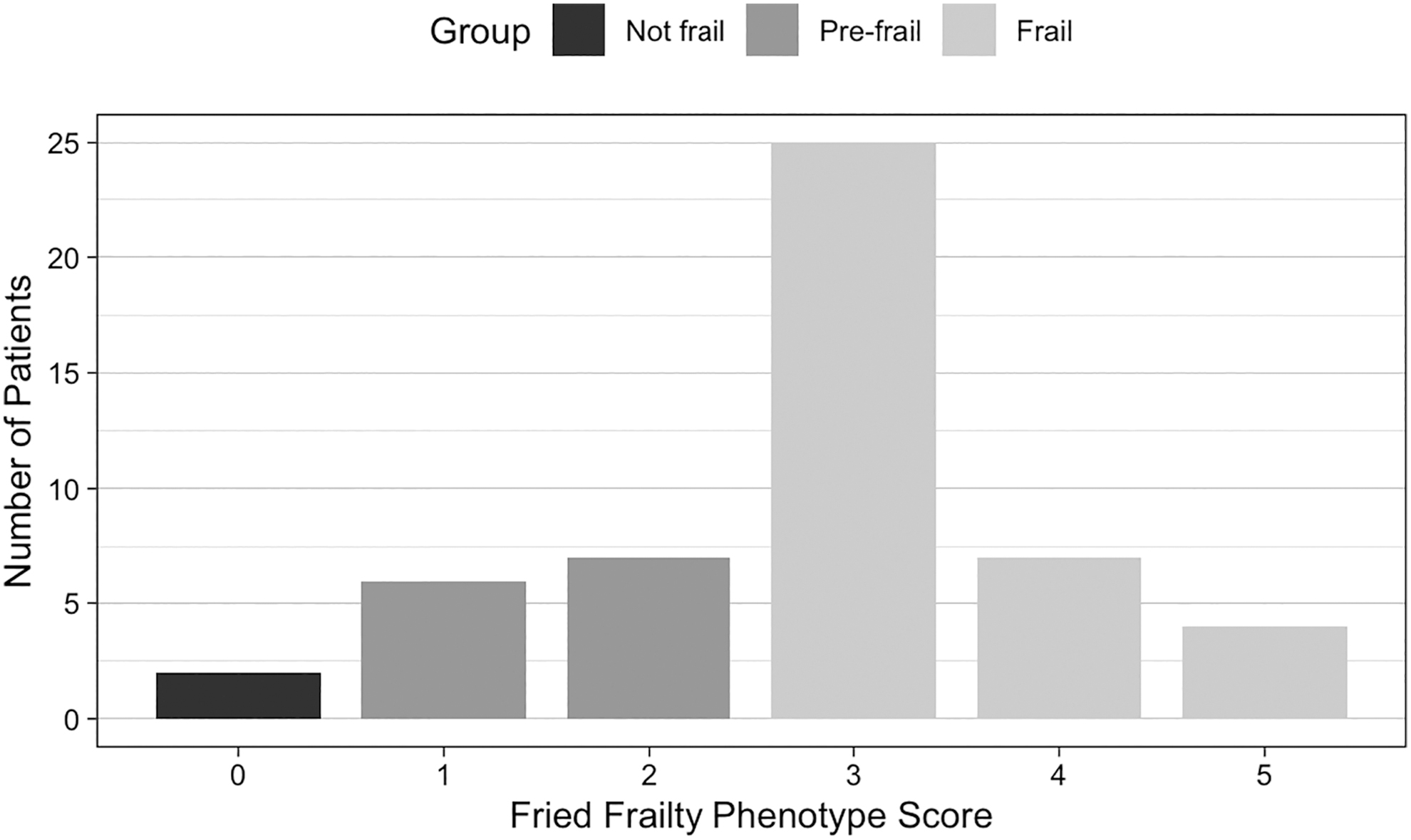
Fried frailty score. The distribution of Fried Frailty Phenotype scores are shown by vertical bars. A score of 0 = not frail; 1–2 = pre-frail; 3–5 = frail.
Discussion
We found that patients being evaluated for advanced cardiac therapies were overwhelmingly frail, had very high levels of psychopathology, and had overall poor quality of life, regardless of the etiology of their disease. The functional and emotional well-being subscales exhibited the lowest distribution range of scores among the four subscales that comprise overall quality of life (Fig. 2). In addition, the mean travel time to our clinic for this patient cohort was over one hour, with many patients traveling from MUAs, HPSAs, and rural areas suggesting such patients may face considerable barriers to health care access.
The rates of anxiety and depression in this cohort of patients were similar to those reported by others in the general heart failure population. 16 These findings are notable because the presence of psychopathology has been linked to increased rates of nonadherence, smoking, and poor dietary compliance. 17 In addition, depression is linked with increased postheart transplant mortality. 17 Furthermore, not only is depression linked with behavioral sources of adverse outcomes, but there is also a biochemical link between depression and heart failure, given that depression is associated with higher levels of inflammatory cytokines known to have direct negative inotropic effects. 18 With 22% of patients reporting depressive symptoms and 40% of patients reporting anxiety, these data suggest that it is critical that advanced therapy teams have access to mental health providers to provide counseling and medication management support for their patients.
With respect to quality of life, the mean FACIT-Pal score in our advanced therapies evaluation population was congruent with that of the usual care cohort of advanced heart failure patients in the Palliative Care in Heart Failure randomized controlled clinical trial. 7 However, in contrast to findings from that study, our cohort had higher social well-being scores. This is noteworthy because the presence of a reliable social support network is important for patients undergoing advanced cardiac therapies. 19
It is known that more frail patients have higher risks of mortality post-transplant, but with proper patient selection, the Fried Frailty Phenotype has been shown to improve following transplant intervention. 20 Although the use of frailty as a screening tool for transplant is controversial and not recommended,11,21 an important goal of advanced therapies is to select patients who have high likelihood of reversal of physiologic frailty post-transplant or MCS. As a result, a key role of the palliative care team can be to identify quality of life and frailty barriers that cannot be reversed with advanced therapies. Examples would be chronic pain syndromes or mental health disorders that limit mobility and contribute to continued frailty after post-transplant rehabilitation. Although coping with the gradual loss of function owing to increased frailty is a common topic discussed in outpatient cardiac palliative care clinics, having an interdisciplinary team to address these issues can help the care process.
Transplant centers are typically located at quaternary care centers in urban environments and often care for patients from large catchment areas. There are 115 active adult heart transplant centers in the United States 22 that serve an estimated 6,859,623 patients living with heart failure. 23 We found that the mean travel time to our clinic for this cohort of patients was over one hour, which can be a challenge for families facing large volumes of provider visits to receive advanced therapies. In addition, these patients have a high symptom burden, which can make travel challenging. The introduction of telehealth into outpatient palliative care clinics has been important but it may be insufficient owing to inconsistent access to Wi-Fi and technology needed to successfully complete telehealth visits.24,25 Of note, nearly half of the patients in our sample lived in areas with at least one HPSA or considered an MUA.
When considering outpatient palliative care services as part of evaluations for advanced cardiac therapies, it is important to consider the ratio of evaluations to successful transplants to budget and plan clinic schedules. In our cohort, we conducted 2.5 evaluations per heart transplant, and 60% of the patients were healthy enough to be seen in the outpatient setting. We hypothesize these rates will vary by institution, but considering these figures may be helpful when managing patient volume. Furthermore, the survival of this patient cohort was much higher than expected. The great majority of advanced therapy evaluation deaths occurred in patients being seen exclusively by the inpatient palliative care team, with only one death occurring in the outpatient cohort. This suggests that teams should consider planning for larger follow-up volumes than might be typically anticipated in a population with high mortality rates.
Our study has some limitations. First, this is a retrospective review of charts from a single clinic during a single year of operation. Given the timing of this study, the influence, if any, of the COVID-19 pandemic is unclear. Nonetheless, the rates of depression and anxiety in our population were similar to those reported for patients with heart failure in general.7,16 Second, our cardiac palliative care clinical programs are very mature, making it possible that our experience differs from institutions with less mature programs or those with fewer patients. Finally, our patient population reflects a Midwestern catchment area and underrepresents women and ethnic minorities who may have different characteristics and experiences. Of note, this underrepresentation of women is consistent with transplant programs across the nation as currently <25% of heart transplant recipients are women. A large U.S. cohort study conducted from 2004 to 2014 assessing the lack of survival differences between sexes showed 23.7% women in the 10-year cohort, which is consistent with our results. 26
Conclusions
This study found high rates of depression, anxiety, frailty, and impaired quality of life among patients seen by an outpatient palliative care program for patients undergoing advanced cardiac therapies evaluation. It will be important for providers to consider the mental health and other care needs this patient population will require as part of their treatments. The results of our study can help palliative care providers better understand the characteristics and needs of this complex patient population and inform efforts to support advanced cardiac therapy evaluation and improve outcomes for these patients.
Footnotes
Acknowledgments
T.A.B. would like to acknowledge The Center for the Advancement of Team Science, Analytics, and Systems Thinking in Health Services and Implementation Science Research (CATALYST) at The Ohio State University for helping the Division of Palliative Medicine expand their health services research and for being a pivotal part of this project. The authors thank the MAPI Research Trust for allowing the free use of the Hospital Anxiety and Depression Screen for unfunded research.
Authors' Contributions
All authors contributed to the study design, data analysis, and writing of this article.
Funding Information
The authors have no funding to report for this study.
Author Disclosure Statement
T.A.B. is a member of the Finance Committee of the American Academy of Hospice and Palliative Medicine. All other authors have no conflicts of interest to disclose.