
Abstract
Background:
Racial and ethnic minoritized people with dementia (PWD) are at high risk of disenrollment from hospice, yet little is known about the relationship between hospice quality and racial disparities in disenrollment among PWD.
Objective:
To assess the association between race and disenrollment between and within hospice quality categories in PWD.
Design/Setting/Subjects:
Retrospective cohort study of 100% Medicare beneficiaries 65+ enrolled in hospice with a principal diagnosis of dementia, July 2012–December 2017. Race and ethnicity (White/Black/Hispanic/Asian and Pacific Islander [AAPI]) was assessed with the Research Triangle Institute (RTI) algorithm. Hospice quality was assessed with the publicly-available Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey item on overall hospice rating, including a category for hospices exempt from public reporting (unrated).
Results:
The sample included 673,102 PWD (mean age 86, 66% female, 85% White, 7.3% Black, 6.3% Hispanic, 1.6% AAPI) enrolled in 4371 hospices nationwide. Likelihood of disenrollment was higher in hospices in the lowest quartile of quality ratings (vs. highest quartile) for both White (adjusted odds ratio [AOR] 1.12 [95% confidence interval 1.06–1.19]) and minoritized PWD (AOR range 1.2–1.3) and was substantially higher in unrated hospices (AOR range 1.8–2.0). Within both low- and high-quality hospices, minoritized PWD were more likely to be disenrolled compared with White PWD (AOR range 1.18–1.45).
Conclusions:
Hospice quality predicts disenrollment, but does not fully explain disparities in disenrollment for minoritized PWD. Efforts to improve racial equity in hospice should focus both on increasing equity in access to high-quality hospices and improving care for racial minoritized PWD in all hospices.
Introduction
More than 30% of U.S. decedents die with or from dementia and almost half of the hospice recipients have dementia. 1 At the same time, the decedent population in the United States is becoming more racially and ethnically diverse. Yet, racial and ethnic minoritized people with dementia (PWD) are less likely to enroll in hospice at end of life and those who do are more likely to experience burdensome transitions following hospice enrollment, including hospice disenrollment.2–11 Disenrollment interrupts care continuity and limits access to interdisciplinary palliative care services at end of life. 12 Moreover, disenrollment may signify that hospice providers are either enrolling marginally eligible individuals or are attempting to avoid paying for higher cost services that support optimal patient care.13–20
Improving racial equity and reducing disparities in hospice is a major priority for the Centers for Medicare and Medicaid Services (CMS), the primary payor for hospice in the United States. 21 Bolstering evidence on the relationship between hospice quality and racial disparities in hospice disenrollment for PWD can help inform these efforts. This has become feasible since activities to measure and report hospice quality have intensified in recent years. Since 2015, hospices have been required to report quality metrics or face financial penalties, and public reporting of hospice quality began in 2018. 22
It is not well understood if known racial disparities in disenrollment among PWD are due to sorting of minoritized groups into lower quality hospices or if disparities persist across the spectrum of hospice quality. Previous studies have found that racial minoritized individuals are more likely to receive care from lower quality health care facilities, including hospitals, nursing homes, home health, and hospice.23–27 However, studies also show that racial and ethnic minoritized individuals tend to have worse outcomes within the same facility/provider.28–30 In the hospice setting, Black hospice recipients had higher rates of transitions to the emergency department and hospital than White recipients within the same hospice, although they were not more likely to be enrolled in hospices with higher transition rates. 31
Determining whether racial and ethnic minoritized PWD are more likely to be enrolled in hospices with high rates of disenrollment—or whether disparities persist across all hospices—can help identify targets for policy or regulatory changes. The objective of our study was to characterize the association between hospice quality and racial disparities in disenrollment among PWD. Specifically, we sought to assess disparities in disenrollment between low- and high-quality hospices, as well as within hospices with similar quality ratings.
Methods
Study design, data sources, participants
This retrospective cohort study used data from 100% Medicare hospice fee-for-service claims, the Medicare Beneficiary Summary File (MBSF), Hospice Provider of Service File, Hospice Public Use File, Neighborhood Atlas, and publicly reported data from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey for Hospice.
The CAHPS survey was used to determine the quality ratings of the hospices in our study. The CAHPS survey is a 47-item questionnaire that is sent to the primary informal caregiver of the hospice decedent and includes questions about the hospice care experience, such as symptom management and hospice team communication. It is administered via telephone, mail, or mixed and is available in eight languages. Survey response rates range from 30% to 35%. Hospices are required to participate in quality reporting or face a 2% financial penalty. Public reporting is mandatory for all Medicare certified hospices with the exception that hospices are not required to participate in the first year after opening, if they have fewer than 30 completed surveys over 8 quarters, or if they have fewer than 50 survey eligible decedents in the prior calendar year. Publicly reported scores are averaged over the previous eight quarters and are case-mix adjusted for decedent age, payor, primary diagnosis, length of stay of the final episode of care, caregiver age, education, relationship with the decedent, Spanish language, and response percentile. More information on the psychometric properties of the CAHPS survey is available elsewhere.32–34
Individuals in our sample included Medicare beneficiaries enrolled in the Medicare Hospice Benefit with a principal diagnosis of alzheimer's disease or related dementia (ADRD) based on codes in the International Classification of Disease, 9th and 10th revisions, who had their index hospice admission between July 2012 and December 2015 (n = 693,165), which allowed for two years of follow up for all individuals in our sample. We excluded individuals younger than 65 (n = 10,681), those missing information on their final disposition (n = 4354), and individuals classified as native American (n = 1731) due to small sample sizes when stratified by hospice quality category or other/unknown (n = 3297) due to a lack of specificity. The hospice provider for each individual in our cohort was identified using the hospice provider ID variable in the hospice claims file, which was used to link to data on hospice provider characteristics.
Measures
Hospice disenrollment
Our primary outcome was disenrollment from hospice alive. Disenrollment can either be hospice-initiated or patient-initiated.35,36 We used a previously described algorithm3 using disposition codes available in the hospice claim file to identify disenrollment (for any reason) and included the first disenrollment that occurred within two years of index hospice admission.
Race and ethnicity
Race and ethnicity (non-Hispanic White/non-Hispanic Black/Hispanic/Asian and Pacific Islander [AAPI]) was identified in the MBSF using the Research Triangle Institute (RTI) race variable. This variable was developed by the RTI using an algorithm that includes data from the Medicare Enrollment Database combined with lists of Hispanic and AAPI last names from the U.S. Census as well as residence information. The RTI algorithm was developed to address deficiencies in the Medicare Enrollment Database race measure, which is known to severely undercount people from Hispanic or AAPI backgrounds. The RTI measure has a sensitivity of 76.6% for Hispanics and 79.2% for AAPI and kappa coefficients reaching 0.8. 37
Hospice quality
We used CAHPS survey data from the May 2018 reporting period to sort hospices into quality categories. CAHPS measures are reported as top, middle, and bottom box values that add up to 100%. We used top-box scores on the single-item measure “How would you rate this hospice on a scale of 1 to 10?” as the primary quality measure. Top box scores for hospices for this measure ranged from 50% to 98% for the hospices in our study. We used this information to create quartiles of hospice quality. For example, in the lowest rated quartile, 50%–77% of survey respondents rated their hospice a 9 or 10, whereas in the highest rated quartile, 85%–98% of survey respondents rated their hospice a 9 or 10. We also included a category for hospices that had no quality measures reported because that hospice did not meet reporting requirements (unrated hospices).
Covariates
Other patient characteristics included patient age, sex, Medicaid dual-eligible, Medicare Part C enrollee, number of comorbidities (0–2/3–4/5+), residence type where hospice was received (home/assisted living/nursing home/other), rural/urban, area deprivation index rank, and census region. Hospice organizational characteristics include years in operation, number of beneficiaries, ownership (nonprofit/for-profit, government/other), and proportion of dementia patients. More information on how these variables were constructed is available elsewhere. 3
Analysis
We summarized the characteristics of hospice enrollees with dementia and the hospice agencies that cared for them and compared characteristics by hospice quality category and race categories using ANOVA or chi-square tests, as appropriate. To estimate and visually depict racial differences in disenrollment across hospice quality categories, we estimated a multilevel mixed-effects logistic regression model. We first estimated a model that included hospice quality and race specified as fixed effects, an interaction term for race and hospice quality, and hospice providers specified as random intercepts (null model). We then estimated a model that adjusted for patient case-mix and hospice organizational characteristics (fully adjusted model). In post hoc analyses, we estimated predicted probabilities of disenrollment by race in the different hospice quality categories for both the null and fully adjusted models.
To estimate the magnitude of between versus within hospice disparities, we calculated adjusted odds ratios (AORs) comparing odds of disenrollment between hospice quality categories by race and ethnicity (i.e., comparing Black PWD in low-quality hospices with Black PWD in high-quality hospices) and also adjusted odds of disenrollment within hospice quality categories by race (i.e., comparing Black PWD in high-quality hospices with White PWD in high-quality hospices), including adjusted for case-mix and hospice organizational characteristics.
Data on hospice organizational characteristics (e.g., size and proportion of dementia patients) were missing for some hospices, especially hospices that fell into the unrated quality category. These data are voluntarily reported by hospices and thus are not missing at random, and so, we opted against an imputation approach for these missing data. Instead, we included these data in a “missing” category for those variables.
We used SAS Version 9.4 (SAS Institute) and Stata Version 17 (StataCorp, LLC) for all analyses. This study was approved by the University of California, San Francisco, and the Center for Medicare and Medicaid Services Privacy Boards.
Results
Characteristics of hospice agencies and patients
There were 673,102 individuals in 4371 hospices who met the inclusion criteria as follows: 571,203 (85%) were White, 49,403 (7.3%) were Black, 42,061 (6.3%) were Hispanic, and 10,435 (1.6%) were AAPI (Table 1). The case-mix of the hospices varied across quality categories. For example, 90.3% of patients in the highest quality quartile were White compared with 79.4% in the lowest quartile, while Hispanics comprised 2.4% of patients in the highest quartile and 9.7% of the lowest quartile (p < 0.001). The organizational characteristics of the hospice agencies differed by quality category. Hospices in the lowest quality and unrated categories tended to be newer and have for-profit ownership compared with the highest quality hospices (Table 2). Hospices in the lowest quality quartile tended to be largest hospices (34.5%) compared with the highest quality category (19.1%), while unrated hospices were more often in the smallest hospice category (48.2%) (p = < 0.001).
Case-Mix and Service Use Patterns Across Hospice Quality Categories
Based on CAHPS survey for the proportion of respondents rating hospice 9 or 10 out on a scale of 1–10, where 10 is best.
p-Values compare lowest to highest quality category.
AAPI, Asian and Pacific Islander; CAHPS, Consumer Assessment of Healthcare Providers and Systems; IQR, interquartile rage; LOS, length of stay.
Organizational Characteristics of Hospices Across Quality Categories
Based on the CAHPS survey for the proportion of respondents rating hospice 9 or 10 out on a scale of 1–10, where 10 is best.
p-Values compare lowest to highest quality category.
Number of beneficiaries per year.
Sociodemographic characteristics and characteristics of the hospices where care was received by race and ethnicity are shown in Supplementary Appendix Table SA1.
In unadjusted analyses, almost one in five (19.4%) individuals in our cohort were disenrolled alive. The unadjusted proportion disenrolled varied from 16.4% in the highest quality hospices to 19.9% in the lowest quality quartile to 34.0% in unrated hospices (Table 1). Racial and ethnic differences in disenrollment ranged from 18.1% of White PWD compared with 25.6% of Black PWD, 25.3% of Hispanic PWD, and 25.1% of AAPI PWD (Supplementary Appendix Table SA1).
Predicted probabilities of disenrollment
Fully adjusted predicted probabilities of disenrollment by race across hospice quality categories are shown in Figure 1 and Supplementary Appendix Table SA2. The predicted probability of disenrollment ranged from 16.5% (95% confidence interval [CI] 15.9–17.2) for White PWD in the highest quality hospices to 32.3% (30.8–33.9) for Black PWD in unrated hospices. Fully adjusted predicted probabilities were attenuated from the null model values, particularly for the unrated hospice category (Supplementary Appendix Table SA3). The interaction term for race and hospice quality was statistically significant (p = 0.02), with some indication that differences in disenrollment between races were higher in the lower quality and unrated hospices, but CIs were overlapping.
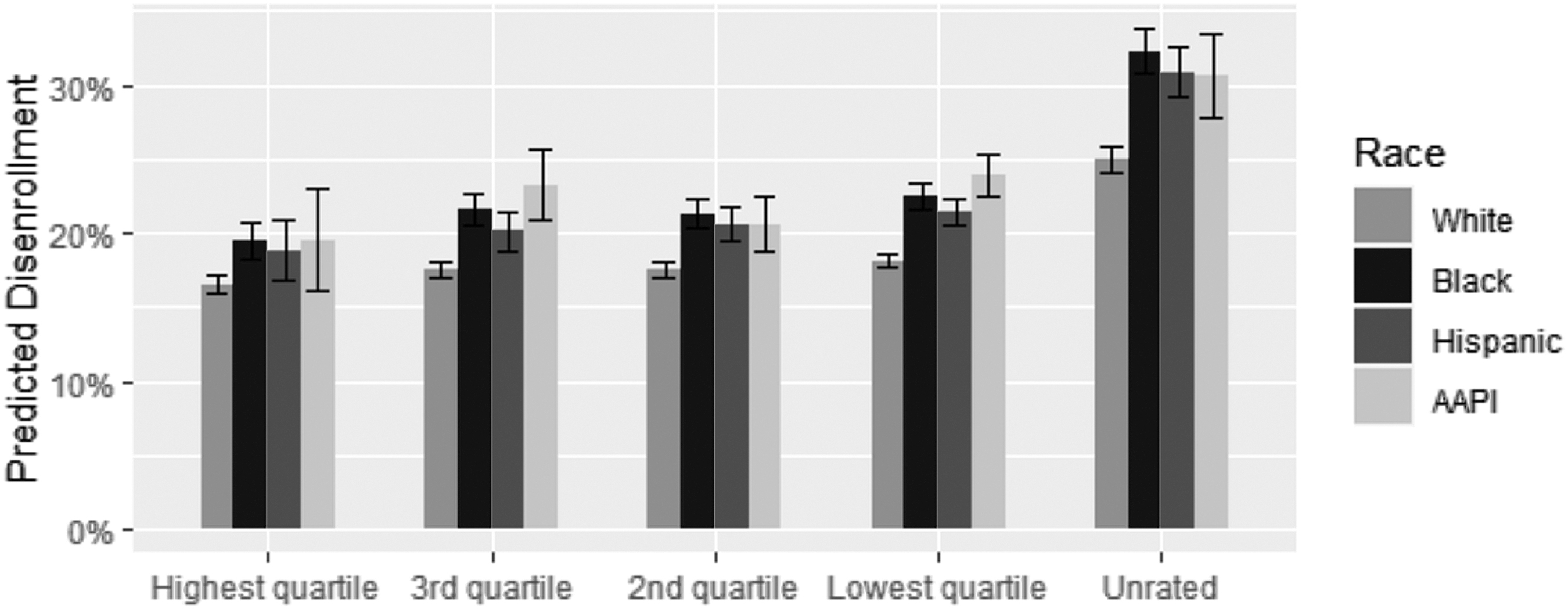
Adjusted predicted probability of disenrollment by race and hospice quality. Hospice quality is assessed using the CAHPS survey for the proportion of respondents rating a hospice 9 or 10 out on a scale of 1–10, where 10 is best. Predicted probabilities are estimated using a multilevel mixed-effects model that includes a random intercept for hospice, fixed effects for hospice quality and race, an interaction term for hospice and race, and are adjusted for hospice case-mix (age, gender, insurance status, comorbidities, residence type, rurality, area deprivation, region) and hospice organizational characteristics (years in operation size, ownership, and proportion of dementia patients). AAPI, Asian and Pacific Islander; CAHPS, Consumer Assessment of Healthcare Providers and Systems.
Between-hospice quality category comparison
AOR of disenrollment for White PWD in the lowest compared with highest quality quartile was 1.12 (95% CI 1.06–1.19); for Black PWD AOR was 1.2 (95% CI 1.09–1.32); for Hispanic PWD 1.2 (95% CI 1.0–1.4); and for AAPI PWD 1.3 (95% CI 1.0–1.6) (Table 3). The AOR for unrated hospices was substantially higher for all groups: White PWD 1.7 (95% CI 1.6–1.83); Black PWD 2.0 (95% CI 1.8–2.2); Hispanic PWD 2.0 (95% CI 1.6–2.3); and AAPI PWD 1.9 (95% CI 1.4–2.4).
Adjusted Odds (95% Confidence Interval) of Disenrollment Between Hospice Quality Categories Among White, Black, Hispanic, and Asian and Pacific Islander Hospice Enrollees With Dementia
Models include a random intercept for hospice, fixed effects for hospice quality and race, an interaction term for hospice quality and race, and are adjusted for hospice case-mix (age, gender, insurance status, comorbidities, residence type, rurality, area deprivation, region) and hospice organizational characteristics (years in operation size, ownership, and proportion of dementia patients).
Within-hospice quality category comparisons
Within the same hospice quality categories, racial minoritized PWD had consistently higher probability of disenrollment compared with White PWD (Table 4). In the highest quality quartile, the AOR was 1.23 (95% CI 1.1–1.3) for Black PWD and 1.18 (95% CI 1.02–1.34) for Hispanic PWD. For AAPI, the point estimate was higher at 1.24, although the 95% CI crossed 1 (95% CI 0.95–1.52).
Adjusted Odds (95% Confidence Interval) of Disenrollment in Racial and Ethnic Minoritized (Compared With White) Hospice Enrollees With Dementia Within Hospice Quality Categories
Models include a random intercept for hospice, fixed effects for hospice quality and race, an interaction term for hospice quality and race, and are adjusted for hospice case-mix (age, gender, insurance status, comorbidities, residence type, rurality, area deprivation, region) and hospice organizational characteristics (years in operation size, ownership, and proportion of dementia patients).
Discussion
All people deserve access to high-quality care at end of life. 38 Understanding drivers of racial disparities in hospice use patterns and care quality for the growing dementia population is a major priority for society generally and federal payors specifically. In this study of Medicare hospice recipients with dementia, our results indicate that the racial disparities in disenrollment among PWD may be driven by both sorting of racial and ethnic minoritized groups into lower quality or unrated hospices—which tend to have higher disenrollment rates—and also that disparities persist within both low- and high-quality hospices.
Our findings highlight institutionalized racism and discrimination that limits access to high-quality hospice care for racial and ethnic minoritized PWD and results in worse care quality within both high- and low-quality hospices. More research is needed to untangle how these disparities arise. One possibility is that discriminatory policies that reinforce residential segregation have resulted in geographic disparities in access to high-quality hospices. This has been shown to be the case for many other types of health outcomes and service use, and was made even more obvious by COVID-19.39–48 However, a study of home health found that even within the same neighborhood, racial and ethnic minoritized individuals were more likely to receive care from lower quality agencies. 25 Since home health and hospice clinicians visit patients in their home, the geographic forces that sort minoritized patients into hospitals and clinics in closer physical proximity to patients may be less prominent for home health and hospice.
Whether racial minoritized PWD are enrolling in lower quality hospices in the same geographic region or neighborhood requires further inquiry. If that is the case, it will be important to determine whether selective enrollment is due to hospice organizational factors (e.g., targeted outreach by low-quality providers to minoritized groups, especially those with dementia), community provider factors (e.g., referral patterns from clinicians), or patient factors (e.g., limited access to information about hospice quality). Previous research has shown that for-profit and lower quality hospices served higher proportions of racial and ethnic minoritized groups and patients with dementia, and similar incentives for expanded enrollment may be at play for lower quality hospices. 49
More research is needed to understand why racial and ethnic minoritized PWD have higher disenrollment rates than White PWD in both low- and high-quality hospices. Some possible explanations include implicit and explicit bias from staff who lack adequate training in culturally responsive care.50–52 Supporting this hypothesis is previous research showing that Black and Hispanic patients report lower scores on getting emotional and religious support within the same hospice. 23 A historical legacy of racism in health care may result in racial and ethnic minoritized groups being more hesitant about the hospice eligibility requirement to forgo disease-directed treatments, leading to revocation and hospitalization in the face of a health crisis. 53
The Hospice Quality Reporting Program (HQRP) is relatively new and continues to evolve. 21 Our findings add to prior evidence for both strengths and weaknesses of the current version of the HQRP and specifically the CAHPS survey.54–57 Although differences in disenrollment between hospice quality categories were not large, the fact that disenrollment increased as hospice quality decreased indicates that the CAHPS survey may assess the hospice organization's ability to support patients and families through the end-of-life period. On the contrary, the publicly reported measure, which does not stratify by race, might miss the nuance when it comes to the experience of racial and minoritized patients. It was also notable that disenrollment was substantially higher in the unrated hospices, which accounted for one-third of all hospice providers and care received by almost 10% of individuals in our sample. Providers and consumers going to the Care Compare website will have limited information about these hospices, some of which may have the most concerning practices of disenrollment. This may further exacerbate inequities for disadvantaged groups, who may already experience difficulties accessing web-based Care Compare data. 58
Our findings have policy implications for addressing racial disparities in disenrollment from hospice for PWD. At the policy level, regulators can try to increase access to high-quality hospices for racial and ethnic minoritized PWD through financial incentives for serving more racial and ethnic minoritized individuals.59,60 This may also allow hospices to provide more disease-directed treatments for patients concurrently with palliative treatments, which may enable continued enrollment. At the same time, they could enhance scrutiny on practices in lower quality hospices through increased audits. As the HQRP continues to evolve, policymakers should be ensuring that equity is a component of measurement and there are no unintended consequences of worsened racial disparities, as has been found for nursing homes. 61 Policymakers can also require that hospice organizations invest in efforts to provide equitable care, such as by mandating clinician training in culturally responsive care.
This study has limitations. The CAHPS survey has low response rates and may be subject to selection bias. However, the publicly reported values are already adjusted for response percentile for the hospice provider. 32 The RTI race measure is based on an algorithm rather than self-report, which is considered the gold standard for assessing race and ethnicity. In addition, race categories are broad and there are no options for mixed race. However, the RTI measure has been shown to have adequate accuracy for assessing race and is considered a better alternative to the other race measure available in Medicare data. 62 Finally, we used the CAHPS data reported in 2018, which are based on hospice survey results from 2016 to 2018, while patient data included enrollments between 2012 and 2017, and so, it is possible that the quality of the hospice was different than when patients received care.
In conclusion, hospice disenrollment decreases continuity of care and deprives seriously ill individuals of access to holistic and interdisciplinary palliative care when they are at their most vulnerable. It is unjust that racial and ethnic minoritized PWD are more likely to be disenrolled than White PWD. While higher disenrollment rates may be, in part, due to sorting of racial and ethnic minoritized PWD into lower quality and unrated hospices, we found a higher probability of disenrollment for racially minoritized PWD in both low- and high-quality hospices. Policy interventions should be aimed at increasing access to high-quality hospices for racial and ethnic minoritized PWD, and also ensuring that investments are made in improving care equity across all hospices.
Footnotes
Authors' Contributions
Funding acquisition (L.J.H. and K.Y.); conceptualization and study design (all the authors); analysis (L.J.H., S.G., and W.J.B.); article drafting (L.J.H.); article review and editing (all the authors); and final approval of the article (all the authors).
Funding Information
This study was supported by the National Institute on Aging (P01AG066605 and P30AG04428). L.J.H. is supported by the National Institute on Aging (K76AG074924). A.K.S. is supported by the National Institute on Aging (K24AG068312). K.Y. is supported by the National Institute on Aging (5R35AG071916). M.D.A. is supported by the National Institute on Aging (K07AG060270). K.L.H. is supported by the National Institute on Aging (5K01AG059831). A.L. is supported by the National Institute on Aging (5K01AG073532
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.