
Abstract
Background:
It is essential to establish both the appropriateness of palliative care (PC) and the prognosis in daily clinical practice to guide decision making in the management of older people with multiple advanced chronic diseases.
Objectives:
We assessed patients who were appropriate for PC using the NECPAL tool in a hospitalized older population and then we investigated its predictive validity on one-year mortality compared with the multidimensional prognostic index (MPI), a validated geriatric prognostic tool.
Design:
Prospective cohort study.
Setting/Subjects:
We enrolled 103 older adults hospitalized for acute medical and surgical conditions in a geriatric hospital in Italy.
Measurements:
The variables of interest were obtained at baseline through interviews of the ward medical staff and by consulting the computerized medical records. Long-term mortality (one-year) was assessed through the analysis of data acquired from hospital or territorial databases or through telephone contact with caregivers.
Results:
Mean age was 86.8 ± 7.2 years, with a female prevalence of 54.4%. Prevalence of NECPAL+ patients was 65.1%. MPI low risk: 30.1%; moderate risk: 41.7%; severe risk: 28.2%. Patients deceased during follow-up were 54.4%. NECPAL+ patients were more likely to die, even after adjusting for age, sex, and MPI score (hazard ratio [HR] 2.7, p = 0.020). All the NECPAL categories were associated with one-year mortality. MPI showed a better predictive power than NECPAL (area under the curve [AUC] 0.85 vs. 0.75, p = 0.030). After the exclusion of “Comorbidity: ≥2 concurrent diseases” item from NECPAL, its AUC increased to 0.78 with no statistically significant differences from MPI (p = 0.122).
Conclusions:
NECPAL is useful to identify the appropriateness of PC in hospitalized older adults, also allowing to predict long-term mortality with a performance similar to that of a validated geriatric prognostic tool.
Introduction
Ademographic shift has occurred over the last decades in developed countries, resulting in a considerably increased number of older people affected by chronic conditions. 1 Prognostic predictors are needed in daily clinical practice to guide decision making regarding clinical management, discharge plan, therapies, and follow-up of patients. This is particularly true in older patients with multimorbidity. 2 These patients, often affected by advanced chronic diseases and frailty, are at high risk of rapid deterioration of health and functional status. In this setting, the goal of care should be to plan programs of palliative care (PC), already in an early stage of the chronic disease to be combined with specific treatments. 3 Since both short-term and long-term mortality in older subjects result from a combination of biological, functional, psychological, pathological, and environmental factors, prognostic tools should imply a multidimensional approach.4,5
The NECPAL CCOMS-ICO© (NECesidades PALiativas—WHO Collaborating Center for Public Health Palliative Care—WHOCC at the Catalan Institute of Oncology—hereafter NECPAL) is a tool used to identify patients who are appropriate for PC, 6 supporting the clinicians in the development of an integrated care plan able to comprehend the global needs of the patient. The NECPAL is a flexible tool that provides both quantitative and qualitative assessments. It allows a multifactorial and nondichotomous evaluation process that combines subjective perception (surprise question [SQ]) with several other objective parameters (request and need, assessment of the disease severity and its progression, geriatric syndromes, psychosocial factors, use of health resources, comorbidities, and specific pathology indicators). 7 The NECPAL can be used in several areas of the health care system. 8 The ability of this tool to define the appropriateness of PC, coupled with its ability to assess prognosis,9,10 could be valuable also in the geriatric setting characterized by multimorbidity.
Nevertheless, it has been rarely applied in the hospitalized older population. Therefore, the aim of our study was to evaluate the prevalence of patients who could be appropriate for PC using the NECPAL tool in hospitalized older multimorbid patients. Then, we also explored the predictive validity of NECPAL on one-year mortality, comparing it to a validated geriatric prognostic tool, to investigate whether it could be useful also in this peculiar setting never studied before.
Materials and Methods
Study design and population
We performed a prospective study on 103 older adults admitted for acute medical and surgical diseases to the Italian National Institute of Health and Science on Aging (IRCCS INRCA) of Ancona (Italy), which is a unique institute specifically focused on geriatric care and gerontological research in Italy. Indeed, our hospital is dedicated to scientific research and care of older subjects (mostly aged 80 years or older), which are usually still excluded from clinical trials and in which scientific evidence is still scarce. The hospital has 179 beds at full capacity. We took into account the following inclusion criteria: age ≥75 years, patients admitted to medical or surgical wards for acute conditions, and informed consent to the participation of study and data collection. We also took into account the following exclusion criteria: patients in imminent state of death, and patients admitted to rehabilitation ward, given the absence of acute diseases in this setting. We enrolled patients who were hospitalized on June 24, 2019 in the following wards: Internal Medicine and Geriatrics (n = 43), Surgery units (General Surgery, Vascular Surgery, Urologic Surgery, Diabetic Foot Surgery) (n = 17), Cardiology (n = 21), and Postacute Care (n = 22).
All data needed for the analyses were collected and recorded on June 24, 2019 and thereafter in the following 48 hours. All patients, or their legal representatives, gave their written informed consent and clinical investigations have been conducted according to the principles expressed in the Declaration of Helsinki as revised in 2013. This observational study was approved by the local Institutional Ethics Committee (Comitato Etico INRCA).
Proceedings
At baseline, all the variables of interest, including the patients' characteristics and variables related to the NECPAL tool, were obtained by dedicated physicians through interviews of the ward medical staff and by consulting the computerized medical records, after an adequate training. The same evaluating physician conducted the interviews with the ward medical staff in each unit. All physicians involved in the data collection have been properly trained and all the definitions, the procedures, and the measures were standardized to reduce systematic errors. Along with the NECPAL assessment, the multidimensional prognostic index (MPI), which is a geriatric validated prognostic scale, 11 was also performed.
One-year mortality was assessed through the analysis of data acquired from hospital or territorial databases or through home telephone contact with the caregivers.
The NECPAL tool
The NECPAL tool was developed as a joint initiative of the Qualy Observatory and the World Health Organization (WHO) Collaborating Center for Palliative Care Public Health Programs (QUALY/CCOMS-ICO) based on the experience of Prognostic Indicator Guidance (PIG-GSF) 12 and the Supportive and Palliative Care Indicators Tool (SPICT), 13 which was adapted and content-validated in clinical and cultural contexts of Catalonia (Spain), where the tool was developed. In this study, we used the updated version with reviewed and expanded contents. 14 The NECPAL is divided into four categories: (1) the SQ; (2) choice/demand or need of PC; (3) general clinical indicators of disease severity and progression, including comorbidity and resource use; and (4) disease-specific indicators (Supplementary Table S1). The SQ is a single question asked to the patient's physician about the patient's life expectancy estimate: “Would you be surprised if this patient dies within the next 12 months?.” Whenever the attending physician's answer was “no,” the patient was defined as SQ positive (SQ+). 15
Patients were defined as NECPAL positive (NECPAL+) if they resulted SQ+ and if they also tested positive to at least one of the other three categories. 14 NECPAL+ patients were considered appropriate for PC. Patients were then classified into two subgroups: NECPAL+ (defined as SQ+ plus at least another NECPAL category tested positive) and NECPAL− (defined as either SQ− or no other NECPAL category tested positive).
The MPI
The MPI is a validated geriatric prognostic tool based on the comprehensive geriatric assessment (CGA) and used in several settings.11,16 MPI consists of sixty-three items from the following eight domains: activities of daily living (ADL), instrumental activities of daily living (IADL), short portable mental status questionnaire (SPMSQ), mini nutritional assessment (MNA), Exton–Smith scale (ESS), cumulative illness rating scale (CIRS), number of medications, and social support network (Supplementary Table S2). According to the MPI, subjects were classified into three degrees of mortality risk at 12 months (low, moderate, and severe): low risk if the score ranged from 0 to 0.33; moderate risk if the score ranged from 0.34 to 0.66; and severe risk if the score ranged from 0.67 to 1.00. 11
Statistical analyses
Data were analyzed with the Statistical Package for Social Science version 21 (SPSS Inc., Chicago, IL, USA). A value of p < 0.05 was defined as statistically significant. Normal continuous variables were expressed as mean ± standard deviation. Skewed variables were expressed as median and interquartile range. Categorical variables were expressed as percentage. The χ 2 test was used to analyze the differences between categorical variables. The unpaired t test and Mann–Whitney tests were used to compare quantitative variables. Kaplan–Meier curves were drawn for one-year mortality and log-rank test was used to compare the different groups. Cox regression analysis was used to create adjusted models with age, sex, and MPI score (Model 1) and age, sex, ADL, IADL, SPMSQ, MNA, ESS (Model 2) as covariates. Adjusted model 2 was based on the variables of MPI that resulted significantly associated with mortality at univariate analysis. Log-minus-log plots were used to assess proportional hazards assumption. The receiver operating characteristic (ROC) curve was used to test the predictive performance on one-year mortality of both NECPAL and MPI.
Results
General characteristics
The mean age of the patients was 86.8 ± 7.2 years, with a female prevalence of 54.4%. Out of the 103 patients, 41.7% came from the Internal Medicine and Geriatrics Units, 20.4% from the Cardiology Unit, 16.5% from Surgery Units, and 21.4% from Postacute Care Facility.
The prevalence of NECPAL+ patients was 65.1% (67 patients). In particular, the percentages of patients tested positive in each NECPAL category were the following: 66.0% for SQ, 39.8% for category 2, 95.1% for category 3, and 60.2% for category 4. General characteristics of the study population according to NECPAL are described in Supplementary Table S3. NECPAL+ patients were older than NECPAL− patients, while there was no difference regarding sex between the two groups. In particular, patients who tested positive for SQ, categories 2 and 4 were older compared with patients who tested negative for the same categories (88.5 ± 6.6 vs. 83.5 ± 7.2 years, p = 0.001 for SQ; 89.4 ± 6.5 vs. 85.1 ± 7.1 years, p = 0.003 for category 2; 88.1 ± 6.8 vs. 84.9 ± 7.4 years, p = 0.024 for category 4, respectively), while no statistical difference was observed in mean age for category 3 (87.1 ± 6.9 vs. 81.1 ± 11.1 years, p = 0.068).
Regarding MPI, 30.1% of the study population was at low risk, 41.7% at moderate risk, and 28.2% at severe risk. The means of the points for each item of the MPI are described in Supplementary Tables S3 and S4. NECPAL+ patients were at higher risk according to MPI score compared with NECPAL− patients. NECPAL+ patients had worst scores at ADL, IADL, SPMSQ, MNA, and ESS, and they were also taking more drugs (Supplementary Table S3).
General characteristics according to sex are described in Supplementary Table S5. Females were younger than males, having higher risk at MPI and worst scores in several MPI subcategories, higher functional markers, enclosed in the category 3 of NECPAL, and higher burden of comorbidities.
One-year mortality
The median follow-up was 274 (38–395) days. Fifty-six patients (54.4%) died during follow-up. Deceased patients were older, tested more frequently positive in all the NECPAL categories, were more dependent in ADL and IADL, had worse cognitive function, higher risk of pressure sores, higher risk of malnutrition, and were more often institutionalized (Tables 1 and 2).
General Characteristics and NECPAL According to One-Year Mortality
p-Value for comparison between survivors and deceased. NECPAL has been defined positive (NECPAL+) if patients tested positive to SQ and if they also tested positive to at least one of the other three categories; Category 2 (choice/request or need): it is considered positive (+) if at least one of the subcategories tests positive; Category 3 (general clinical indicators of severity and progression): it is considered positive (+) if at least one of the subcategories tests positive; Category 4 (specific clinical indicators of severity and progression per diseases): it is considered positive (+) if at least one of the subcategories tests positive. See Supplementary Table S1 for details.
ALS, amyotrophic lateral sclerosis; GFR, glomerular filtration rate; SQ, surprise question (Would you be surprised if this patient dies within the next 12 months?).
Multidimensional Prognostic Index According to One-Year Mortality
p-Value for comparison between survivors and deceased.
Number of residual functional activities.
Number of errors.
Number of diseases.
MNA score: ≥24 (satisfactory nutritional status), 17–23.5 (at risk of malnutrition), <17 (malnutrition).
ESS score: 16–20 (minimum risk), 10–15 (moderate risk), 5–9 (high risk of developing pressure sores).
ADL, activities of daily living; CIRS, cumulative illness rating scale; ESS, Exton–Smith Scale; IADL, instrumental activities of daily living; MNA, mini nutritional assessment; MPI, multidimensional prognostic index; SPMSQ, short portable mental status questionnaire.
Survival analyses for NECPAL+ and MPI scores are described in Figure 1. NECPAL+ patients were more likely to die within one year, and the risk of death increased with increasing MPI severity. NECPAL+ patients had an almost threefold higher risk for one-year mortality than NECPAL− patients even after adjustments [adjusted hazard ratio (Model 1): 2.7, 95% confidence interval (CI) 1.2–6.4, p = 0.020; adjusted HR (Model 2): 2.5, 95% CI 1.0–6.0, p = 0.046], as described in Supplementary Table S6. All the NECPAL categories were associated with one-year mortality (Supplementary Fig. S1), even after adjusting for age, sex, and MPI score (adjusted model not possible for category 3 given the small number of control subjects) [adjusted HR for SQ: 2.4 (95% CI 1.0–5.6), p = 0.045; adjusted HR for category 2: 2.6 (95% CI 1.4–4.8), p = 0.002; adjusted HR for category 4: 2.4 (95% CI 1.1–5.5), p = 0.037].
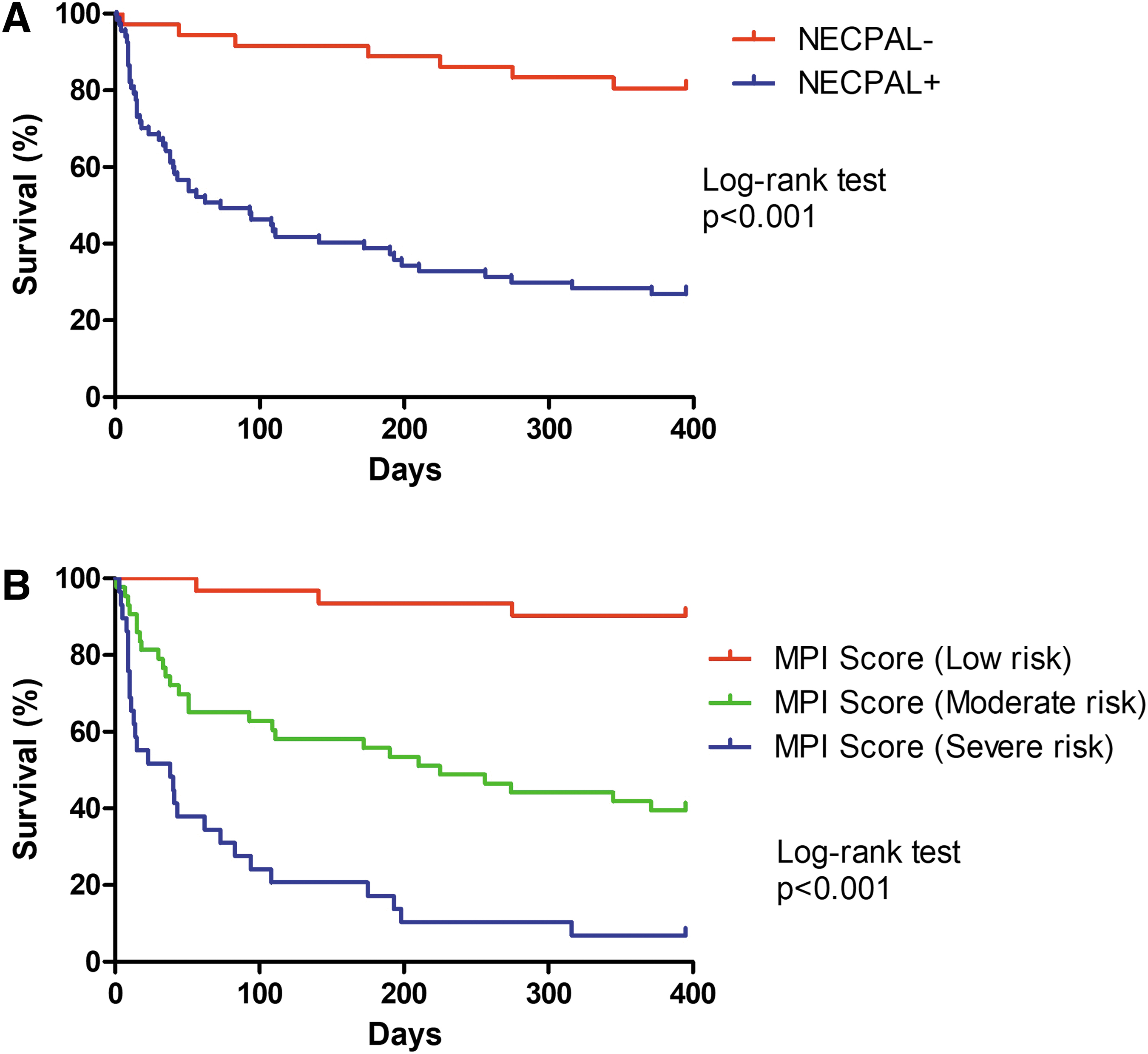
Kaplan–Meier survival curves according to NECPAL
In the comparison between ROC curves, MPI showed a better predictive power than NECPAL [area under the curve for MPI: 0.85 (95% CI 0.74–0.91) vs. AUC for NECPAL: 0.75 (95% CI 0.65–0.83), p for pairwise comparison = 0.030], as described in Figure 2. Among the NECPAL categories, SQ, categories 2 and 4 predicted mortality with no statistically significant differences, while category 3 did not predict mortality (Supplementary Fig. S2).
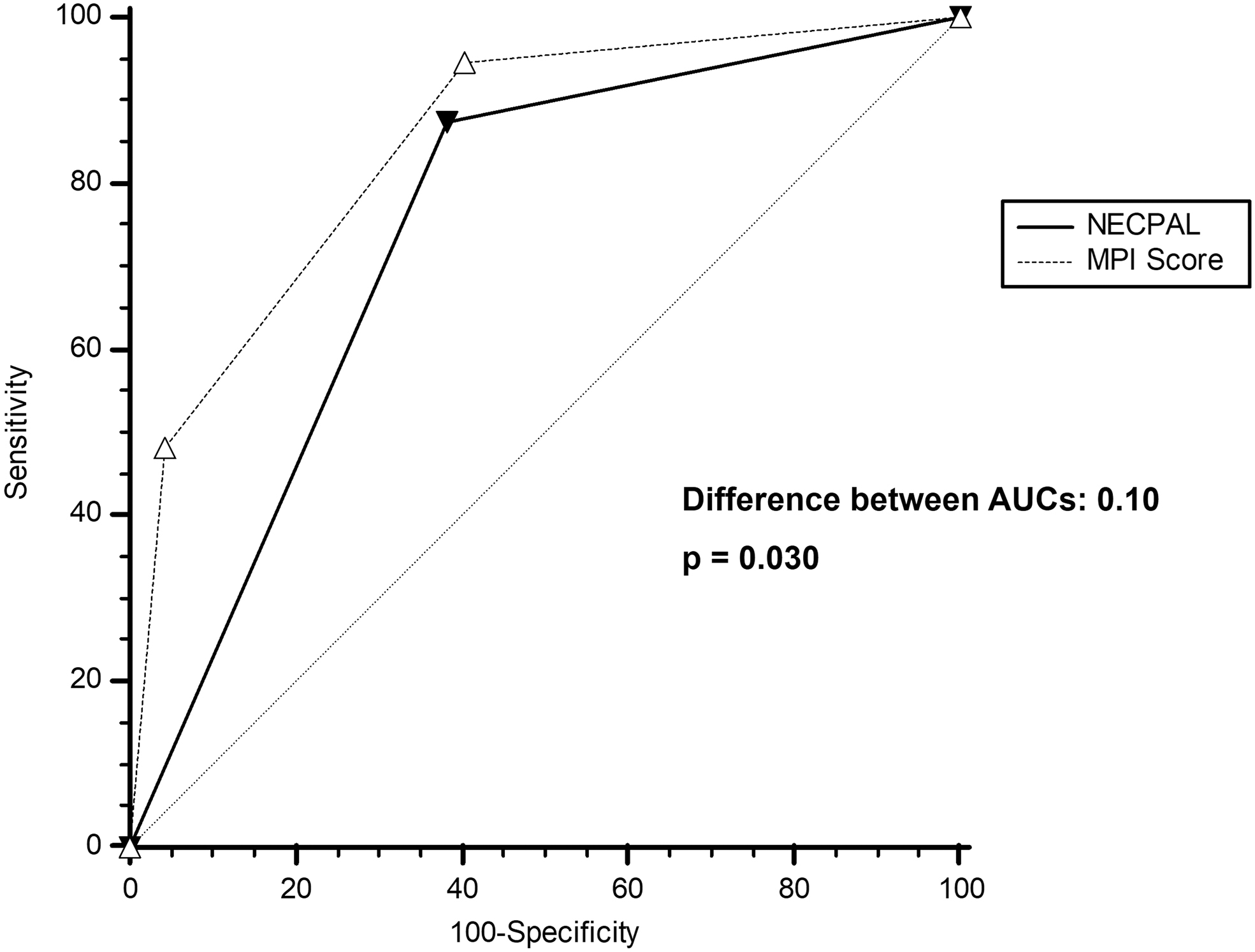
Comparison of ROC curves between NECPAL and MPI in predicting one-year mortality. AUC, area under the curve; ROC, receiver operating characteristic.
A sensitivity analysis was performed to improve the predictive power of the NECPAL tool. We evaluated the AUC of each single item of both NECPAL and MPI (Supplementary Table S7). Regarding MPI, all the items showed a statistically significant AUC, except for number of medications and social support network. Regarding NECPAL, the item “Comorbidity: ≥2 concurrent diseases” was the only one not statistically significant within the category 3, while the neurological diseases were those with the greatest predictive value within the category 4. Given that the category 3 was the only one that resulted not statistically significant (Supplementary Fig. S2) and the item “Comorbidity: ≥2 concurrent diseases” was the only one not statistically significant within the category 3 (Supplementary Table S7), we chose to remove the item “Comorbidity: ≥2 concurrent diseases” from the NECPAL. After the exclusion of this item, the prevalence of NECPAL+ patients was 62.1% (64 patients). NECPAL+ patients confirmed a higher one-year mortality compared with NECPAL− patients, as described in Supplementary Figure S3 [adjusted HR (Model 1): 3.3, 95% CI 1.4–7.8, p = 0.006; adjusted HR (Model 2): 2.7, 95% CI 1.1–6.7, p = 0.028].
In the comparison between ROC curves, no statistically significant differences emerged between “modified” NECPAL and MPI regarding predictive performance for mortality [AUC for “modified” NECPAL: 0.78 (95% CI 0.69–0.85) vs. AUC for MPI: 0.85 (95% CI 0.74–0.91), p for pairwise comparison = 0.122] (Supplementary Fig. S4).
Discussion
In our study of more than one hundred hospitalized older patients followed for one year, NECPAL allowed to identify a high prevalence of patients (more than half) who were appropriate for PC. NECPAL was also found to have a good predictive power on one-year mortality in this particular population, similar to that of a validated geriatric prognostic tool, the MPI. Patients who tested NECPAL+ during hospitalization had almost threefold higher risk of one-year mortality compared with patients who tested NECPAL−, regardless of age, sex, and MPI or its single items.
In our study, we evaluated medium/long-term mortality (one-year mortality), considering both the mean age of our patients and the multiple chronic diseases they suffered from, rather than short-term mortality (e.g., 30 days) that is characteristic of end-of-life studies. In fact, other previous studies on similar populations used the same cutoff (one year) to define long-term mortality. 17 In this context, an early identification of PC appropriateness in noncancer older frail patients is important and should look beyond the disease-centered parameters.18,19 Both of the tools taken into account in our study (NECPAL and MPI) require a comprehensive multidimensional approach and they are both labor intensive. However, the fact that NECPAL allows to establish the appropriateness of PC and to predict the prognosis at the same time in the hospitalized older patient could represent a major advantage compared with MPI in daily clinical practice. It is important to keep in mind that the evaluation of prognosis is always characterized by a certain degree of uncertainty, therefore, a single prognostic indicator suitable for all patients cannot exist. 20
This is even more true in the geriatric setting, as most of the available models do not adequately adapt to this peculiar population. 21 The MPI is a validated geriatric scale that was developed using the CGA data. Several previous studies found that MPI has excellent accuracy in estimating negative clinical events (e.g., short- and long-term mortality, hospitalization, institutionalization) in different clinical settings and in several cohorts of older adults with specific acute and chronic diseases.22–24 The NECPAL tool, as well as MPI, takes into account several aspects of the CGA, although it is not a tool specifically designed for older subjects and for prognostic purpose. However, the combination of the SQ with the other parameters of the NECPAL tool (functional and nutritional declines, multimorbidity, use of resources, and disease-specific criteria of severity and progression) was found to be potentially useful to estimate both short and long-term mortality in patients with advanced chronic diseases and appropriate for PC in previous studies, with AUCs similar to those found in our study. 9
In fact, several previous studies investigated the prognostic performance of NECPAL in different settings from ours, such as younger populations affected by chronic illness.7,9,10 Gómez-Batiste et al. explored the predictive validity of SQ and NECPAL in a cohort of 1064 subjects with advanced chronic conditions. 10 At 12-month follow-up, NECPAL showed a high sensitivity and good negative predictive value, but low specificity in terms of prognosis. The authors questioned how the definition of NECPAL+ as having only one additional parameter added to the SQ+ led to no significant differences between SQ+ population and NECPAL+ population (93% of SQ+ individuals were also NECPAL+), suggesting the need for greater selectivity in the criteria for NECPAL+, such as the use of additional indicators (e.g., frailty, geriatric syndromes, and cognitive impairment), to increase its predictive value and to differentiate it more clearly from the SQ. 10 At least in part, this criticism has also been found in our analysis on older subjects, in whom the prevalence of SQ+ patients and NECPAL+ patients was 66.0% and 65.1%, respectively. This issue is beyond the scope of our study and future ad hoc studies are needed to clarify this aspect.
While the neurological diseases were those with the greatest predictive value within the category 4 (disease-specific indicators) of the NECPAL, the category 3 was found to not significantly predict one-year mortality in our study. Therefore, we chose to remove the item “Comorbidity: ≥2 concurrent diseases” of the category 3 from the NECPAL, as a result of statistical observations, given its lack of statistical significance. This was likely due to the very high prevalence of multiple (two or more) comorbidities typically found in our older subjects (94.2% of patients had two or more concurrent comorbidities) that could have overestimated the prevalence of NECPAL+ patient. After removing this item, the accuracy of the NECPAL has improved in our scenario. However, this hypothesis should be tested and validated in further larger studies on geriatric populations.
In our study, >60% of older hospitalized patients admitted for acute medical and surgical conditions resulted in NECPAL+ and thus potentially appropriate for a PC approach. A recent study on 590 acute geriatric subjects (mean age: 86.4 ± 5.6 years) with cognitive decline and/or approaching the end of life found a lower prevalence of NECPAL+ patients (44.1%) than our study. The authors found a direct association between the degree of frailty, evaluated by Frail-VIG index (Valoración Integral Geriátrica—CGA), and the prevalence of NECPAL+ patients, similarly to what was observed in our study using MPI. Moreover, the degree of frailty correlated with survival after a 2-year follow-up. 25
It would be appropriate to start a PC approach whenever patients suffering from progressive degenerative diseases (oncological and nononcological) test positive to NECPAL. The patient management should be based on the complexity of the individual condition.14,26 In this perspective, our study highlights the high prevalence of older hospitalized patients for whom starting a PC approach would be appropriate. To do this, basic PC skills should be acquired by all geriatricians and integrated into routine clinical practice, while at the same time close collaborations with PC experts should be built. The PC approach is based on some fundamental elements: quality of life as the main objective, care centered on the patient and his family and not centered on the disease, a great attention to the assessment and control of symptoms that cause distress (i.e., pain, dyspnea), a clear communication with respect to the prognosis for a shared planning of care. 27 Regarding this last aspect, the fact that NECPAL has also a prognostic role in the older hospitalized population may represent a key issue in clinical practice.
The comprehensiveness of the NECPAL enables early PC intervention, multidimensional assessment, advanced care planning, and case management. If an old conception considered the transition from active care to PC as a clear step, over time, scientific consensus is favoring a progressive introduction of PC as an integrated response (the so-called “simultaneous PC”) dedicated to the majority of older patients with advanced chronic diseases. However, the early identification often still remains a challenge in daily clinical practice.28–31
The PC in hospitalized older patients appears as a priority, given the high prevalence of patients that would be appropriate for a PC approach and the prognostic implications found in our study. However, specific literature on this topic is still scarce. Therefore, major challenges in this area include establishing high-quality, ethically sound research projects on older population, facilitating health care decision making on the different phases of the care trajectories.
Study limits
The strength of our study is the accurate training of the investigators and the standardization of data collection, to reduce systematic errors. However, the study has some limitations. The peculiar study population (oldest patients in acute hospital setting) may not allow a generalization of our findings to other populations with different characteristics. Laboratory parameters were not collected in this study. However, the population has been well characterized, thanks to the collection of data needed for compiling both the NECPAL and MPI. The main causes of death were not easy to be determined in our older population, in whom comorbidities and advanced chronic diseases were often present. Moreover, the enrollment of the patients took place on June 24, 2019 and the SARS-CoV-2 pandemic spread during the one-year follow-up. Therefore, a possible influence of the pandemic on our findings cannot be excluded. Finally, although the statistical power of NECPAL in predicting mortality in the survival analysis was >90%, the statistical power of our study with this sample size for comparing the AUC between the two tools (NECPAL and MPI) was <80%.
Conclusion
Previous studies on younger populations found that NECPAL was useful to define the appropriateness of PC, also having a good prognostic performance. In our study, we tested both the performance of the NECPAL tool on identifying the appropriateness of PC and its predictive value on one-year mortality in older hospitalized patients. Then, we compared the NECPAL with another tool validated in older populations, the MPI, finding that they performed comparably. NECPAL is adequate both for establishing the appropriateness of PC and for predicting one-year mortality in hospitalized older patients. This tool could help clinicians detecting those patients in whom PC should be integrated with active care simultaneously, with the aim of a global response to the needs of the patients suffering from multiple chronic diseases and their families, through an individual care planning. We, therefore, conclude that if you are using NECPAL, you can be comfortable extending it to older hospitalized patients for whom, unless CGA tools are readily available, NECPAL may be less labor intensive than MPI for documenting one-year mortality risk.
Further studies are needed to investigate the clinical usefulness of NECPAL in terms of decision making, impact on the patient care, and cost-effectiveness in older patients.
Footnotes
Acknowledgments
The authors thank the “Fondazione Floriani” and the “Fondazione G. Berlucchi” for the authorization to use the NECPAL CCOMS-ICO©.
Authors' Contributions
F.S.: Conceptualization, data curation, formal analysis, investigation, methodology, software, validation, visualization, writing–original draft, and writing–review and editing. S.F.: Data curation, investigation, resources, and writing–original draft. F.G.: Data curation, validation, visualization, writing–original draft, and writing–review and editing. S.S.: Data curation, and investigation. V.M., P.T., P.G., L.M., and L.F.: Data curation, investigation, and resources. M.C.: Supervision, validation, and writing–review and editing. R.S.: Resources, supervision, validation, and writing–review and editing. M.R.L.: Conceptualization, data curation, investigation, methodology, project administration, resources, validation, writing–original draft, and writing–review and editing. All authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Data Statement
The data that support the findings of this study are available from the corresponding author (F.S.) upon reasonable request.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
The authors declare no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.