
Abstract
Background:
Given the complex care needs of older adults receiving home health care (HHC), it is important for HHC clinicians to identify those with limited prognosis who may benefit from a transition to hospice care.
Objectives:
To assess the association between HHC clinician-identified likelihood of death and (1) 1-year mortality, and (2) hospice use.
Methods:
Prospective cohort study from the National Health and Aging Trends Study (NHATS) waves 2011–2018, linked to the Outcomes and Assessment Information Set (OASIS) HHC assessment and Medicare data among 915 community-dwelling NHATS respondents. HHC clinician—identified likelihood of death/decline was determined using OASIS item M1034. Multivariable logistic regression was used to assess the association between clinician-identified likelihood of death/decline and 1-year mortality and hospice use.
Results:
HHC clinicians identified 42% of the sample as at increased risk of decline or death. One year mortality was 22.3% (n = 548), and 15.88% (n = 303) used hospice within 12 months of HHC. HHC clinician-perceived likelihood of death/decline was associated with greater odds of 1-year mortality (odds ratio [OR], 6.57; confidence interval (95% CI), 2.56–16.90) and was associated with greater likelihood of hospice use (OR, 1.61; 95% CI, 1.00–2.62).
Conclusion:
HHC clinician perception of patients' risk of death or decline is associated with 1-year mortality. A better understanding of HHC patients at high risk for mortality can facilitate improved care planning and identification of homebound older adults who may benefit from hospice.
Key Message
Home health care (HHC) clinician perception of likelihood of death was associated with increased mortality among a nationally representative sample of HHC patients. Our findings illustrate the potential clinical utility of Outcomes and Assessment Information Set question; M1034 to prompt clinicians to initiate goals-of-care discussions with patients with serious illness.
Introduction
A
Indeed, data show that even short hospice stays are associated with fewer burdensome transitions at the end of life (e.g., hospitalizations and intensive care unit admissions) in the general Medicare population. 7 Prior work in nursing home settings has shown that clinicians' ability to recognize terminal decline significantly influences hospice referral timing. 9 The surprise question, “Would you be surprised if this patient dies in the next 12-months?” is widely used to alert clinicians in the nursing home and hospital setting to identify patients who might benefit from referral to programs such as hospice or from discussion about end-of-life care needs and preferences.10,11
In HHC settings, clinicians (registered nurses [RN] and therapists [physical therapist, occupational therapist, or speech language pathologist) conduct patients' assessments using the federally mandated Outcomes and Assessment Information Set (OASIS) instrument. 12 Until 2019, OASIS contained a version of the surprise question—item M1034 which prompted the HHC clinician to document if, “the patient has serious progressive conditions that could lead to death within a year,” based on the clinician's subjective risk assessment. To determine whether HHC clinician's perception of likelihood of death was predictive of patient outcomes, we examined the association of HHC clinician-perceived likelihood of death based on the OASIS item (M1034 Patient Overall Status) and (1) 1-year mortality, and (2) hospice use. This information, if used effectively, could guide HHC care planning and future development of OASIS items that better support HHC clinician decision making for patients with serious illnesses.
Methods
Study sample and data sources
Data for this study were drawn from OASIS, National Health and Aging Trends Study (NHATS), and Medicare claims. OASIS is the nationally mandated patient assessment completed by HHC clinicians (RN or physical therapist) for adult patients who receive HHC services covered by Medicare or Medicaid. OASIS contains data regarding patients' sociodemographic status, environment, health status, functional status, plan of care, and caregiver availability.13,14 Conducted since 2011, NHATS is a longitudinal nationally representative survey of Medicare beneficiaries 65 years of age and older in the United States, over sampling older ages and Black beneficiaries. 15 Linked Medicare claims are available for all Medicare recipients. The Johns Hopkins University Institutional Review Board approved the NHATS protocol, and all participants provided written informed consent. The Icahn School of Medicine at Mount Sinai's Institutional Review Board approved this study.
Study population
To construct this data set, we linked NHATS annual assessment data for the years 2011 to 2018 (N = 12,427 respondents, 53,325 observations) to OASIS for the years 2011 to 2018 (N = 5239 patients; 22,435 observations). First, we dropped those who did not complete the sample person interview (N = 329 patients, 1085 observations). We limited individuals to those whose first OASIS clinical assessment was within 3 months of the NHATS survey interview to ensure that survey collected variables were contemporaneous with the clinical assessment (N = 2425 patients, 3435 observations). Because one NHATS participant can have multiple OASIS assessments, only the first HHC start of care assessment was included (N = 2202 patients, 3108 observations). The final sample included 2202 community dwelling NHATS participants with OASIS assessments and only the last qualifying interview was included.
Measures
The primary outcome of interest was 1-year mortality (time from NHATS survey to death, censored at 365 days). Date of death was obtained from the Master Beneficiary Summary File and from NHATS. As a secondary outcome, we assessed whether participants received hospice (yes/no) within a year following the SOC OASIS assessment, using CMS hospice billing data.
Predictor
The predictor of interest was a version of the surprise question identified by OASIS item M1034 (overall patient status), which asks “Which description best fits the patient's overall status?” M1034 group's overall status of HHC patients into four categories: 0 = stable with no heightened risks for serious complications or death, 1 = temporarily facing high health risks but is likely to return to being stable without heightened risks for serious complications and death, 2 = likely to remain in fragile health and have ongoing high risks of serious complications and death, and 3 = serious progressive conditions that could lead to death within a year. To examine clinician perceived likelihood of decline leading to death within a year, we combined “0” and “1” (i.e., clinician perception that death is not likely in the next year) to create a three-category measure of perceived likelihood of death.
Other variables
Covariates were obtained from the NHATS survey unless otherwise noted. Sociodemographic and caregiving characteristics included age (65–69, 70–74, 75–79, 80–84, 85–89, and ≥90 years), sex (male/female), race/ethnicity, educational attainment (high school education or greater), Medicaid status, living arrangement (living alone), marital status (married/living with partner), presence of a paid caregiver, and number of unpaid caregiver hours per week (<6, 6–19.9, 20–39.9, and ≥40). 16 Functional characteristics included level of Activity of daily living (ADL) dependency (defined as receiving help with none vs. one to two ADLs, three or more ADLs) and Instrumental ADL (IADL) dependency defined similarly (receives help with none vs. one to two IADLs, three or more IADLs), using the five IADLs: laundry, driving, shopping, meal preparation, and managing finances, and ADLs: eating, bathing, toileting, dressing, getting out of bed, getting around inside, and getting around outside.
Clinical characteristics included self-reported health (e.g., cancer and depression), dementia status was determined based on previously defined and validated NHATS algorithm. 15 We used Medicare claims to calculate the Charlson Comorbidity Index based on ICD-9/10 codes in claims. 17 We used the OASIS item M1000 to determine if a patient had a prior inpatient stay within 14 days of HHC admission (hospital or nursing home) or whether they were community-entrants.
Statistical analysis
We first performed univariate analyses to summarize baseline demographics, comorbidities, caregiving status, and other health-related predictors. Weighted percentages were reported for categorical variables; mean and standard deviation were reported for continuous variables. Multivariable logistic regression models were used to examine the relationship between HHC clinician-assessed risk of death/decline within a year and the following: (1) 1-year mortality and; (2) transition to hospice within 12 months. All analyses used survey weights to account for differential nonresponse and the complex sampling design. 18 All analyses were performed using Stata, version 16 (College Station, TX).
Results
The study sample included 2202 community-dwelling individuals. Table 1 describes characteristics of the population. Most notably, 37.86% were 75–84 years old and 33.30% were 85 years or older. The sample was mostly female (63.36%) and White (75.45%). Of participants, 35.68% were married or living with a partner, while many lived alone (41.73%). Of participants, 25.61% were enrolled in Medicaid, and 58.24% reported no more than a high school education. Most participants had substantial health issues, 49.48% reported fair or poor overall health, 34.76% had cancer, 28.93% were identified with probable dementia, 28.90% had depression. Less than one-quarter (23.95%) of the sample reported receiving help from a paid caregiver. A larger share of participants was admitted to home health following an acute care hospital stay in the last 14 days (43.50%), followed by participants admitted to HHC directly from the community, without an inpatient stay in the last 14 days (36.39%).
Sample Characteristics (N = 2202)
Discharge statuses during the past 14 days are not mutually exclusive.
Only assessment 2017 and prior was included.
ADL, activity of daily living; IADL, Instrumental ADL; NHATS, National Health and Aging Trends Study; SD, standard deviation.
In the overall cohort, 1-year mortality was 22.30% (n = 548). As shown in Figure 1, HHC patients had distinct trajectories based on HHC clinician's response to the M1034 “surprise” question.
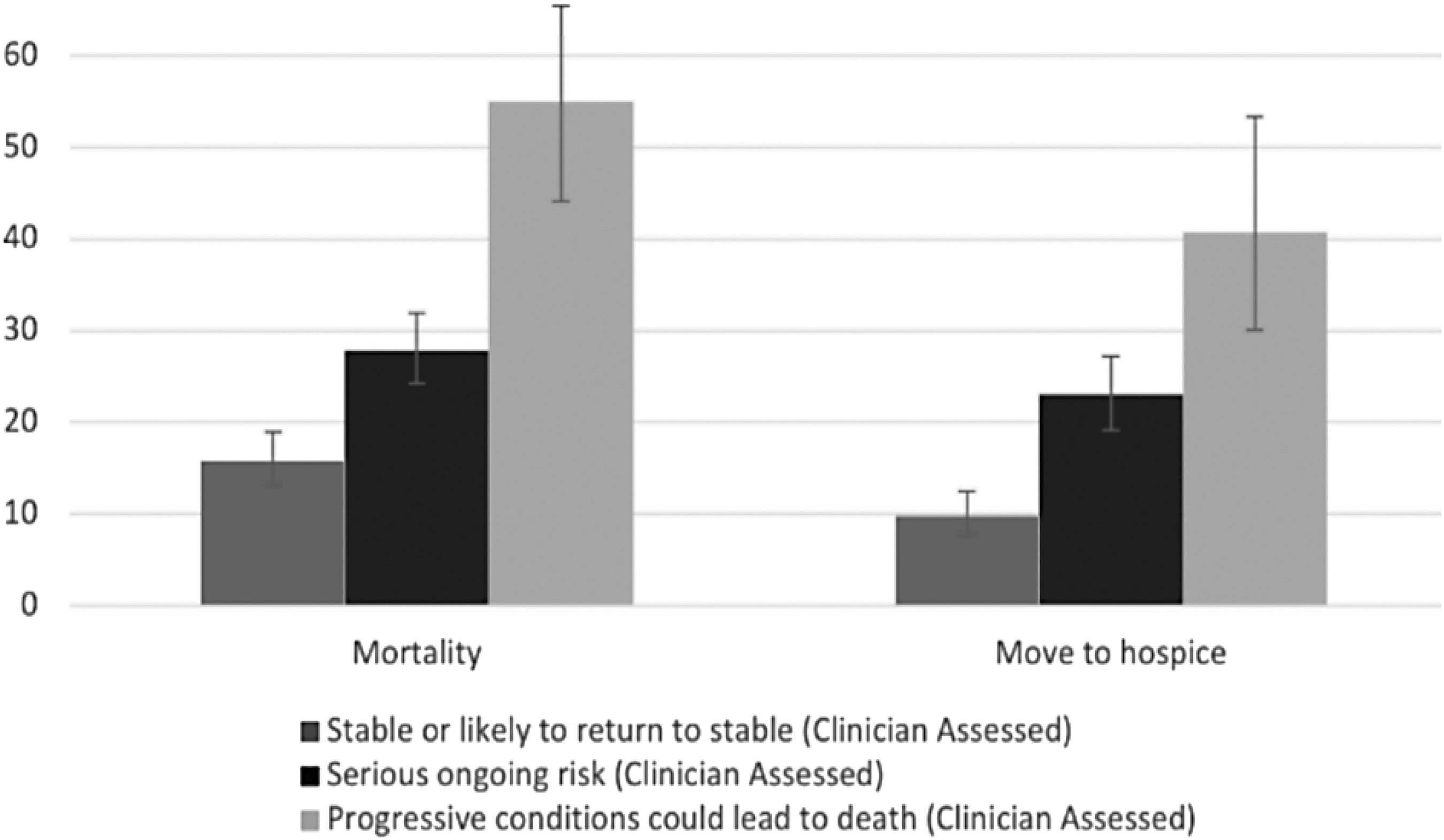
Association between HHC-clinician assessment of risk of death/decline and risk of mortality and hospice in the next year. HHC, home health care.
Association between HHC clinician-perceived likelihood of death/decline and 1-year mortality
Table 2 presents the association between HHC clinician-perceived likelihood of death/decline and 1-year mortality. Clinician assessed likelihood of ongoing high risk of serious complications and death was associated with hospice use (odds ratio [OR], 1.88; confidence interval [95% CI], 1.23–2.87). HHC-clinician identified likelihood of death/decline within a year was strongly associated with greater odds of 1-year mortality (OR, 6.57; 95% CI, 2.56–16.90) in adjusted models that accounted for a range of sociodemographic and clinical characteristics. The multivariable logistic regression model identified several additional patient characteristics that were significantly associated with 1-year mortality. The oldest age group had a 2.58 times greater odds of mortality (≥85 years, OR, 2.58; 95% CI, 1.49–4.46), compared with those aged 65 through 74 years.
Logistic Regression on Home Health Care Clinician-Perceived Likelihood of Death/Decline and 1-Year Mortality
Unadjusted OR (95% CI) of clinician-assessed likelihood of death within a year = 2.12 [1.52–2.95].
CI, confidence interval; OR, odds ratio.
Association between HHC clinician-perceived likelihood of death/decline and hospice use
Table 3 presents the association between HHC clinician-perceived likelihood of death/decline and Hospice Use. Clinician assessed likelihood of ongoing high risk of serious complications and death was associated with hospice use (OR, 1.93; 95% CI, 1.07–3.48). HHC-clinician identified likelihood of death/decline within a year was strongly associated with greater likelihood of hospice use (OR, 4.99; 95% CI, 1.80–13.87) in adjusted models that accounted for a range of sociodemographic and clinical characteristics. The multivariable logistic regression model identified several additional patient characteristics that were significantly associated with hospice use.
Logistic Regression on Relationship Between Home Health Care clinician-Perceived Likelihood of Death/Decline and Move to Hospice in a Year
Unadjusted OR (95% CI) of clinician-assessed likelihood of death within a year = 2.32 [1.50–3.61].
Patient characteristics independently associated with hospice use included older age (≥85 years, OR, 3.52; 95% CI, 1.60–7.75), receiving help with three or more ADLs (OR, 2.21; 95% CI, 1.15–4.26), and more medical conditions (OR, 1.25; 95% CI, 1.10–1.42). We found that those who self-reported fair or poor health were more likely to enroll in hospice than those who did not (OR 1.94; 95% CI, 1.11–3.40). Those discharged from nursing homes within the past 14 days were less likely to enroll in hospice care (OR, 0.24, 95% CI, 0.10–0.60).
Discussion
In this nationally representative, prospective cohort study, HHC clinician perception that death in the next year was likely was independently associated with 1-year mortality and hospice use among community dwelling older adults who received HHC. Previous work in the HHC population has been limited to predictors of mortality among HHC patients with specific diagnoses, including heart failure, postacute care patients with sepsis or COVID-19.19–21 Our study adds to the limited existing literature examining clinician perceptions of patient likelihood of death in the next year using OASIS, and confirms that this question may have clinical utility as a means to help HHC clinicians to identify patients who may benefit from hospice care referral. 22
Our models account for age, comorbidities, caregiver availability, and measures of functional status in examining the association between clinician-perceived likelihood of death in the next year and mortality. This affirms that above and beyond other information obtained as part of a HHC clinical assessments, the question (OASIS item: M1034) is a clinically promising approach to improve the quality-of-care planning for HHC patients with serious illness and potentially improve transitions to hospice care among this vulnerable group of older adults.
Of note, we also found that clinician-perceived likelihood of death was associated with hospice use. One may argue that this finding, in part, points to potential barriers to transition to hospice not captured in patients' acuity in HHC and further underscores a need for future research to better understand clinician—decision-making processes or care planning related to transitions from HHC to hospice. In particular, the finding that Black patients had lower likelihood of transition to hospice is not surprising, and consistent with well-documented racial disparities in hospice and end-of-life care in the United States.3,23–26
Reasons for these disparities are multifaceted and include the dearth of culturally tailored information about the benefits of hospice in minority communities. 23 The integration of standardized OASIS items, such as the M1034 is necessary, and presents a promising opportunity to advance equitable transitions from HHC to hospice care. By incorporating objective and evidence-based criteria in the OASIS, HHC clinicians (nurses and therapists) are empowered to effectively identify patients who may benefit from earlier referrals to hospice.
These findings have important implications for policymakers and HHC clinicians. OASIS item M1034: “Overall status” was eliminated in the OASIS-D release in January 2019, and no similar item exists to prompt clinicians to develop care plans tailored to the needs of patient who may be nearing the end-of-life period within the current version of OASIS. Reconsidering this change and reincorporating this question may provide an opportunity to improve the OASIS tool and support clinician decision making that facilitates a pathway to hospice for appropriate patients. Recent qualitative data show that HHC clinicians are willing to have serious illness discussions and develop care plans that address patient's end-of-life care needs. 5 The HHC setting provides an opportunity to engage patients with serious illness and their families in discussions about hospice to facilitate transitions to hospice.
However, HHC nurses, who are the primary clinicians in the HHC setting responsible for care coordination and referrals, have emphasized a need for a risk assessment tool that prompts the identification of patients who may be appropriate for hospice care. 6 While examining referral sources for hospice referrals was outside the scope of this study, we recognize that a hospice referral can be made from a variety of sources (e.g., hospital discharge planner or primary care provider) that may or may not be connected to HHC providers. To better understand how HHC clinicians may impact hospice referral, future work should examine referral sources for HHC patients who are discharged directly to hospice.
This study was strengthened by using a nationally representative sample of the U.S. older adult population. Still, several limitations must be mentioned. Our study population was limited to older Medicare recipients, and the findings may not apply to other patient populations. In addition, we were unable to report the distinct profile of each response to the M1034 because of cell size restrictions in the data use agreement. While we were able to identify factors associated with hospice use, we did not have data on patients' end-of-life preference, which is crucial to better understand drivers of hospice enrollment.
Conclusion
In summary, we found that HHC clinician-assessed risk of death was associated with 1-year mortality, and increased hospice use. Our findings illustrate the potential clinical utility of this question in OASIS to prompt clinicians to consider hospice care. Future work should further investigate the development and implementation of more OASIS-based clinician-decision support tools to guide end-of-life care planning in HHC.
Funding Information
The study is supported by the National Institute on Aging (P01 AG066605 and P30AG028741). Z.T.O. was supported by a grant from the National Institute on Aging (5P30AG028741-07) awarded to the Claude D. Pepper Older Americans Independence Center at the Icahn School of Medicine at Mount Sinai.
Author Disclosure Statement
No competing financial interests exist.