
Abstract
Background:
The modified Rankin Scale (mRS), which measures degree of disability in daily activities, is the most common outcome measure in stroke research. Quality of life (QoL), however, is impacted by factors other than disability. The goal of this study was to assess the correlation between functional dependence and a more patient-centered QoL measure, the European QoL visual analog scale (EQ VAS).
Methods:
We reviewed prehospital and hospital records from 11 acute care hospitals in Seattle, Washington (USA) from June 2000 to January 2003 for this cohort study. Patients with a final diagnosis of stroke were contacted three to four months after stroke, and mRS and EQ VAS were assessed. Good QoL was defined as EQ VAS ≥65.
Results:
Of 760 patients with stroke, 346 were available at three to four months. Most (296, 85.5%) had ischemic stroke. Overall, mRS and QoL were negatively correlated (Spearman's ρ −0.53, p < 0.001). Percentage of good QoL decreased as mRS increased from 0 to 5 (88%, 70%, 52%, 50%, 31%, 20%, respectively, p < 0.001). However, 36% (n = 62) of patients with dependent mRS (3–5, n = 174) reported good QoL, and 30% (n = 52) of patients with independent mRS (0–2, n = 172) reported poor QoL. In multivariable analysis, older age, male gender, and absence of dementia, were associated with good QoL despite dependent mRS; atrial fibrillation was associated with poor QoL despite independent mRS.
Conclusions:
QoL decreases with increasing mRS, but exceptions exist with good QoL despite high mRS. To provide patient-centered care, clinicians and researchers should avoid equating disability with QoL after stroke.
Introduction
Treatment decisions after stroke rely heavily on what clinicians, patients, and families understand possible outcomes to be. Outcomes are commonly measured by the degree of disability. The modified Rankin Scale (mRS) score (Supplementary Table S1) quantifies disability on a 7-point scale ranging from 0 (no symptoms) to 6 (dead) and has become a standard clinical outcome measure when evaluating the effectiveness of stroke-related treatments (Supplementary Table S1). The mRS is often dichotomized into good versus poor outcome, although no consensus exists on where to draw the line. 1 To add granularity to the mRS, the Barthel Index (BI) is frequently used as an adjunctive outcome measure in stroke research (Supplementary Table S2). This scale rates the patient's level of independence in performing 10 basic activities of daily living: feeding, bathing, grooming, dressing, bowel control, bladder control, toileting, transfers, walking on level surfaces, and climbing stairs.
Quality of life (QoL) is likely affected by circumstances other than level of disability, including social, psychological, and financial factors. One of the most used metrics of health-related QoL is the self-reported European QoL (EQ) scale, which includes two parts. 2 The first part is the EQ-5D descriptive classifier, which asks patients to rate their level of difficulty on five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The second part is the visual analog scale (EQ VAS), which asks patients to rate their overall health from 0 to 100, in which 0 is the worst and 100 the best imaginable health state. The EQ VAS rating scale may provide a more holistic representation of QoL not captured by the specific dimensions assessed using the EQ-5D, particularly given the EQ-5D's emphasis on level of function and physical disability. 3 As with the mRS, no consensus exists as to where to draw the line between “good” and “poor” outcome in the EQ VAS.
The goal of this study was to assess the correlation between disability or functional dependence as represented by the mRS and QoL as represented by the EQ VAS. If functional dependence correlates highly with QoL after stroke, then QoL outcome predictions can continue to rely on predictions of dependence.
Methods
We reviewed prehospital and hospital records from 11 acute care hospitals in the Seattle area from June 2000 to January 2003 and identified all subjects with a final hospital diagnosis of stroke, but not transient ischemic attack (TIA). Data collected from the medical record included demographic information, comorbid diseases, stroke symptoms, and stroke severity on admission. Stroke severity was quantified using the validated retrospective NIH stroke scale (rNIHSS). 4 All subjects were initially contacted by telephone for a three- to four-month follow-up assessment with the patient or a surrogate respondent. During this call, we explored patients' sociodemographic factors and their outcomes with the mRS, BI, and EQ VAS.
We dichotomized mRS into independent (0–2) and dependent (3–5). 5 We dichotomized QoL at the median EQ VAS and defined good QoL as an EQ VAS greater than or equal to the median and poor QoL as an EQ VAS below the median. We made this choice a priori so that we would have groups of equal size to optimize the power of comparisons and with the understanding that the definition of good QoL is somewhat arbitrary.
This study was approved by the Human Subjects Research Committee of the University of Washington and a similar committee at each of the 11 Seattle acute care hospitals.
Statistical approach
Within the two mRS subgroups, independent or dependent, we compared demographic, baseline, and comorbid clinical variables among patients with good versus poor QoL using nonparametric statistics, including chi-square for categorical variables and Wilcoxon Rank Sum for continuous variables. Demographics included age, sex, race, insurance, level of education, and residence. The baseline variable was rNIHSS. Comorbid variables included history of stroke, TIA, hypertension, diabetes, atrial fibrillation (AF), myocardial infarction, cigarette use, hyperlipidemia, and dementia. Multivariable logistic regression with dichotomized QoL as the outcome variable proceeded in a three-step process separately for those independent (mRS 0–2, with poor QoL as the outcome of interest) and dependent (mRS 3–5, with good QoL as the outcome).
First, demographic and baseline variables with p < 0.10 in univariate analyses were added to the multivariable model and manually removed in a stepwise fashion if p > 0.05, starting with the highest p-value first. Second, comorbid conditions were added to the multivariable model and removed in the same process. Third, individual items from the BI (coded as an ordinal variable with scores from 0 to 3 depending on the individual Barthel item; Supplementary Table S2) were added and removed in the same way. The variables mRS, age, sex, and second step significant comorbid conditions were retained in all models. Statistical significance was set at the traditional 0.05 level. Statistics were performed using STATA (version 16, College Station, TX).
Results
We identified 760 patients admitted to the hospital with stroke. Of those, 228 (30%) died before the three-month call, and 186 (24%) were lost to follow-up. Among the remaining 346 stroke patients, the most common diagnosis was ischemic stroke in 296 patients (85.6%), followed by intraparenchymal hemorrhage (n = 40; 11.6%), and subarachnoid hemorrhage (n = 10; 2.9%). Our population was elderly (mean age 76 years, standard deviation (SD = 1), and predominantly Caucasian (70%) and female (58%).
At the three-month follow-up, most patients were living at home (n = 248, 72%), 66 patients (19%) were in a skilled nursing facility, 9 patients (3%) were in inpatient rehabilitation, and 23 patients (6%) resided in other situations. Half of patients (n = 172, 50%) were independent (mRS 0–2). A majority (n = 205, 59%) were able to answer the questionnaires independently, leaving surrogates (n = 141, 41%) to answer questions on the patients' behalf in the rest. The median value on the EQ VAS was 65 and the mean value on the EQ VAS was 61.5 (SD = 23.7). Overall, mRS and EQ VAS were negatively correlated (Spearman's ρ −0.53, p < 0.001, Fig. 1). The percentage of a good QoL decreased as the mRS increased from 0 to 5 (87.8%, 70.4%, 51.9%, 50%, 31.3%, 20.4%, respectively, p < 0.001). Still, 62/174 (36%) of dependent patients (mRS 3–5) had good QoL and 52/172 (30%) of independent patients (mRS 0–2) had poor QoL.
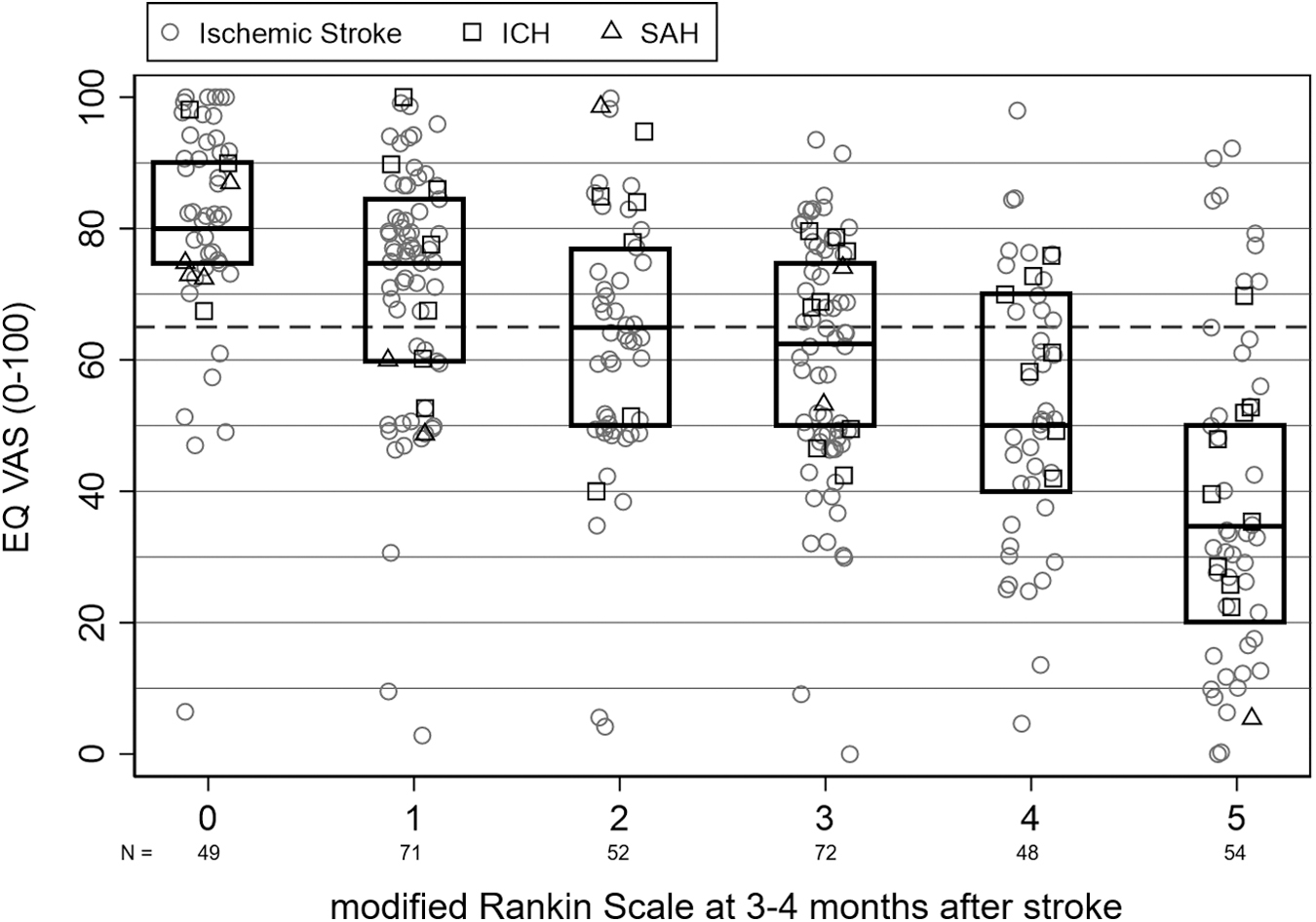
EQ VAS versus mRS at three to four months poststroke. Dotted line represents break point of 65 for good versus poor QoL. Spearman's ρ −0.54, p < 0.0005. EQ VAS, European QoL visual analog scale; ICH, intracerebral hemorrhage; QoL, quality of life; SAH, subarachnoid hemorrhage.
Good QoL despite dependent mRS
For dependent patients (mRS 3–5; n = 174), QoL decreased with increasing mRS (Spearman's ρ −0.38, p < 0.0001). In univariate associations, a good QoL (EQ VAS >65, n = 62) was more common in men, in patients who self-reported QoL (vs. surrogate reporting), were living at home, had lower baseline rNIHSS, and did not have dementia (Table 1).
Patient Characteristics By Modified Rankin Scale and European Quality-of-Life Visual Analog Scale
“Good” QoL defined as EQ VAS ≥65; “poor” QoL defined as EQ VAS <65 (65 was the median reported QoL in this cohort). Bold: p ≤ 0.05 using Chi-square for categorical variables and Wilcoxon Rank Sum for continuous variables.
EQ VAS, European QoL visual analog scale; HS, high school; IQR, interquartile range; mRS, modified Rankin Scale; NIHSS, NIH stroke scale; QoL, quality of life; SD, standard deviation; TIA, transient ischemic attack.
In the first two steps of multivariable analyses, mRS, older age, male sex, and absence of dementia remained independently associated with a report of a good QoL in these dependent patients. In the third step, all 10 individual items of the BI were associated with good QoL in the univariate analyses, and so were added into the multivariable model. After stepwise removal of nonsignificant Barthel items, three Barthel items (improved functional status with feeding, mobility on a level surface, and bowel control) were independently associated with good QoL adjusted for mRS, age, gender, and dementia; age and sex also remained independently associated with good QoL (Table 2).
Multivariable Analysis of Quality of Life Performed Separately for Dependent (Modified Rankin Scale 3–5) and Independent (Modified Rankin Scale 0–2) Patients
All models included age, sex, and mRS, regardless of p-value. Final models are shown here with bold indicating p ≤ 0.05.
For analyses, we defined “Good” QoL as EQ VAS ≥65 and “poor” QoL as EQ VAS <65 (65 was the median reported QoL in this cohort).
CI, confidence interval; OR, odds ratio.
Poor QoL despite independent mRS
For independent patients (mRS 0–2; n = 172), QoL again decreased with increasing mRS (Spearman's ρ −0.37, p < 0.0001). In univariate analyses, poor QoL (EQ VAS <65, n = 52) was more common among patients with medical comorbidities, such as diabetes or AF (Table 1). In the first two steps of multivariable models, only AF remained independently associated with poor QoL adjusted for mRS, age, and sex with an odds ratio of 4 (p = 0.03). In the third step, all items of the BI except independence with feeding (p > 0.1 for association with poor QoL in univariate analysis) were added to the multivariable model. After stepwise removal of nonsignificant Barthel items, two Barthel items (less functionality with mobility on level surfaces and with dressing) were independently associated with poor QoL; mRS and AF also remained independently associated with poor QoL (Table 2).
Discussion
Our population median EQ VAS (65, where we dichotomized good vs. poor QoL) was considerably lower than the general U.S. population median of 85, 6 which may reflect the debilitating impact of stroke on QoL. Exceptions exist with our work showing that 36% of patients with dependence (mRS 3–5) had good QoL, and 30% of independent patients (mRS 0–2) had poor QoL.
Our observations need to be considered when counseling families about prognosis: some stroke survivors with dependence (mRS 3–5) can enjoy a good QoL. Among stroke survivors with mRS 3–5, we found that better functional status on three items in the BI at three to four months after stroke were significantly associated with good QoL in adjusted multivariable models: feeding, mobility on a level surface, and bowel control. While taking into account that associations do not necessarily mean causality, these findings may highlight areas for concentrated therapy efforts and assistive tools that may lead to the greatest gains in poststroke QoL, as well as key functional domains to consider when communicating prognosis after stroke.
We also found that older age, male sex, and possibly the absence of dementia were independently associated with higher QoL among disabled survivors. The association of age with QoL has been previously reported, although the direction of that correlation (direct or inverse) is equivocal and reasons for this association only hypothetical. For example, older stroke patients have been postulated to have poor QoL due to having fewer social contacts or due to a higher risk of being institutionalized. 7 However, younger stroke patients have also been postulated to have poor QoL due to higher expectations of health 8 and difficulty performing tasks such as work and child care, which are more relevant in younger populations. 9
Even among survivors who are independent (mRS 0–2), a small group reported poor QoL. In this population, only comorbid AF was independently associated with poor QoL, although it is likely that other, unmeasured factors unrelated to stroke or cardiovascular disease may have played a role. Patients with AF do report poorer QoL compared with healthy controls, and their ratings improve with rate or rhythm control strategies. 10 The impact of AF on QoL in stroke patients specifically has not been extensively investigated. Contrary to our findings, one recent study found a weakly positive association between AF and QoL after stroke, which they hypothesized may have been due to patient relief upon receiving a diagnosis of a treatable cause for their stroke. 11
Limitations of our study include that nearly half of patients initially recruited passed away or were lost to follow-up, which may introduce a selection bias toward respondents with better functional status and higher QoL. Second, follow-up QoL rating was only assessed at three- to four-month follow-up, which limits our ability to draw longer-term conclusions. Third, in those stroke survivors without dependence (mRS 0–2), the QoL before the stroke was unknown. Fourth, we used the median EQ VAS as a cutoff between good and poor QoL, which suggests that one half of the study population is considered to have a poor QoL. The true cutoff is unknown and may not exist. Fifth, the inclusion of surrogate responses in our results may have led to different QoL ratings than if only patient responses were included, as surrogates tend to rate QoL lower than patients do. 12 In stroke survivors with aphasia for example, proxies report lower QoL even when physical function is comparable. 13
Greater differences between patient and family caregiver ratings may exist in more subjective domains like mood and thinking, as compared with more objective domains like physical function. 14 This observation is particularly relevant when studying a subjective aggregate measure such as the EQ VAS. We selected the EQ VAS as a primary outcome measure for its holistic representation of overall QoL as one numeric score that does not limit the participant to a specific source of QoL, such as walking or dressing; given its subjectivity, it is also possible that the data collection process, which simultaneously assessed for mRS and BI may have biased participants to interpret health in terms of functional mobility. Finally, the data reported in this study were collected before the introduction of new therapies that reduce disability for some patients, 15 although these therapies are unlikely to have altered the associations between dependence as measured by mRS and QoL as measured by EQ VAS.
Conclusion
Our cohort study suggests that patients with residual functional dependence after stroke may still enjoy a good QoL. Health care providers and health care systems need to consider these findings when communicating, planning, and delivering appropriate person-centered care. Stroke researchers may consider incorporating multiple types of outcome measures such as the EQ VAS to capture aspects of morbidity aside from physical disability. 16 More research is needed to understand how to best measure and improve QoL after stroke.
Funding Information
This study was funded by National Institute of Neurological Disorders and Stroke grant K23 NS099421 (C.J.C.); National Institute of Neurological Disorders and Stroke grant K23 NS02119 (D.L.T.); and Medic One Research Foundation (D.L.T.).
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.