
Abstract
Background:
The pediatric literature describes reliance on community-based organizations for home-based palliative and hospice care for children.
Objective:
To quantify and describe the inclusion of children in services, staffing, and care scope offered by community-based hospice organizations in the United States.
Design and Subjects:
This study utilized an online survey distributed to organizational members of the National Hospice and Palliative Care Organization (NHPCO) in the United States.
Results:
A total of 481 hospice organizations from 50 states, Washington DC, and Puerto Rico responded. Twenty percent do not provide services for children. Nonmetro geographies are less likely to provide services for children. Pediatric services provided include home-based pediatric hospice (57%), home-based palliative care (31%), inpatient pediatric hospice (23%), and inpatient pediatric palliative care (14%). Hospice annual pediatric census is an average of 16.5 children, while palliative care annual census is an average of 36. Less than half (48%) of responding agencies have a team that is dedicated to only pediatric care. Medicaid and the Children's Health Insurance Program are the most common forms of reimbursement, with 13% depicting “no reimbursement” for provision of care for children and many relying on philanthropy coverage. Lack of trained personnel, discomfort, and competing priorities were depicted as the most common barriers.
Conclusions:
Children remain underrepresented in the extension of care offered through community-based hospice organizations in the United States particularly in nonmetro settings. Further research into strong training, staffing, and reimbursement models is warranted.
Introduction
The pediatric literature describes gaps in hospice and palliative coverage for children.1–4 Home-based pediatric palliative and hospice services currently rely on the inclusion of children in coverage offered by community-based hospice organizations.5,6 These organizations have the potential to extend key provision of high-quality care for children relevant to supportive care and end-of-life care. 7 The extent to which children are able to access care provided by community-based hospice organizations in the United States remains unknown.
A national survey of children's hospitals in the United States found that 119 (80%) had a pediatric palliative care (PPC) program and 29 (20%) did not. 5 An equity expectation and access opportunity would be for all children's hospitals to offer PPC services. Over the past 6 years there has been a decrease in the presence of PPC programs and their service reach in the United States. 8 While access to hospice care for children slightly increased over the past decade, 9 as of 2020, more than half of children's hospitals reported still not having access to hospice services for children (n = 82, 55%). 5 For settings with access to home-based hospice services, the reliance is on adult-based hospice teams clustered around city settings.10–12
The purpose of this national survey of hospice organizations was to report on the state of existing pediatric hospice and palliative care services for children in the United States to include an overview of the population served, the services offered, the reimbursement schema, the staffing model and training of staff, and the perceived barriers or enablers to extending care for children. While the study focuses on the quantification of service reach, the ultimate reality is that gaps in the extent of services translates into unmet needs for children and families who may prefer to experience life at home. 6 This article presents the results of a survey of community-based hospice organizations to better understand how pediatric patients are or not being served, particularly in regard to home-based access.
Materials and Methods
Design and sample
The study design was a cross-sectional survey using an electronic questionnaire distributed to the National Hospice and Palliative Care Organization (NHPCO) members. The organizational purpose of the NHPCO is to lead and mobilize the transformation of care delivery to ensure equitable access to high-quality interdisciplinary, person-centered care for those living with serious illness. Due to wide geographic coverage and diverse demographic distribution, NHPCO membership was selected as the cohort due to being representative of most community-based hospice and palliative care organizations within the United States.
Organizations in the United States registered as members of the NHPCO were asked via e-mail correspondence to designate a knowledgeable employee to complete the study survey via an e-mail invitation to the organization's medical director with two follow-up reminders sent in 2-week intervals. One response was accepted per hospice. The link to the online survey remained open from June 15 to November 1, 2020. Participants were not offered incentives for survey completion.
Instrument
The study group consisted of an interdisciplinary team representative of medicine, nursing, public health, law, health care ethics, epidemiology, and health policy both as NHPCO Pediatric Working Group members and as NHPCO staff. Survey questions were designed by a collaborative, interdisciplinary study group consisting of seven team members according to the Tailored Method of Survey Design. 13 The survey instrument is available as Supplementary File S1. NHPCO's Pediatric Advisory Council, comprising 25 interdisciplinary hospice leaders, pretested the first survey draft as expert reviewers for content and clarity. The second survey draft was then independently reviewed, piloted, revised, and repiloted by an interdisciplinary team (two physicians, four nurses, one social worker, one chaplain, and one mixed methodologist) before field administration on Qualtrics XM©.
For purposes of the survey, the study team utilized a shared working definition of hospice as an interdisciplinary Medicaid benefit for children and adolescents with an anticipated life span of 6 months or less. Palliative care was defined as a supportive care and quality-of-life interdisciplinary care service. Concurrent care was defined as the continuation of disease-directed interventions in addition to hospice support. The variables measured in the survey included the following: description of the population (ages, medical conditions, and referral source); description of pediatric services (home/inpatient pediatric hospice or palliative care and additional offerings such as concurrent care, telemedicine, respite, and integrative therapies); pediatric census and length of enrollment; staffing models (disciplines, contractual agreements, and credentials of staff); reimbursement plans; and summary of barriers and enablers to pediatric inclusion.
Data analysis
The Office of Human Subjects Research Protections at the University of Nebraska determined that the survey format and content qualified as exempt from full Institutional Review Board review. Responses were aggregated and anonymized. The analyses were descriptive and univariate. The study team utilized counts for categorical variable responses. For missing responses due to skip patterns in the survey, the number of responders was used as the denominator (actual n). Frequencies and percentages are presented with recognition that the survey format allowed for selecting “all that apply” rather than multiple choice (thus percentages often add up to >100%). Variables were analyzed using chi-square tests or Fisher's exact tests when expected cell counts fell below 5.
This article includes the semantic content analyses for the free-text responses to the two questions: “Anything else you want us to know about your organization” and “any other comments about pediatric palliative or hospice care?” to categorize barriers and facilitators to providing pediatric services. Two members of the study team independently applied “facilitator” or “barrier” labels to key phrases in the free-text answers to capture their meaning and to develop a code dictionary. The code dictionary contained the definition of each “facilitator” or “barrier” and an example of use of the code. Team members then used this grouped-specific codebook to categorize the content of the free-text responses.
To explore the presence of services in rural or urban geographies, zip-code application of metropolitan areas was based on the Office of Management and Budget (OMB) delineation. The term nonmetro encompassed rural and suburban areas, while the term metro encompassed urban areas. The Federal Information Processing System (FIPS) Codes for States and Counties were applied to uniquely identify geographical areas. Shapefiles for counties and states were downloaded December 12, 2022, from the U.S. Census Bureau website. Maps were created using ArcGIS Pro software version 2.7.0 (Esri, Inc., Redlands, CA).
Results
The response rate was 59% (n = 481/815). Respondent demographics are provided in Table 1. Responding hospices included all 50 states plus Washington DC and Puerto Rico. Twenty percent of respondents did not provide hospice or palliative care for pediatric-age cohorts. There was not a statistically significant difference in terms of total (all-age) patient census, staffing size, geographic region, and financial model (not for profit or for profit) between those agencies that do and do not provide pediatric services. Thirty percent of respondents reported that their organization had declined to care for a child in need of services, while 70% reported they had not declined care for a child.
Demographics
Pediatric population
Age groups served by hospices, the most common diagnostic categories, and referral sources are described in Table 2. In the respondent's geographic area, the nursing/medical community was depicted as being very aware (11%), somewhat aware (50%), somewhat unaware (25%), and not aware (14%) of the advantages of hospice and palliative services for seriously ill children. Approximately two-thirds (66%) of responding hospice organizations reported provision of information of pediatric services on their organization's website or brochures, while one-third (33%) reported not announcing pediatric care through these modalities.
Description of Population Served and Referral Source
More than one answer per question allowed.
PPC, pediatric palliative care.
Pediatric services
Services provided for children and adolescents by those organizations that include this demographic in care are shown in Figure 1. The most common services included the following: patient and family education (36%), pain and symptom management (35%), bereavement care (35%), advance care planning (30%), and counseling (30%). The majority of respondents provided in-home visits (78%). Additional ways services are provided included telemedicine (20%), inpatient residential care (17%), home health skilled nursing visits separate from hospice nursing visits (12%), and private duty home health coverage (<1%). Integrative therapies included music therapy (25%), pet therapy (22%), art therapy (17%), massage therapy (16%), deep breathing (13%), healing touch (11%), aromatherapy (8%), Reiki (8%), meditation (7%), yoga (3%), acupuncture (2%), and chiropractor (<1%). No integrative therapies were available to patients receiving pediatric services in 10% of settings.
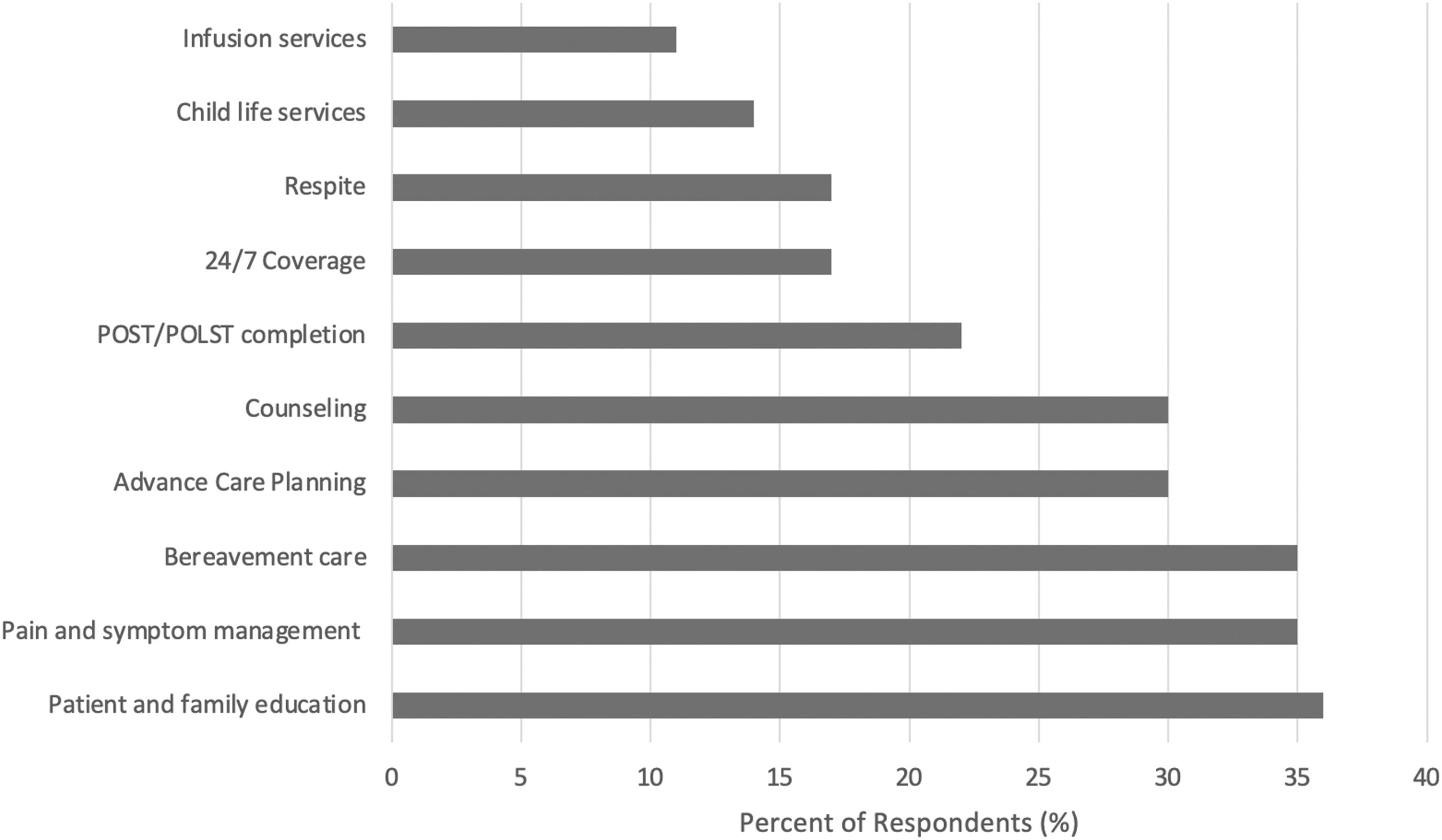
Services provided for children (including only respondents who enroll children). More than one answer allowed.
Pediatric hospice and palliative coverage, census, and concurrent care
Among the hospices (or palliative care providers) providing care to children, the census varied by hospice and palliative services. The daily and annual pediatric hospice and palliative census numbers are reported in Table 3. Hospice service duration for children and adolescents was reported as an average of 146.6 days (median 90 days). Average PPC service duration was reported at an average of 215.1 days (median 0 days). Three-fourth (76%) of responding agencies have utilized concurrent care for children, while one-fourth have not.
Annual and Daily Pediatric Service Census
n = The number of community-based organizations that offer pediatric care (%).
Geographic considerations
Results revealed lower access to all services in nonmetro areas. Pediatric home hospice is offered in 22% of nonmetro counties versus 40% of metro counties. Pediatric inpatient hospice is offered in 18% of nonmetro counties versus 27% of metro counties. Pediatric home palliative care was offered in 12% of nonmetro counties versus 30% of metro counties. Pediatric inpatient palliative care was offered in 16% of nonmetro counties versus 23% of metro counties. Visual depiction of counties, which were indicated to be covered by at least one hospice organization for pediatrics according to survey respondents, is provided as Figure 2. Counties indicated as not being covered by a given service (shaded in light gray) may actually be covered by an entity that either did not receive or respond to the survey.

Counties with pediatric services in the United States based on NHPCO survey respondents (2020). Countries that were indicated to be covered by at least one community-based hospice organization for pediatrics: home hospice, home palliative care, inpatient hospice, and inpatient palliative care, according to the 2020 NHPCO survey respondents. Counties indicated as not being covered by a given service may actually be covered by an entity that either did not receive or respond to the survey. NHPCO, National Hospice and Palliative Care Organization.
Pediatric staffing
Less than half (48%) of responding agencies had a team that was dedicated to only pediatric care. For those 118 responding organizations with staff dedicated to pediatrics, the team consisted of a registered nurse (87%), social worker (82%), physician (77%), chaplain (65%), advance practice nurse (41%), child life specialist (30%), integrative therapist (32%), and certified nursing assistant (28%). To staff pediatric-specific teams, almost half (46%) of responding agencies contracted out roles. Staff members with certifications in pediatrics included physicians (14%), registered nurses (13%), advance practice nurses (7%), child life specialists (6%), social workers (5%), alternative therapists (3%), chaplains (3%), and certified nurse assistants (<1%).
Pediatric reimbursement
Medicaid (25%) and the Children's Health Insurance Program (CHIP) (25%) are described as common forms of reimbursement for PPC. Additional sources of reimbursement included private insurance (17%), waiver programs (7%), and out-of-pocket (3%). “Other” reimbursement sources were selected by 12% of respondents. Notably, “other” reimbursement sources were then defined in the free-text box as “charity” or “donations” or “gifting.” Thirteen percent of respondents reported that “no reimbursement” is the most common occurrence among pediatric patients. Similarly, Medicaid and CHIP composed more than half of pediatric hospice reimbursement. Respondents depicted private insurance as composing 30% of pediatric hospice reimbursement. No reimbursement (11%), waiver programs (6%), other source (3%), and out-of-pocket payment (3%) composed the remainder of responses for the most common reimbursement source.
Sixty-eight percent of programs received philanthropy support for their pediatric palliative programs. Eleven percent of respondents described philanthropy funding over half of the pediatric palliative programs, 5% depicted philanthropy covering three-fourth of the program, and 5% depicted the PPC program being fully funded by philanthropy.
Barriers and facilitators to providing pediatric care
Barriers and facilitators to providing pediatric services are depicted in Table 4. The most commonly cited barriers/challenges to providing pediatric services for all survey respondents included the following in order of most to least frequently reported: lack of pediatric trained personnel, discomfort in caring for pediatric patients, competing priorities within the organization, no demand, and lack of funding/reimbursement. The most common barrier cited by settings providing pediatric services was lack of funding/reimbursement, while the most common barrier cited by settings not providing pediatric services was lack of staffing.
Perceived Barriers and Facilitators to Providing Pediatric Services
NHPCO, National Hospice and Palliative Care Organization.
Adequate staffing, reimbursement and funding, staff training/education, more referrals/requests, pediatric protocols, organizational leadership, stronger relationships with primary health care providers, specialized pediatric medical equipment, community resources, and parent advocates were recognized as enablers to help the organization offer pediatric services in that order of frequency. Online modules (42%), in-person education (35%), and direct mentorship (23%) were recognized as the most helpful form of pediatric-specific training for hospice and palliative care teams.
Respondents depicted ongoing staff training and education (30%), more staff with pediatric expertise (27%), more funding (23%), community partnerships (23%), stronger relationships with primary health care systems (21%), pediatric protocols (18%), medical coverage for pediatric primary care (17%), specialized pediatric medical equipment (13%), organizational policy/leadership (12%), and the presence of parent advocates (12%), as ways their organization would be better equipped to provide PPC. More than one-quarter of respondents (27%) expressed interest in incorporating pediatric services as an available service, while half (49%) expressed “maybe” being interested and one-quarter (24%) did not express interest.
Discussion
The goal of this study was to report the NHPCO membership survey findings regarding the provision of home-based and inpatient pediatric hospice and palliative care specifically for pediatric-age patients in the United States. A majority of programs had provided care for children, with the most common services provided being home-based hospice, followed by home-based PPC, inpatient hospice, and inpatient PPC. Less than half of respondents had a dedicated PPC program. Common barriers to pediatric care services were lack of trained staff, discomfort in caring for children, competing priorities, and lack of reimbursement.
Three-fourth of the 50,000 annual pediatric deaths in the United States occur in acute-care settings. 14 Data from the Children's International Project on Palliative/Hospice Services (ChiPPS; now the Children's Project on Palliative/Hospice Services) acknowledge that on any given day, 5000 pediatric-age patients with complex chronic conditions in the United States were in their last 6 months of life. 15 With those statistics in mind, this survey revealed that hospice organizations have woefully low pediatric enrollment. Nationally, access to hospice care for children has increased over the past decade, coinciding with the landmark passage of the Affordable Care Act Section 2302 (Concurrent Care for Children Requirement) requirement for all state Medicaid programs to pay for both curative and hospice services for patients <21 years of age with a life-threatening illness and documentation of anticipated death in less than 6 months.9,16
While concurrent care hospice has increased “potential” access to hospice for children, there remain multifactorial gaps in “realized” access to include the staffing, actual funding, training, and willingness of community-based services to enroll children. Although prognostic uncertainty was not listed as a picklist option of barriers in this survey, prognostic uncertainty is cited in the existing literature as a potential reason for delayed referral or missed enrollment opportunities.14,17,18 Future policy considerations may include extending the 6-month prognostic time line to a longer time line for pediatric cohorts to avoid missed hospice enrollment due to innate prognostic uncertainty.
The results of the survey emphasize the limited access to palliative care, especially in nonmetro settings, as PPC programs tend to be associated with larger, academically affiliated institutions. 5 Analysis shows ongoing disparity between rural and urban hospice and palliative care service coverage for children. The standing reality is that geographic location influences care options and access to services and subsequently the quality and location of a child's end of life.
We defined comprehensive palliative and hospice services as interdisciplinary team-based biomedical, psychosocial, and spiritual services that begin at the time of diagnosis; focus on the provision of curative therapies as well as comfort measures; and service children throughout the disease trajectory across care settings.14,19,20 We found that there was generally a lack of comprehensive hospice and palliative care services for pediatric patients. For example, the core hospice services of pain and symptom management were offered by only a third of respondents. Integrative therapies and child life services were even scarcer.
Contributing to lack of access and services is low staffing and resources. Many programs reported this barrier in their free-text responses, noting low frequency of pediatric admissions as a factor in lack of recruiting and retaining pediatric trained staff. Unfortunately this propagates a cycle of programs feeling ill-equipped to enroll pediatric patients, 21 thus reducing admissions, which then translates to lack of feasibility in retaining pediatric resources. Further exploration into what staff mean when reporting “discomfort” in caring for children is due to inform training and mentorship models to foster self-efficacy, confidence, and competence. Programs that do have staff reportedly comfortable in caring for children often times do not have staff with actual pediatric-specific training or the existing pediatric certifications offered through professional organizations as a combination of work hours and examination.
Potential solutions may include use of a spoke-hub model, telehealth support from pediatric-trained subspecialists for adult teams willing to care for children, improved funding models for pediatric training and staffing, and statewide consortia for the care of children. Relationally based support in the form of program champions and collaborations with subject matter experts (such as hospital-based PPC teams) may facilitate a readiness and improved ability to care for children.
The survey results revealed factors that appear to facilitate the ability for a program to care for children. Larger programs identified the ability to absorb costs related to caring for children. They identified the reimbursement from their larger adult population as a strategy to mitigate losses from providing poorly reimbursed care to children. These programs often identified having a larger geographic catchment area. Another facilitator was the presence of a pediatric champion on the interdisciplinary team (often a clinician) that could be leveraged to spearhead care for pediatric patients. This individual could also be utilized to support and educate other members of the interdisciplinary team in caring for children. An important facilitator for programs both currently enrolling children and those with plans to expand to enrolling children was awareness of the need and recognition of the current gap in palliative and hospice resources for children. 16
There are important limitations of this study. This study surveyed only NHPCO members and while this provides a national snapshot, the cohort may not be generalized beyond NHPCO membership. The sampling time interval included COVID pandemic months, which may have impacted the response rate. Survey methods are at risk of nonresponse bias and recall bias. To maximize answer accuracy, the survey invitation did request that the most knowledgeable person at the organization be responsible for responses in an effort to mitigate this possibility. Future research is needed to explore the quality of pediatric care provided for children and families and ways to extend not only enrollment but also care experiences for patients, family members, and staff.
Despite these limitations, the study has clinical implications. This survey demonstrates the need and opportunity to expand services for children. Streamlining enrollment logistics and improved education for staff is likely to increase access. Palliative care services, especially home-based palliative care, serve as a potential future option for the population of children who would benefit from rigorous home-based support, but do not meet the strict prognostic requirement of hospice. Through continued advocacy, support, and establishment of resources the care for children with life-threatening conditions can be further expanded upon to improve the scope and reach of support for pediatric patients navigating serious illness.
Footnotes
Acknowledgments
The authors extend their appreciation to the hospices and palliative care program respondents.
Authors' Contributions
M.S.W.: Conceptualization, methodology, and writing—original draft preparation. T.C. and K.S.: Software and statistics: D.F., H.F., B.H., K.J.: Investigation and reviewing and editing. S.S.: Writing—Original draft preparation. L.C.L. and C.T.: Conceptualization, methodology, and reviewing and editing.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No known conflicts of interest to disclose. Dr. M.S.W. participated in this project in a private capacity. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the U.S. Department of Veterans Affairs, the U.S. Government, or the VA National Center for Ethics in Health Care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.