
Abstract
A 78-year-old man with postoperative recurrence of esophageal cancer was admitted to the hospital due to chest pain and dyspnea. Oral short-acting opioids provided some relief, but chest pain persisted and worsened, leading to the initiation of a transdermal fentanyl patch. However, the patient developed opioid-induced urinary retention, which was treated with a naldemedine, a medication used for opioid-induced constipation and urinary retention. Opioid switching led to recurrent urinary retention, requiring placement of a urinary catheter. The patient ultimately required continuous deep sedation for refractory symptoms and died several days later.
Background
Opioids are frequently used to alleviate pain and dyspnea in cancer patients. However, they are associated with a range of side effects such as nausea, vomiting, constipation, drowsiness, and delirium. Although previous literature has examined the incidence of dysuria related to opioid use in cancer patients, the occurrence of urinary retention still lacks clarity.1–3
The mechanism of urinary retention is still not completely understood but is likely due to opioid-induced decreased detrusor muscle tone and force of contraction, decreased sensation of bladder fullness and urge to void, and inhibition of the voiding reflex. These effects likely involve both central and peripheral opioid effects. 4 Although naloxone was found to be very effective in reversing urinary retention, it also reversed the analgesic effect. 5 One study demonstrated reversal of opioid-induced bladder changes by methylnaltrexone, a peripherally acting μ-opioid receptor antagonist (PAMORA). 4
Naldemedine, a PAMORA designed for opioid-induced constipation, also inhibits the peripheral action of opioids without affecting centrally mediated analgesia. 6 It has been reported that a patient who experienced urinary retention after the initiation of opioids achieved complete resolution of urinary retention and well-controlled pain the day after receiving naldemedine. 7 However, there is a limited number of case reports available regarding pharmacotherapy for opioid-induced urinary retention in cancer patients, and it is crucial to accumulate more cases for further understanding and evaluation. We report a case of temporary improvement of opioid-induced urinary retention with the peripheral opioid antagonist naldemedine.
Case Report
A 78-year-old man was admitted to our hospital with chest pain and dyspnea due to disease progression of postoperative recurrence of esophageal cancer, which was causing increased lung and mediastinal lymph node metastasis. He had undergone pharyngolaryngoesophagectomy a year earlier, with the addition of an enterostomy. The clinical course is shown in Figure 1. Initially, oral short-acting opioids provided symptomatic relief, but chest pain persisted and worsened, so a transdermal fentanyl patch at 6.25 mcg/h was started. However, 11 hours later, he developed lower abdominal distention and had not urinated until then.
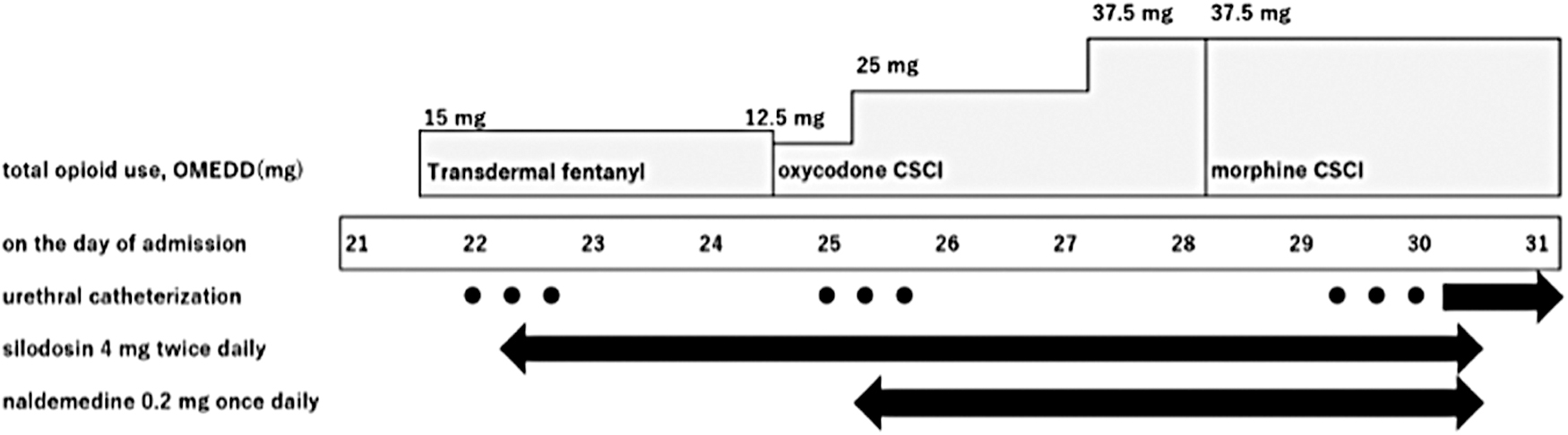
The chart displays urinary drainage and drug administration after hospitalization. The circle in the urethral catheterization column indicates a single voiding, with a total of three voidings, each on day 22, day 25, and from days 29 to 30. The arrows indicate indwelling catheters. Silodosin and naldemedine were initiated on days 22 and 25, respectively, and were continued until the catheter was placed on day 30. CSCI, continuous subcutaneous infusion; OMEDD, oral morphine equivalent daily dose.
After voiding, 300 mL of urine was obtained. No urinary tract diseases or infections were detected. Although he had been receiving medications related to urinary retention (antipsychotics and benzodiazepines), he had been receiving them for several days before the onset of retention, so we considered opioid-induced urinary retention. The day after starting silodosin, an alpha blocker used in patients with prostatic hypertrophy, urinary retention reversed. However, due to worsening chest pain and dyspnea, we switched him from transdermal fentanyl patch to oxycodone continuous subcutaneous infusion.
Five hours after opioid switching, he complained of urinary retention again. It was believed that urinary retention recurred due to incomplete cross-tolerance of opioids. Chest pain and dyspnea improved with opioid switching, but constipation persisted regardless of oral laxatives. We added naldemedine at a dose of 0.2 mg for constipation and urinary retention, based on reports that naldemedine is effective in opioid-induced urinary retention. 7 The patient was unable to take the medication orally, so the drug was administered through an enterostomy by simple suspension method.
Four hours after naldemedine administration, the patient was unable to urinate and experienced lower abdominal distention, which necessitated urinary drainage. However, the patient was able to resume urination spontaneously the day after naldemedine administration. No gastrointestinal (GI) adverse effects, such as diarrhea, nausea, vomiting, or abdominal pain, were observed. After two days, we switched him from oxycodone to morphine due to worsening dyspnea, but urinary retention reappeared. His general condition deteriorated, and he required repeated intermittent urethral catheterization, so a urinary catheter was placed. Continuous deep sedation was administered to him with refractory symptoms such as dyspnea and delirium for several days before his death.
Discussion
Opioid analgesics have been shown to increase smooth muscle and sphincter tone, leading to occasional urinary retention that likely involves both central and peripheral mechanisms.2,4,5,8 There has been only one previous report on the use of naldemedine for opioid-induced urinary retention. 7 In our case, urinary retention occurred three times after the patient was started on fentanyl and then switched to oxycodone and morphine. Although there was a temporary improvement in urinary retention after initiating naldemedine, urinary retention occurred again after switching from oxycodone to morphine.
Compared with the previous report, the effect of the PAMORA was found to be prompt, but not long lasting. These mechanisms may be attributed to the distinct binding affinities of each opioid for opioid receptors. Naldemedine acts as a noncompetitive antagonist of μ-opioid receptors. 6 However, the occurrence of urinary retention after opioid switching to morphine, which has a higher binding affinity for μ-opioid receptors than oxycodone, suggests its potential role in inducing urinary retention once again. 9
Naldemedine is generally well tolerated. However, GI disorders such as abdominal pain, diarrhea, nausea, and vomiting may occur. 10 Use of naldemedine early in the initiation of regular opioid is beneficial because it reduces adverse events. 11 The use of naldemedine is contraindicated in cases of GI obstruction, increased risk of recurrent obstruction, and conditions that may weaken the integrity of the GI tract walls due to the potential risk of GI perforation. 10
PAMORAs are μ-receptor opioid antagonists specifically designed to have limited ability to cross the blood–brain barrier (BBB). As a result, they selectively antagonize peripheral μ-opioid receptors while sparing central μ-opioid receptors. However, patients with a disrupted BBB are thought to be at increased risk for opioid withdrawal or reduced analgesia. 12 Therefore, caution should be exercised when using naldemedine in patients with brain metastases. In addition, naldemedine undergoes hepatic metabolism primarily through the CYP3A pathway. Therefore, concurrent use of CYP3A4 inhibitors may elevate the blood concentration of naldemedine, potentially intensifying its opioid receptor antagonist effects. 10
Mercadante et al. reported the prevalence of opioid-induced dysuria in patients admitted to a palliative care unit. 2 They found that male gender, the presence of a pelvic mass, and previous pelvic surgery or opioid switching were associated with urinary retention. In the present case, male gender and prior opioid switching were identified as risk factors for urinary retention. Tolerance of urinary retention can develop rapidly, 5 but catheterization may be necessary to manage transient problems. 3 However, catheterization is invasive and can cause a decrease in quality of life.
Therefore, rapid improvement in urinary retention with medications would be beneficial, especially for patients with a poor prognosis. In addition, if naldemedine proves to be effective in improving symptoms, it may have the potential to prevent opioid-induced urinary retention. However, there is currently no data to support this, and further reports are eagerly anticipated.
The limitations in this case are several. First, it is possible that the improvement in urinary retention was the result of the rapid development of tolerance rather than due to the administration of naldemedine. Duration of urinary effects of epidural morphine lasts as long as 14 to 16 hours. 5 In this case, opioids were administered through continuous subcutaneous infusion, and the duration of the urinary effects is unclear. Second, the effectiveness of the drug administered through an enterostomy is uncertain. Although there is insufficient data on enterostomy administration, this case demonstrated an improvement in constipation after the initiation of naldemedine, indicating the drug's effectiveness in enterostomy administration.
This case suggests the effectiveness of PAMORA in opioid-induced urinary retention, as seen in previous reports. 7 However, once observed, it was noted that the effects of naldemedine did not last long. This suggests that the opioid switching to a higher binding affinity opioid may have diminished the efficacy of naldemedine. The use of PAMORA could be considered when opioids are the principal cause of urinary retention. Reports on the treatment of urinary retention induced by opioids are lacking in the cancer population. Future studies should be performed to examine this observation.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.