
Abstract
Background:
Some clinicians suspect that patients with do-not-resuscitate (DNR) orders receive less aggressive care. Extrapolation from code status to goals of care could cause significant harm. This study asked the question: Do DNR orders in the intensive care unit (ICU) lead to a decrease in invasive interventions?
Methods:
This was a retrospective cohort study of ICU patients from three teaching hospitals. All ICU patients were assessed for inclusion. Exclusion criteria were medical futility and death, comfort care, or ICU discharge <48 hours after DNR initiation. Five hundred thirty-six patients met inclusion criteria. One hundred forty-five were included in the final analysis. Primary outcomes were occurrence of invasive interventions after DNR initiation—surgical operation, central line, ventilation, dialysis, or other procedure. Secondary outcomes were antibiotic administration, blood transfusion, mortality, and discharge location.
Results:
Patients with DNR orders underwent fewer surgical operations (14.5% vs. 31.1%, p = 0.002), but more central lines (42.1% vs. 23.0%, p = 0.009), ventilator use (49.0% vs. 18.9%, p < 0.001), and dialysis (20.0% vs. 4.1%, p = 0.002), compared with patients without DNR orders. Transfusions and antibiotic use decreased similarly over admission for both groups (transfusions: β = 1.25; p = 0.59; and antibiotics: β = 1.44; p = 0.27). Mortality and hospice discharges were higher for DNR patients (p < 0.001.).
Conclusions:
DNR status did not decrease the number of nonoperative interventions patients received as compared with full code counterparts. Although differences in populations existed, patients with DNR orders were likely to receive a similar number of invasive interventions. This finding suggests that providers do not wholesale limit these options for patients with code status limitations.
Introduction
Do-not-resuscitate (DNR) orders instruct health care teams not to perform cardiopulmonary resuscitation (CPR) after cardiac arrest. However, many clinicians suspect that care starts to be limited before cardiac arrest for patients with simple DNR orders.1,2 This concern may be driven by personal biases; studies have demonstrated that providers may equate DNR orders with end-of-life care. 3
This bias has been documented to contribute to fewer procedures being offered during preoperative care discussions with surgeons.4–6 If inpatient care teams also extrapolate from code status for overall goals of care, this bias has high potential for harm, especially in the intensive care unit (ICU) where patient acuity leads to a higher volume of urgent interventions.
Parsing causality related to patient mortality at the end of life has become more complex as approaches to care at the end of life have become more nuanced. Studies to date have reported that patients with DNR orders tend to have higher mortality rates than full code counterparts.1,7–20 Some have reported decreased rates of both invasive8,10,14 and noninvasive12,20,21 interventions.
On the other hand, other studies have shown no differences in morbidity or other measured quality of care metrics.13,15,17,19,22 Confounding the interpretation of some of these studies are the significant qualifying data that are omitted such as the timing of DNR orders, whether patients received only comfort-oriented care, and whether DNR orders coincided with impending death. 23
Overall, it remains unclear whether DNR orders drive changes in care or if other factors influence both changes in code status and care intensity. Patients who limit certain aspects of their care (i.e., CPR) may be more likely to limit other aspects as well. These patients may be sicker at baseline or have more contact with the health care system, giving them a better understanding of the implications of aggressive interventions. However, if code status changes affect provider perceptions of overall goals of care and decrease other aspects of care, they must be identified and addressed.
This study is unique, in that it assessed the impact of DNR order status across a disparate ICU population. While previous studies have attempted to address this issue for specific patient populations, this study looked more broadly at and included multiple types of both medical and surgical ICUs. We aimed to determine whether code status impacts the incidence or continuation of multiple invasive interventions in the ICU.
Methods
This retrospective cohort study compares rates of invasive procedures in ICU patients with DNR orders with matched full code patients. Retrospective chart review of ICU patients at three large academic institutions in Salt Lake City, Utah, and Washington, DC, was performed. ICUs studied include the burn, trauma, neurological, and general surgical ICUs at MedStar Washington Hospital Center (MWHC); medical, surgical, burn, and cardiovascular ICUs at the University of Utah; and a combined medical, surgical, and cardiac ICU at the George E. Wahlen VA Hospital in Salt Lake City.
The study was reviewed by institutional review boards (IRBs) at the MedStar Health Research Institute (IRB ID MOD00001037, approved June 10, 2019), University of Utah (IRB No. 125656, approved January 31, 2020), and Salt Lake City VA (IRB No. 00125656, approved February 5, 2020) and determined to be exempt (study title: “Care Quality in the Surgical Intensive Care Unit after Do-Not-Resuscitate Order Initiation: A Retrospective Analysis”). The studied period was from April 2018 to May 2019. Study data were accessed from May 2019 through January 2022.
Inclusion criteria were (1) discharge from the ICU during the study period and (2) an ICU stay duration after DNR initiation (or DNR equivalent in the unexposed group) of at least 48 hours before discharge or death. Exclusion criteria were (1) discharge from the ICU, death, or transition to comfort care <48 hours after DNR orders were placed and (2) clear medical futility, as documented by multiple provider notes. These exclusion criteria were selected to minimize the number of studied patients with DNR orders placed solely as a bridge to death.
Medical futility inevitably drives care limitation in this patient population. Although DNR orders may have also impacted provider perceptions about patients' desire for aggressive interventions in this group, determining if care was limited due to those biases versus because that care was no longer medically indicated would be impossible to differentiate. Whether providers make erroneous assumptions about prognosis and thus recommend DNR orders and less aggressive care for specific patient subgroups was not the subject of this study.
The exposure of interest was “DNR status” during or before ICU admission. The unexposed group comprised full code patients matched to exposed patients based on age, length of stay (LOS), and gender. They must have been admitted to the ICU at least 48 hours after average DNR status initiation for exposed patients (on average, patients received DNR orders at 48.5% of hospitalization for MWHC and 60.5% for University of Utah). No unexposed patients were collected at the Salt Lake City VA due to limitations of the electronic medical record and ability to collect data.
For brevity and ease of understanding, in the unexposed group, pre-DNR and post-DNR signify the corresponding periods during hospitalization before and after average DNR order initiation, respectively, in the exposed group. Consideration was given to matching by National Surgical Quality Improvement Project (NSQIP)-collected comorbidities, Acute Physiology and Chronic Health Evaluation (APACHE) II score, and individual institution severity indexes. However, due to missing data (such as Glascow Coma Scale [GCS] scores and pH values for APACHE II), heterogeneity of patient populations across ICU subtypes, and differences in institution-specific severity of illness stratification systems, these were not practical.
Primary outcomes were incidence or continuation of the following five invasive interventions post-DNR: surgical operation (hereafter referred to as “operation”), central line use, ventilator use, dialysis, or other invasive procedures. Operative and other invasive interventions were recorded only if they occurred after DNR orders were placed. Dialysis, central line use, and ventilator use were recorded if these were continued after DNR initiation, even if initiation occurred before code status change.
If receiving an operation, invasive ventilation must have been continued at least 48 hours after the operation (meeting the definition of delayed extubation). Other invasive procedures included bronchoscopy, chest tube placement, interventional radiology procedure, and other interventions, which were performed with relatively low frequency. Secondary outcomes were antibiotic administration, blood product transfusion, mortality, and discharge location. As all outcomes were interventions, data for these were readily available across groups.
We also evaluated whether patients had code status conversations documented on admission and whether DNR orders were placed due to previously expressed patient values or poor prognosis. Previously expressed values were identified based on family meeting notes and advance directives. Poor prognosis was similarly determined from provider progress notes and family meeting notes stipulating that the reason for the code status conversation was poor prognosis.
Locations searched for evidence of interventions included daily progress notes, operative notes, procedure notes, and institution-specific locations for the recording of surgeries, antibiotics, and blood product administration.
Statistical methods
For descriptive statistics, we calculated proportions for categorical variables and medians and interquartile ranges (IQRs) for continuous variables. To compare the demographic distributions, we used the chi-squared (χ 2 ) test for categorical variables (or Fisher's exact test when the cell sample size is ≤5) and Wilcoxon rank sum tests for continuous variables.
Primary outcomes were assessed using logistic regression and multivariable logistic regression. Statistical significance remained similar between methods (Supplementary Table S1). Reported data are adjusted for age, gender, LOS, and site. We used the same statistical approaches to compare primary and secondary outcomes between the two groups and reported proportions or medians as appropriate.
For blood product and antibiotic administration, the number of days of therapy pre-DNR order was compared with the number of days post-DNR order. These differences were assessed using linear regression with pre-post difference as the dependent variable and group status as the independent variable. We report the slope (β) and its p value to indicate the difference in the pre-post change of the outcome and its statistical significance, respectively, between the two groups.
Analyses were conducted using Stata, version 17, and an alpha level of 0.05.
Results
There were 536 patients who met inclusion criteria and 145 were included in the final analysis. A total of 391 patients were excluded, with 290 being excluded due to either clear futility (29) or proximity of code status change to death or comfort care (261). Only 74 patients met inclusion criteria as unexposed patients. Challenges included several exposed patients with very long LOS (25 patients stayed 30 days or longer, maximum LOS 168 days) and the need for unexposed patients to remain in the ICU at least 48 hours after average DNR order initiation in exposed patients.
Gender was similar between groups (exposed 55.2% male vs. unexposed 56.8%; p = 0.82). Matching was not fully successful: the exposed group had longer LOS (median, 13.0 days vs. 9.1 days; p = 0.001) and was older than the unexposed group (73 years vs. 69 years; p = 0.004) (Table 1).
Demographic Characteristics (n = 219)
For categorical variables, the chi-squared test was used (Fisher's exact test when a cell sample size is ≤5). For continuous variables such as age and length of stay, the rank sum test was used.
CVICU, cardiovascular intensive care unit; DNR, do-not-resuscitate; ICU, intensive care unit; IQR, interquartile range; MICU, medical intensive care unit; UofU, University of Utah; VA, Veterans Affairs; MWHC, MedStar Washington Hospital Center.
Fewer patients with DNR orders received operations than full code patients in the post-DNR period (14.5% vs. 31.1%, odds ratio [OR] 0.24 [0.10–0.60]; p = 0.002). However, they were more likely to receive dialysis (20.0% vs. 4.1%, OR 8.21 [2.20–30.67]; p = 0.002), have central lines (42.1% vs. 23.0%, OR 2.44 [1.25–4.75]; p = 0.009), and experience ventilator use (49.0% vs. 18.9%, OR 7.23 [3.24–16.11]; p < 0.001). Differences between the incidence rates of other invasive procedures were not statistically significant (30.3% vs. 24.3%, OR 1.59 [0.79–3.18]; p = 0.19) (Fig. 1).

Primary outcomes—invasive interventions adjusted for age, gender, length of stay, and site. Statistical significance did not change when unadjusted logistic regression was performed, nor when the site was not included in the multivariable logistic model.
We compared differences in blood product and antibiotic use before and after DNR initiation using linear regression. Both groups experienced a decrease in both interventions over the course of their hospitalization. The pre- and post-DNR differences were compared between groups and were not statistically different (blood products: β = 1.25; p = 0.59; and antibiotics: β = 1.44; p = 0.27).
Discharge locations were compared using Fisher's exact test. Mortality rates and discharge to hospice were higher for DNR patients (cumulatively 58.62% vs. 4.05%) and discharge to home or a rehabilitation facility was less likely (cumulatively 28.80% vs. 83.78%) (Fig. 2).
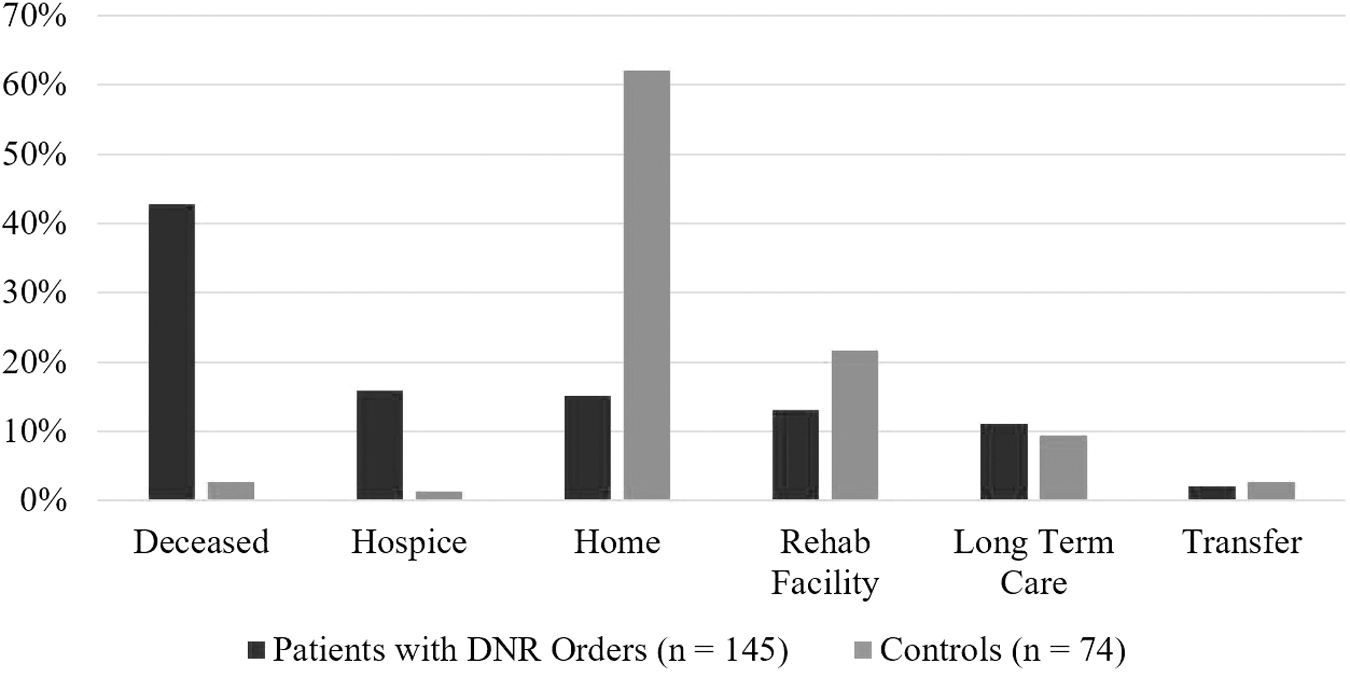
Discharge location. The p value is <0.001, calculated using Fisher's exact test.
Additionally, we collected data on whether DNR orders were placed because of patient's prior wishes or due to poor prognosis. We compared the incidence of primary and secondary outcomes between these two groups within the exposed population and found that the only statistically significant difference between groups was in ventilator use. The group of patients who had previously expressed that they would want DNR initiation were less likely to undergo ventilator use (Table 2).
Primary and Secondary Outcomes Based on Reason for Do-Not-Resuscitate Order Initiation
Three patients did not have information regarding the reason for DNR.
Finally, we evaluated whether exposed patients had code status conversations documented on admission. The results varied widely across types of ICUs and institutions as followed, with remarkable differences even among similar types of ICUs at different institutions (Table 3).
Distribution of Patients by Intensive Care Unit Type and Documentation of Admission Code Status
Neuro, neurological intensive care unit.
Discussion
Overall, we found no evidence that ICU patients with DNR orders had fewer interventional procedures than full code-matched patients, except with respect to surgical operations. While the differing mortality rates suggest that our comparison groups were not fully matched on severity of illness, increased rates of invasive procedures in the DNR group argue against severe withholding of indicated procedures. While some providers worry about the impact of DNR orders on overall patient care, this provides some reassurance that providers do not limit invasive nonsurgical interventions indiscriminately.
Differences in surgical interventions in the DNR order cohort may stem from differences not reflected in documentation. Surgeons may have consulted with patients and determined that surgical intervention would be nonbeneficial. If so, this determination may have been biased by preconceptions about DNR orders. However, it is equally possible that due to the underlying severity of illness, both CPR and operative interventions are unlikely to be beneficial.
Alternatively, intensivists may have declined to call surgical consults altogether for this population for either of the above reasons. This study was not designed to address these nuances. Regardless, it is important to remember that surgeons play an important role in the delivery of care across the spectrum of a patient's life.
Across ICU types, there was heterogeneity in documentation of code status discussions on admission. This likely, in part, reflects different patient demographics; several charts for trauma and burn patients noted the inability to find surrogate decision makers, making discussions about code status impossible. This may also reflect differences in medical culture.
The Patient Self-Determination Act has been interpreted by some to mean that all patients should be asked about their code status by a physician on admission. In fact, it stipulates that patients must be asked by someone whether they have an advance directive and are informed of their right to create one. 24 If preadmission code status is determined by staff in the context of admission screening questions, physicians must be careful not to miss preexisting DNR code statuses.
We compared patients with DNR orders due to previously expressed values with patients with limitations in their code status due to prognosis. These two groups represent different clinical scenarios with disparate reasons for treatment limitations. We hypothesized that patients with DNR orders placed due to poor prognosis would have higher mortality rates, as has been shown elsewhere. 16
Interestingly, both groups had similar mortality rates and received similar numbers of interventions (except for intubation, which was likely driven largely by DNR and Do Not Intubate [DNI] orders at baseline in the group with prior values). Differences in severity of illness (acute vs. chronic) and in patient preferences between the two groups could have influenced this result.
This study focused on whether DNR orders by themselves impact administration of care beyond performance of CPR after cardiac arrest. DNR orders are often placed for one of two reasons—either because of patient wishes (either before admission or in the face of new medical data) or as a bridge to death when the medical team becomes certain of care futility. This latter patient population was not the subject of this study and they make up most of the excluded patients.
In fact, there were more patients for whom DNR orders were used as part of care de-escalation than there were included patients. We drew this distinction because in patients with DNR orders as a bridge to death, the overall clinical trajectory would appropriately direct both care limitation and DNR order initiation, rather than DNR orders influencing care limitation. DNR order use in the process of care de-escalation appears to be quite common and is an interesting subject for future research.
Overall, few patients died without a DNR order; similar findings have been documented in other studies.25,26 This study was not designed to study postcardiac arrest outcomes. However, when CPR was successful, but patients subsequently died, the overwhelming majority were first assigned DNR status rather than passing away because a code was terminated. From a research perspective, many of these patients were excluded from the study, as discussed above, making it challenging to find unexposed patients who match the exposed group in disease severity.
Although this study allowed for granularity of information because individual charts were evaluated, there was heterogeneity in coding for treatment limitations. Extrapolating this information systematically was challenging; for example, where “no vasopressors” is stipulated, should those patients be included in the central line use metric (because there are other reasons to have a central line placed) or not (because most patients who do not want vasopressors are likely to decide this to avoid invasive interventions)?
Ultimately, we opted to ignore whether other limitations of care were stipulated and analyzed the data based on interventions performed. We felt this strategy would be least susceptible to subjectivity, although another approach could have been to exclude these patients on a limited (intervention specific) or wholesale basis.
This study did not collect data regarding when dialysis, central line, or ventilator use was initiated (i.e., whether these were started before or after DNR order initiation). Some of what appears to be increased intervention rates in the DNR group may be due to physician hesitance to withdraw care.
We suspect that most of the observed differences between groups are due to higher severity of illness of the exposed group since this population had longer lengths of stay and increased invasive interventions. Unfortunately, given the heterogeneity of the patient populations (surgical, cardiac, neuro, and medical ICUs), matching was not possible. However, we chose to study ICUs generally because if providers extrapolate from code status for overall goals of care, the fast-paced and often emergent nature of interventions in this environment has high risk of harm.
To our knowledge, the impact of DNR orders in this population has not yet been studied in this way. Given the difficulties experienced in ensuring similarity between exposed and unexposed populations, future studies should consider standardized prospective data collection or selecting a narrower study population. In the latter strategy, obtaining a sufficient sample size in a more specific ICU population would be challenging.
Goals of care and code status conversations are difficult; intricacies about decisions made in these conversations are even more challenging to convey to other providers. In this chart review, it was evident that many providers make good faith attempts to understand patients' wishes. However, carrying these wishes out in clinical practice involves provider judgment. In addition, these conversations are sometimes either not had or not documented well. In these cases, it is impossible to know whether patient wishes were carried out.
Given the above issues, reducing the intricacies of code status conversations to binary variables about whether interventions were performed is fraught with potential for bias, subjectivity, and inaccurate interpretation.
Conclusions
Overall, across this multicentered and multidisciplinary study, we found no evidence that ICU patients with DNR orders had fewer interventional procedures than full code-matched patients, with the exception of surgical operations. The significance of the decreased surgical operations is unclear, but the sustained number of other interventions suggests that providers do not wholesale limit these options for patients with limitations in their code status.
Heterogeneity in documentation of patient goals of care was widespread in the evaluated patient charts. Clear goals of care conversations are critical to treating patients in a goal-concordant manner, and documenting those conversations allows other providers to do the same. This study had limitations with respect to ensuring similar severity of illness between exposed and unexposed populations. It should be considered as idea generation for future studies on this topic.
Footnotes
Acknowledgments
The authors would like to thank Andrea Ryan, RN, whose work over a decade ago on perceptions of care after DNR orders led to the creation of this project. The authors would also like to thank Brian Locke, MD, for his assistance with reviewing the methods of this article and the Biostatistics Department at the University of Utah for their assistance in identifying unexposed patients from that institution.
Authors' Contributions
K.E.D and L.S.J. had full access to all of the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. K.E.D., L.M.K., and L.S.J. conceived and designed this study based on prior studies, as cited in the ![]() section. All authors were involved in acquisition of data. K.E.D., L.M.K., and K.C.A. analyzed and interpreted the data and drafted the manuscript. K.C.A. performed the statistical analysis. All authors were involved in critical revision of the manuscript.
section. All authors were involved in acquisition of data. K.E.D., L.M.K., and K.C.A. analyzed and interpreted the data and drafted the manuscript. K.C.A. performed the statistical analysis. All authors were involved in critical revision of the manuscript.
Disclaimer
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences, the Department of Defense, or the U.S. Government.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.