
Abstract
Institutional transference is a phenomenon describing patients' attitudes toward the institutions where they receive mental health or medical care. While transference toward individual clinicians in palliative care has been described, attitudes of patients with serious illness toward the institutions where they receive specialized care have not been described. Here, we present three cases which demonstrate the phenomenon of institutional transference in patients with serious illness and the resulting clinical implications, which include countertransferential responses of clinicians caring for them. We consider three conditions: (1) the idealized reputation of the academic cancer center, often a tertiary referral center; (2) loss of an institutional connection during care transitions; and (3) countertransferential reactions to institutional transference. We highlight characteristics and personality styles of individuals with cancer that may complicate and intensify institutional transference and identify potential interventions to address common challenges associated with institutional transference.
Originally defined as the attitudes and feelings that individuals with serious mental illness experience toward psychiatric institutions where they receive treatment, 1 the term institutional transference has come to encompass the analogous phenomenon experienced by those with serious medical illness toward medical institutions, a perception of them as “holy places of pilgrimage and healing.” 2 In either versions, the institution becomes central to the treatment experience, and some people facing illnesses develop greater attachment to a particular institution than to individual clinicians.
On one level, the experience of institutional transference presents potential benefits to both the individual facing illness and their treating clinicians. For the individual, these include an inclination to closely adhere to treatment protocols, satisfying relationships with providers, and a greater sense of stability when provider switches are necessary within an institution.3,4 For the clinician, positive institutional transference on the part of patients can serve to heighten emotional investments in those patients and, in turn, job satisfaction. However, institutional transference can also present unique clinical challenges. Enhanced expectations of care can increase the sense of dependency of ill and vulnerable patients. Intense emotional involvement with patients may lead to clinician stress and even burnout, particularly when boundaries between professional and social relationships are blurred.
While the relevance of both transference and countertransference reactions in the palliative care setting have been explored, 5 the concept of institutional transference toward cancer centers has received little attention. Here, we describe transferential reactions of individuals with cancer toward their cancer center and countertransferential responses of their oncologic providers, as well as their clinical implications. We highlight characteristics and personality styles of individuals with cancer that may complicate and intensify institutional transference. In particular, we consider three conditions: (1) the idealized reputation of the academic cancer center, often a tertiary referral center; (2) loss of an institutional connection during care transitions; and (3) countertransferential reactions to institutional transference. We identify potential interventions to address common challenges associated with institutional transference in Table 1.
Suggested Interventions for Challenges Posed by Institutional Transference
Idealization of the Academic Cancer Center
A serious illness such as cancer typically leads to uncertainty and distress regarding outcomes and prognosis, and therefore, both individuals with rare forms of cancer and those who have failed standard treatment often travel great lengths in search of state-of-the-art or experimental treatments at specialized centers. Their feelings of desperation can heighten expectations which may make it difficult to accept limitations of the institution's clinicians and care.
A man in his twenties with advanced sarcoma traveled abroad to a United States' academic cancer center in pursuit of clinical trial participation. Due to disease progression, he was removed from the trial some months later, with the recommendation to return to his home country to continue standard chemotherapy. He declined referrals to other academic cancer centers for a second opinion, and repeatedly requested that his treatment teams consider surgical and experimental treatments which had been deemed high risk and futile for his case. His providers expressed feelings of helplessness and at times frustration about the situation and consulted psychiatry for help with management of the patient's anxiety in the context of limited treatment options and likely terminal disease.
This patient's initial idealization and later devaluation of the cancer center (demonstrated by his refusal to accept repeated clinical recommendations) can be understood as splitting, an unconscious psychological defense employed to overcome intolerable ambivalence toward an object (labeling one aspect of an experience as entirely good, and another as entirely bad). In the case of cancer centers, it can be very difficult for patients to tolerate ambivalence about whether the institution can save their lives. After first magnifying a providers' or institution's positive qualities, they may then see them in an overly negative light, manifested as anger, rejection, denial, or withdrawal from care.
High patient expectations may create complex countertransference reactions. Although the idealized provider may at first feel special or important, they may later feel inadequate and helpless when unable to meet these expectations. This may result in blurring of boundaries (e.g., giving patients their cell phone numbers, or significant between-visit contact) to meet the idealized standard—potentially fueling their own annoyance with the patient and, cumulatively, burnout. Patients' devaluation also commonly evokes in providers feelings of frustration and defeat. Recognizing the transference and countertransference contributions to these feelings can help providers acknowledge their own ambivalence and achieve perspective.
Loss of an Institutional Connection in Transitions of Care
Institutions often provide individuals with cancer a safe holding environment through the frequent contact with the providers involved in their treatment. Transitions of care away from a valued institution can present an often under-appreciated loss for patients, heightened by individual vulnerabilities.
A man in his twenties with a history of depression lost his father three months prior to a diagnosis of stage IV Hodgkin's lymphoma. During his treatment, he developed a strong attachment toward the psychiatrist he saw weekly for psychotherapy at the cancer center. He began to reach out frequently between sessions, resulting in his psychiatrist setting limits on communication. His cancer was treated successfully, and he was informed that he would have less frequent visits with the oncology team and would eventually transition to a community mental health provider. He made a suicidal gesture the day after he completed active disease treatment.
It may be helpful to understand the transference aspects of this case through the lens of object relations theory. Everyone contains an inner, often unconscious, world of relationships consisting of self-representations and object (other) representations (parents, past role models or figures). 6 These internal representations, which form from repeated interactions over time, are then often used unconsciously to predict behaviors in others (Fig. 1). Transference occurs when feelings are transferred from the original object to an external object, specifically onto a physician or analyst, 7 or in this case, institution. These positive or negative feelings can inform the way an individual relates to their care providers.
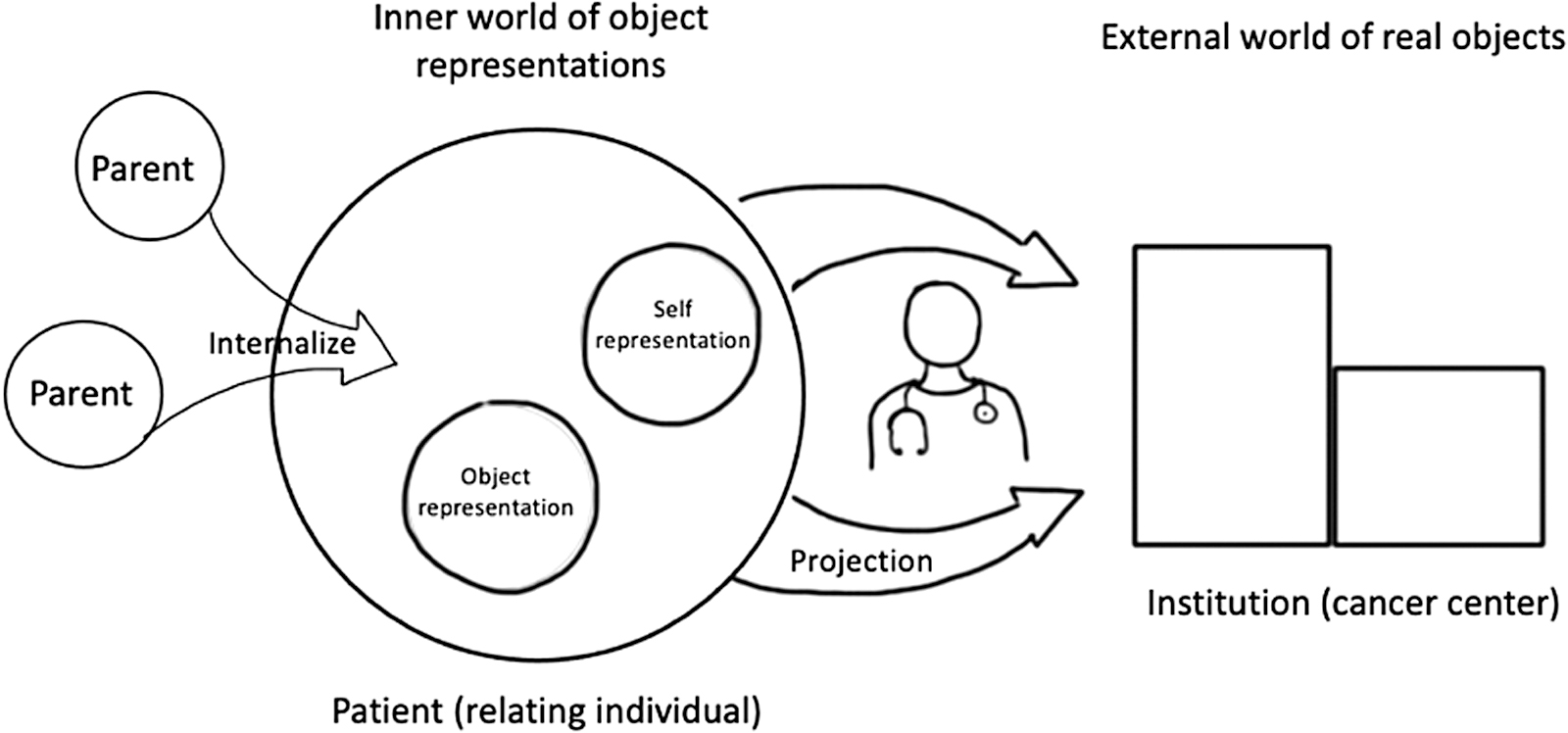
Object relations theory and institutional transference. This figure illustrates the basic principles of object relations theory, in which a relating individual (in this case, the patient) brings with them an internalized set of self and other representations which through projection, they impart onto external others, or objects, they interact with (in this case, the institution). Clinicians (presented with stethoscope) may be intermediaries in patients relating to the institution.
Even when the object is lost, the patient can hold onto an internalized representation of the good object, which may ease the anxiety of separation from the object. If object loss occurs before successful internalization, patients may experience profound separation anxiety, presenting with depressed mood, anger, or in more severe cases, suicidal gestures, or attempts. Cancer patients may internalize the caring function of the institution and their care team, and as they transition out of active treatment into either survivorship or hospice, experience object loss as they experience less frequent contact with the institution. Patients with unstable internal object representations, insecure attachments, and regressed states may be particularly vulnerable to this transference during transitions of care.
Identifying individual patients' vulnerabilities to object loss and separation anxiety can lead to greater sensitivity during transitions of care. It is also helpful to communicate with all patients during their treatment what will be expected trajectory of their relationship with the cancer center, including some acknowledgment of the possible emotional impact of a transition from active treatment to surveillance or hospice care. An active discussion of the frame, or parameters, of treatment can contain anxieties associated with transferential reactions.
Countertransference Reactions and Their Clinical Implications
Just as the institution may engender transferential feelings in the patient, its reputation may influence the feelings of clinicians working there. Providers may experience a variety of countertransference reactions to their intensely engaged patients who have sought them out as experts at an elite cancer center.
A woman in her seventies with GBM being followed for symptom management by the cancer center psychiatrist transitioned to home hospice care, and her family insisted her oncologist remain the physician of record. The oncologist had formed a close relationship with the family, which included exchanging personal phone numbers and being available for questions around the clock. As she transitioned to hospice and began to deteriorate, she required more assessments, medication titration, and support than the oncologist and outpatient psychiatrist could provide. This created confusion and anger among the family, and among staff.
Strong institutional transference can provoke separation anxiety in patients who are then perceived as “needy” or “clingy,” which may evoke frustration in providers, motivating them to reinforce interpersonal boundaries and distance themselves from patients' care. Conversely, providers who are highly invested in their patients in ways akin to friendships may experience an undue sense of responsibility (perhaps enhanced by their perceived role as experts at an elite cancer center), difficulty delivering bad news, feelings of inadequacy, heighted grief responses, burnout, and interstaff conflict.8,9 This may lead to providers staying involved with certain patients or avoiding discussion of their own plans to leave the service.
The primary intervention for provider countertransference is proactive and timely education to help providers identify and articulate their reactions to patients' attachments to the institution, especially during transitions of care. Venues for discussing these complex relationships include orientation, supervision, and case conferences involving interdisciplinary teams.8,9
Conclusion
Greater awareness of patients' transference reactions to the specialized institution providing them potentially life-saving care, and the countertransference responses of clinicians who find themselves recipients of idealization and/or devaluation can enhance the management of particularly vulnerable patients, stressful transitions of care, and decisions regarding boundaries.
Funding Information
No funding was received.
Footnotes
Author Disclosure Statement
No competing financial interests exist.