
Abstract
The World Health Organization defines palliative care by its focus on improving quality of life (QOL). Although reducing suffering is part of improving QOL, it should not be the sole focus of our efforts. Opportunities for joy, meaning, love, and growth exist in the midst of serious illness and should be explored and supported even in the face of suffering. Intentionally focusing on these outcomes expands provider's toolset for improving QOL, creates opportunities to better understand, celebrate, and support the full humanity of the person in front of us, and may increase the satisfaction of practice for clinicians. The “Total Enjoyment of Life” provides a framework for reminding clinicians to systematically address positive outcomes. This framework can also be used to suggest clinical strategies for promoting positive outcomes and expanding the scope of interventions and outcomes to be considered in clinical research.
There Is An Important Difference Between Improving Quality of Life and Reducing Suffering
The most recent World Health Organization (WHO) definition of palliative care (PC) focuses on improving quality of life (QOL). 1 Although “improving QOL” and “reducing suffering” may appear interchangeable, these goals are conceptually distinct. 2 Importantly, WHO's definition of QOL explicitly includes both positive and negative dimensions that may interact but are nevertheless separate. 3 In other words, optimizing well-being for an individual may involve not only efforts to reduce suffering but also efforts to enhance valued aspects of being alive.
It is important before moving forward to clarify what we mean by “positive” and “negative” as both words have multiple definitions and connotations. By “positive” we are referring both to the presence or addition of a quality as well as its subjective valence (the individual considers it good). Thus, although the outcome of reducing pain is clearly “positive” in the sense of good to the individual, it is not the focus of this article as it is attained by reducing an undesirable state. We would also like to acknowledge that not all suffering is negative. In many religious and spiritual traditions, suffering can be ennobling, redemptive, meaningful, and actively embraced. Although it is beyond the scope of this article to delve deeply into this topic, we would like to emphasize the importance of understanding an individual's relationship to different types of suffering as we explore concepts such as meaning, hope, and transcendence.
Outside of the clinical setting, it is widely recognized that positive outcomes, such as joy, meaning, and love, are essential to living a good life and that some suffering is to be expected in these pursuits.4,5 Within clinical care, focusing on the positive is equally important if we hope to move from patient-centered care, care that focuses on a person defined and limited by their illness and suffering, to person and family-centered care, care that acknowledges the whole person in front of us, including their strengths, joys, and goals outside of the medical context. 6
Many in the field of PC and psychiatry have intuitively and purposively brought in aspects of the positive side of QOL into their work, including asking questions around what that person enjoys or is looking forward to in their assessment, incorporating larger life goals into plans of care, and focusing on building meaning as a therapeutic strategy.7–11 Although individual clinicians may view these practices as an essential part of the care they provide, systematic efforts to integrate these positive dimensions of practice into education, models of clinical care, or frameworks of the guiding principles of care have been limited. A mental model for thinking about positivity in the face of serious illness will help us be more systematic in screening for and suggesting ways for patients to improve their QOL.
The “Total Enjoyment of Life” Framework for Systematically Exploring and Promoting Positive Outcomes
The concept of the “Total Enjoyment of Life” arises from the converse of two influential conceptualizations of suffering in PC. First is Eric Cassell's groundbreaking work defining suffering as an inherently subjective and individual experience that arises from the meaning an individual attributes to their illness. 12 Using a similar framework, joy can be conceptualized as a positive counterpoint to suffering. 2 Aspects of joy emphasized in this definition are its subjective nature, the diversity of experiences from which joy is derived, and the central role of the individual in defining joy for themselves based on their life experiences, values, and idiosyncrasies.
Second is the “total pain” of illness, one of the most enduring and influential concepts in Dame Cicely Saunder's corpus of work promoting PC. 13 The multiple dimensions of “total pain” provides a memorable and practical framework for PC clinicians to systematically assess and address potential sources of suffering. We propose an analogous framework to systematically assess and promote enjoyment of positive outcomes in the context of serious illness (Fig. 1). As with total pain, the dimensions (physical, cognitive, emotional, social, and spiritual) and examples provided are meant to be suggestive rather than exhaustive and may serve as a starting point for more comprehensive assessment and support.
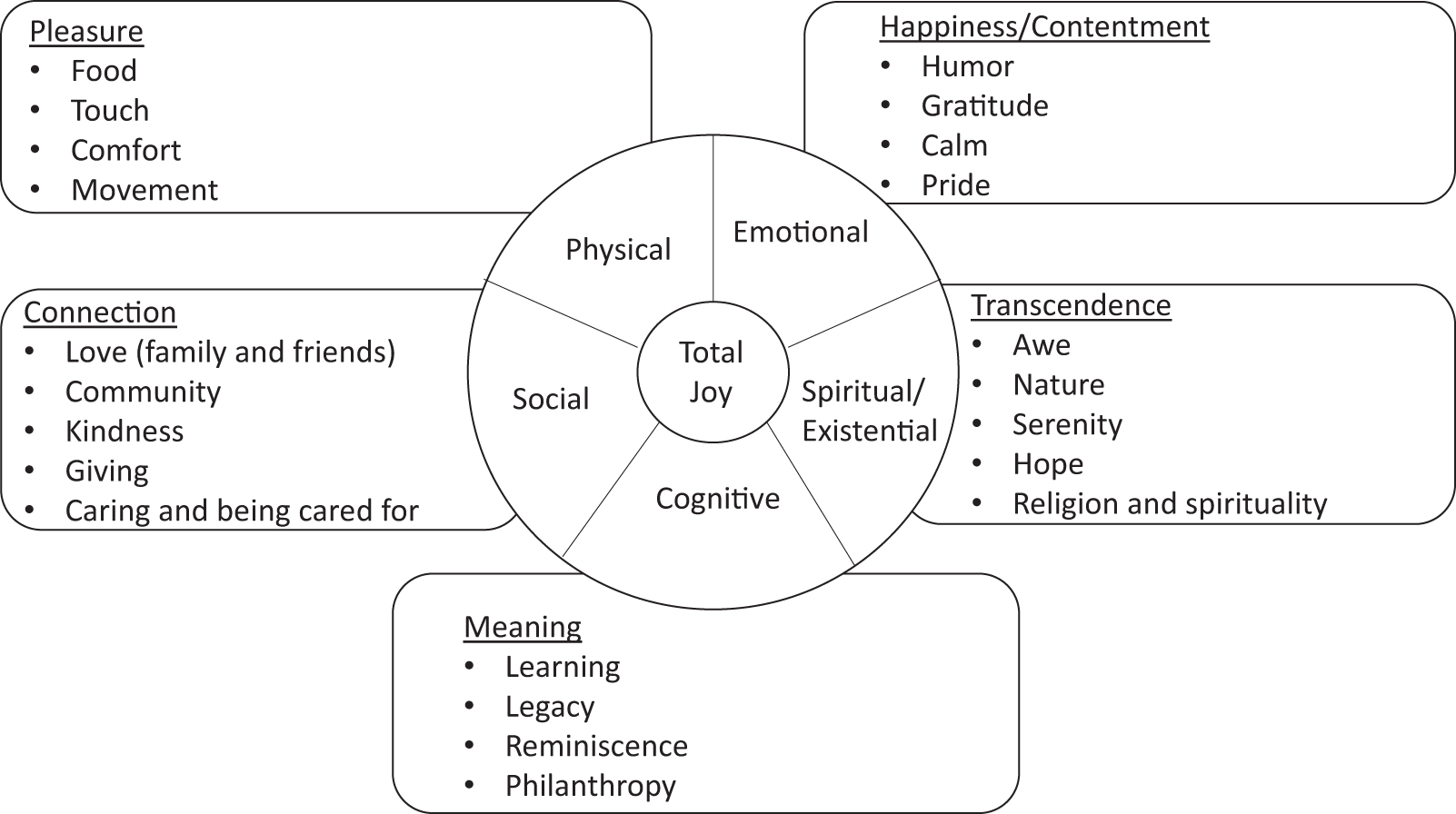
Analogous framework to systematically assess and promote enjoyment of positive outcomes in the context of serious illness.
Just as PC teams may create templates to assess potential sources of total pain (e.g., physician asks about physical pain and chaplain asks about spiritual distress), a team could utilize a positive review of systems to assess physical pleasure, cognitive meaning, spiritual transcendence, happiness (or other positive emotions such as gratitude), and social connection/love. Questions could include how important that dimension is to an individual, how satisfied they are with their current state of enjoyment, and what opportunities could be created to increase engagement in that dimension.
Of note, we thought deeply on the word we wanted to use to convey positive emotions. Joy struck one of us (R.M.A.) as too high a bar and seemed to ignore meaningful experiences that were not “joyful.” Pleasure was a lower bar, yet ignored nonsensory positive experiences. Although we are using enjoyment and joy in this article, we are open to other terms that more accurately reflect the converse of suffering. We believe other terms (e.g., contentment and satisfaction) or phrases (e.g., total pleasure and being fully alive) could easily be used to capture the underlying construct and encourage readers to find language that resonates with them and their patients. It is interesting that we could not find a single word that perfectly conveyed the opposite of suffering.
Strategies for Assessing and Promoting Positive Outcomes
Similar to recommended approaches to assess sources of suffering, it is helpful to start with broad questions that allow the patient or family to raise those issues that are most salient or important to them and then to follow with more specific questions to ensure nothing essential is missed. As a starting point, clinicians can ask patients about their overall QOL at an initial meeting. If rated as fair or better, this can be followed up with the request to “Tell me about those parts of your life that you enjoy or look forward to.” If rated as poor or worse, this can be followed by, “I'm curious to know if there are parts of your life that you enjoy or look forward to.”
If patients respond to either request with a null response, it may be helpful to ask, “Tell me about the things you used to enjoy” or “Tell me about your life prior to this illness.” Asking patients to tell you about the past 24 hours of their life (“tell me what you did yesterday from the time you got up to when you went to bed”) 14 is another way to see if there any parts of the patient's life that brings her/him some positivity. The dimension of time is important to keep in mind as pleasure may be savored in the past (e.g., reminiscence therapy around favorite memories, pictures, or songs), in the present (e.g., mindfulness), or the future (e.g., planning an anticipated event).
The language of hope may provide openings and insights into these areas and may resonate with certain providers and patients. Asking “When you look to the future, what do you hope for?” can allow exploration of opportunities for love, meaning, and enjoyment, and may provide important perspectives. Similarly, explorations of important relationships, community, religion, and spirituality may identify opportunities to heighten engagement through love with life. Family or caregivers, if present, may provide additional insights into potential sources of enjoyment for the patient now or in the past.
Regarding supporting positive outcomes, we propose explicitly considering both “sources of suffering” and “opportunities for enjoyment” in the clinical assessment and for intentionally creating a space for patients and families to hold both. For some patients moving this assessment into a plan can be as simple as encouragement to pursue enjoyable activities. We can ask, “What one thing might you do tomorrow that would bring you some pleasure or meaning?” For patients who need time, we give it to them to think about and report back at our next visit. For people who are resistant, we acknowledge that in the midst of suffering, asking about positive experience may seem incongruous and explain our goal is to see if it is possible to bring even a sliver of pleasure into their life. We often have to give examples of what we mean—a television show they enjoy, sitting outside for 15 minutes or talking with grandchildren on the phone is a start. The goal is to focus on any positivity in the here and now. 15
This is reinforced by making concrete steps around these goals and including them in plans. For example, “eating ice cream at least three times a week,” “getting outside at least once on the weekend,” or “tell your wife thank you before going to bed” can create enjoyable routines and creates permission to enjoy life openly. Notably, gratitude practices may heighten appreciation of positive aspects of life and can be an enjoyable activity in their own right. 16 Clinicians may also support more special or elaborate events, such as helping to make a mobile home wheelchair or walker accessible, or encouragement to plan a family get together. For patients with rapidly progressive illnesses, this support may include encouragement to pursue certain activities sooner than later.
As PC is meant to offer support to both patients and families, it is important that we also include families and carepartners in our assessment and promotion of positive outcomes. Along these lines, providers can include questions for carepartners around positive outcomes in their assessment such as “do you have time for things you enjoy in your life” and “we often focus on burdens, but what are the positive aspects for you of caring for this person.” Likewise, we can include plans to promote enjoyment for carepartners as individuals, focus on meaning or other positive aspects of caring in their caregiving role, and build on positive aspects of their connection to the patient, including friendship, teamwork, and love.
Finally, as a positive way to close-out visits, particularly ones where difficult topics were discussed or news delivered, can be encouragement to do something easy and pleasurable, or at least less stressful, at the end of the day or weekend (i.e., “closing the box on difficult topics”). 17 For example, “We talked about a lot of tough things today and I know it wasn't what you wanted to hear. I wonder what we might do to close this conversation and see if there is something you could do over the next few days that would bring you some enjoyment?”
Striking a Balance Between Acknowledging Suffering and Allowing the Potential for Enjoyment
It is important to note that the intent of the “Total Enjoyment of Life” is not to deny suffering or the harsh realities of serious illness. Nor is it meant to promote dogmatic styles of positive thinking that attribute magical powers to positive intention, a strategy that often leaves a trail of guilt for the sufferer, and blame from true believers, who feel that one is not being positive enough. 18 One can state this intention explicitly when getting into the plan of a visit, “We want to make sure that we acknowledge your suffering, help you to work with it, and do our best to lessen it when possible. We also want to give you and your family encouragement to enjoy the time that you have and find opportunities for joy, love and meaning when possible.” This can also be framed around not having regrets for things left undone or unsaid.
As with goals of care or other components of the palliative approach, positive outcomes do not need to be discussed at every visit and should be used at the discretion of providers in the context of their relationship with individual patients and families. There are notably times where discussing joy or other positive outcomes may be inappropriate and insensitive. For example, severe or urgent physical or psychological distress needs to be managed first to provide space for more positive feelings and actions.
That being said, with practice and skill, there is often more room for the positive in serious illness than most patients or providers would imagine. Our goal is to help patients and families infuse their lives with pleasure and meaning. This specifically includes end-of-life care, a time when spirituality, hope, love, gratitude, awe, and joy may be particularly valued and impactful.19–21 Notably, loss of the ability to participate in joyful activities is a leading reason patients request medical aid in dying (MAID) and suggests MAID discussions should also explicitly include conversations around sources of joy.22,23
Opportunities to Expand and Enrich PC Research
The field of PC may benefit in several ways from the intentional inclusion of these concepts. Regarding research, the “Total Enjoyment of Life” framework may prompt the inclusion of nontraditional but, from a patient or family perspective, critically important outcomes and outcome measures in clinical trials. 24 Importantly, these outcomes may represent some of the gaps between the largely positive experience patients, families, and clinicians have with PC and the disappointing statistical results of clinical trials, some of which may have chosen the wrong outcome. 25 More importantly, researchers can develop and test interventions that specifically engage with positive aspects of life, such as meaning-making, humor, optimism, or enriching social connections.26,27
Although there have been modest efforts in this direction there is certainly more that must be done to bring these outcome measures into larger trials,28–31 and creative strategies may be needed to allow for the quantification of patient-defined positive outcomes based on an individuals' preferences and priorities.32,33 A complementary opportunity is recognizing joy as a therapeutic tool. Quoidbach et al. present an excellent review and framework for conceptualizing positive interventions that may be utilized to not only achieve positive endpoints but also to directly reduce pain and suffering.34,35
A Positive Future for the Field of PC
The “Total Enjoyment of Life” framework directly challenges many of the preconceptions and stereotypes people hold around PC. 36 Explicitly emphasizing these aspects of our work is consistent with recent evidence-based recommendations for improving messaging around PC. 37 Embracing the positive aspects of the care we provide may help providers find joy in clinical practice, 38 and including it in teaching may improve the effectiveness and engagement of our fellows and trainees. Finally, as PC tends to set trends in the culture of caring, these concepts have the potential to influence medicine more broadly as the field of PC works to improve, implement, and disseminate these ideas. By purposefully inviting joy, meaning, hope, and love into our work we draw on some of the most powerful forces at our disposal as healers and acknowledge the complexity and completeness of the human experience even in the face of change, loss, and grief.
Footnotes
Authors' Contributions
Writing—original draft, writing—review and editing, and conceptualization by B.M.K. Writing—review and editing, and conceptualization by R.M.A.
Funding Information
BMK received support from the National Institute on Aging (K02AG062745) related to this article.
Author Disclosure Statement
No competing financial interests exist.