
Abstract
Objective:
We investigated the role of rapid response systems (RRSs) in limitations of medical treatment (LOMT) planning among children, their families, and health care providers.
Methods:
This multicenter retrospective cohort study examined children with clinical deterioration using the Japanese RRS registry between 2012 and 2021.
Results:
Children (n = 348) at 28 hospitals in Japan who required RRS calls were analyzed. Eleven (3%) of the 348 patients had LOMT before RRS calls and 11 (3%) had newly implemented LOMT after RRS calls. Patients with LOMT were significantly less likely to be admitted to an intensive care unit compared with those without (36% vs. 61%, p < 0.001) and were more likely to die within 30 days (45% vs. 11%, p < 0.001).
Conclusions:
LOMT issues existed in 6% of children who received RRS calls. RRS calls for clinically deteriorating children with LOMT were associated with less intensive care and higher mortality.
Introduction
Arapid response system (RRS) is a medical safety system designed to identify and save hospitalized patients experiencing deterioration and thus improve patient outcomes. 1 Many reports have examined pediatric RRSs in Western countries such as Australia, New Zealand, the United Kingdom, and the United States. 2 Systematic reviews of those studies have shown that pediatric RRSs reduce hospital mortality and cardiopulmonary arrest outside the pediatric intensive care unit (PICU).3,4
In adults, several investigators have reported on limitations of medical treatment (LOMT; withholding of medically futile treatments) and initiation of end-of-life (EOL) discussions after RRS calls.5,6 Likewise for children, the concepts of EOL or LOMT have been examined in pediatric settings for acquired immunodeficiency syndrome, 7 oncology, 8 intensive care units (ICUs), 9 and postoperative status, 10 but not specifically in terms of the interplay with RRS. Elucidating the features of LOMT in the setting of pediatric RRSs and subsequent clinical courses may help health care providers better understand the determination of LOMT for children experiencing deterioration.
Our objective in this study was to clarify the frequency of implementation of LOMT in children, either pre-existing before RRS calls or newly implemented after RRS calls. We also compared the characteristics, triggers, interventions, and outcomes between children with and without LOMT who required RRS calls in Japan.
Materials and Methods
This study was approved by the institutional review board at the university (approval no.: 60-21-0077; approval date: August 24, 2021). The requirement for informed consent was waived because of the retrospective nature of this study. This retrospective cohort study was conducted using observational data collected through the In-Hospital Emergency Registry in Japan (IHER-J). Each hospital accessed the online registry form and registered all RRS calls.
This study included all patients from the total dataset. Exclusion criteria were as follows: (1) patients registered from a long-term care facility, (2) patients ≥20 years old, or (3) patients with missing data for LOMT. Details of dataset contents were published elsewhere in previous reports from the IHER-J.11–14
We collected information on patient characteristics, including age (categorized as “newborn and infant [0–11 months],” “toddler [1–3 years],” “preschool [4–6 years],” “school-age [7–12 years],” or “adolescent [13–20 years]”), gender, existing comorbidities (categorized as “malignancy,” “congenital heart disease,” “postoperative status,” or “sepsis”), admitting unit (categorized as “pediatrics,” “internal medicine,” “surgery,” or “other”), and setting (categorized as “inpatient” or “outpatient”). The timing of RRS calls was categorized into “day-shift” (from 08:00 to 16:59) and “night-shift” (from 17:00 to 07:59).
Hospital status was classified into two types (“university” or “nonuniversity”) and three hospital volumes (“small [1–500 beds],” “medium [501–800 beds],” or “large [801–1200 beds]”), according to the previous study. 15 LOMT were defined as withholding or withdrawing life-sustaining treatments such as cardiopulmonary resuscitation (CPR) in the event of cardiac arrest. Children with a care directive of “full code” order were defined as “without LOMT,” and those with a care directive of “partial code” or “do-not-attempt-resuscitation orders” were merged into “with LOMT.”
Furthermore, LOMT that had already existed before the RRS calls were defined as “pre-LOMT,” and patients with newly instituted LOMT after the RRS calls were defined as “new LOMT” in this study. In general, medical practice in Japan, members of responding team and treating physicians or nurses jointly make management decisions in consultation with the child and his or her parents (including the disposition of the child, goals of care, do-not-resuscitate orders, and LOMT) on a case-by-case basis, with a guideline, protocol, or decision-making support for each facility.
Triggers for RRS calls were classified as “respiratory” (tachypnea, bradypnea, new-onset breathing difficulty, or desaturation), “cardiac” (tachycardia, bradycardia, or hypotension), “neurological” (altered mental status, seizure, or agitation), “staff concern,” or “other.” RRS interventions included test orders, supplemental oxygen, fluid bolus, drug administration, tracheal intubation, or CPR.
Outcomes of interest were the patient disposition after the RRS call (death, admission to the ICU or high-dependency unit, or stay in the ward) and 30-day outcomes (death, hospitalization, discharge, or others) for children. Missing values in the dataset were dealt without imputation by analyzing only the available data, as missing data were considered likely to occur randomly.
Continuous data were described as median with interquartile range (IQR). Categorical data were presented as numbers and percentages. We compared variables between children with and without LOMT using the Mann–Whitney U test for continuous variables and the chi-square or Fischer's exact test for categorical variables, as appropriate. Values of p < 0.05 were considered statistically significant. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
A flow diagram for the cohort is shown in Figure 1. During the 10-year study period, the database included 348 children from 28 hospitals on the basis of the predetermined eligibility criteria. Characteristics of the study cohort are given in Table 1. Median age was 5 years (IQR: 1–15 years), with 192 boys (55%). Percentages of children with existing malignancy and congenital heart diseases were 12% (n = 41) and 20% (n = 70), respectively. We did not observe any identifiable trend in the proportion of children with LOMT over the course of the 10-year study period.
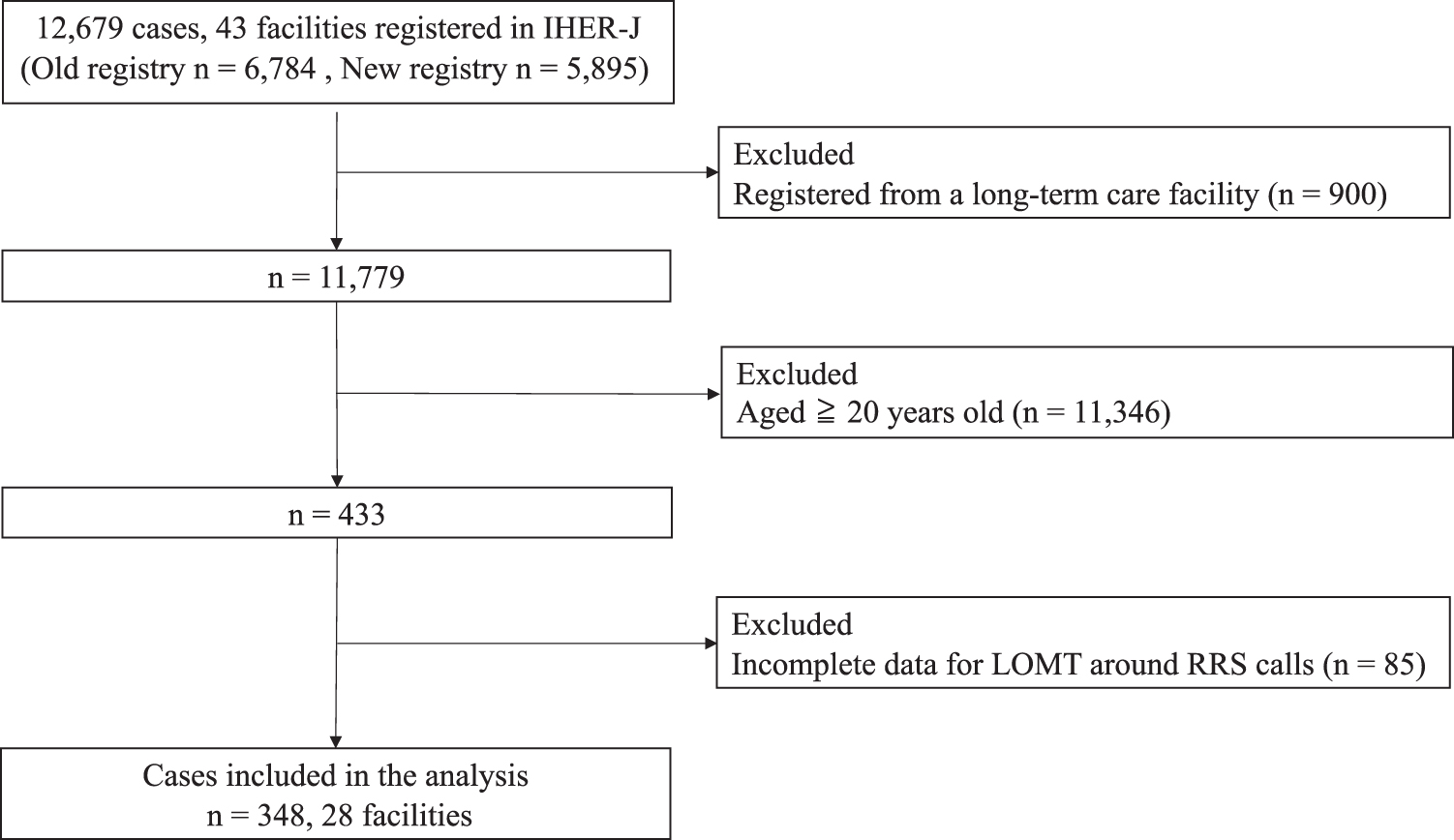
Patients flow chart. IHER-J, In-Hospital Emergency Registry in Japan; LOMT, limitations of medical treatment; RRS, rapid response system.
Characteristics of the Study Cohort
Compared between children without LOMT and with LOMT.
Without LOMT = children without LOMT around RRS activation.
With LOMT = children with LOMT around RRS activation.
With pre-LOMT = children with pre-existing LOMT before RRS activation.
With new LOMT = children with newly implemented LOMT after rapid response team activation.
IQR, interquartile range; LOMT, limitations of medical treatment; RRS, rapid response system.
Of the 348 children, 11 (3%) had LOMT in place before the RRS call (pre-LOMT) and 11 (3%) had LOMT newly implemented after the RRS call (new LOMT), respectively. Patients with LOMT (6%, 22/348) showed a higher frequency of malignancy than those without LOMT (27% vs. 11%, p = 0.033) (Table 1).
Table 2 presents triggers, interventions, and outcomes for RRS calls. In our study cohort, the major triggers for RRS calls were respiratory issues (n = 205, 59%) and staff concern (n = 107, 31%). Children with LOMT were more frequently triggered by cardiac reasons than those without LOMT (41% vs. 21%, p = 0.039). No children with LOMT received tracheal intubation.
Triggers, Interventions, and Outcomes for Rapid Response System Calls
Compared between children with and without LOMT.
Multiple answers allowed.
Respiratory = tachypnea, bradypnea, new-onset breathing difficulty, desaturation.
Cardiac = tachycardia, bradycardia, hypotension.
Neurological = altered mental status, seizure, agitation.
Without LOMT = children without LOMT around RRS activation.
With LOMT = children with LOMT around RRS activation.
With pre LOMT = children with pre-existing LOMT before RRS activation.
With new LOMT = children with newly implemented LOMT after rapid response team activation.
CPR, cardiopulmonary resuscitation; HDU, high-dependency unit; ICU, intensive care unit.
Patients with LOMT were less likely to be admitted to an ICU or high-dependency unit compared with those without LOMT (36% vs. 61%) and more likely to die after 30 days (45% vs. 11%).
Discussion
Our 10-year retrospective observational study examined differences in the clinical characteristics and outcomes of deteriorating children with and without LOMT who required RRS calls among 28 hospitals in Japan. The results showed that the percentage of children with LOMT was 6% in total. Compared with children without LOMT, children with LOMT appeared less likely to enter intensive care and showed a higher mortality rate.
In our cohort, 3% of our cohort received new LOMT after RRS calls, suggesting that RRSs may have a certain role in the decision-making process around LOMT for children with deterioration in Japan. We found that 1 in 30 patients had new LOMT after RRS calls in Japanese hospitals, compared with 1 in 20 patients (169/3531) in U.S. pediatric hospitals 16 and none (0/197) in an Australian urban teaching hospital. 17 This difference is consistent with earlier reports describing a higher prevalence of LOMT in the United States than in other countries, presumably associated with cultural differences. 18
In our study, the 30-day mortality rate for the whole cohort requiring RRS calls was 13%, suggesting that these patients represent a high-risk population with mortality even higher than those admitted to PICUs (1.3–5.0%). 19 Moreover, our finding of a 45% mortality rate among children with LOMT (and 60% in children with new LOMT) underscores both the importance of timely discussions about LOMT and the potential utility of members of the responding team as targets for training in goals-of-care discussions.
The strength of this report is that, to the best our knowledge, this represents the first multicenter study to evaluate the role of pediatric RRS in EOL care and the implementation of LOMT. We have reported differences in the characteristics and outcomes of children who had LOMT compared with children who did not. Our study highlighted that RRSs provide a potential opportunity not only to operate and palliate the underlying disease physiology, but also to initiate discussions about the goals, values, and LOMT for children. RRSs need to be reconfirmed to have the potential to improve the quality of EOL care in deteriorating children who might not benefit from further life-prolonging interventions.
Our study showed several limitations. First, given the differences in health care systems, generalization of the findings to other countries is difficult, given that patients, their families, and health care providers may have markedly different attitudes toward LOMT. Second, the database utilized did not contain detailed information on patient characteristics (e.g., genetic abnormalities, cognitive dysfunctions, or disease severity). Furthermore, this database also lacked detailed information on who initiated the discussion about LOMT, how members of responding team coordinated pediatric palliative care, or how treating physicians or nurses were informed about opportunities to discuss serious illness.
Although we found that children with LOMT were less likely to be admitted to an ICU and more likely to die within 30 days, we could not clearly determine whether discussions with members of responding team prompted any changes in outcomes for children. Third, RRS calls were less frequently required for pediatric patients compared with adults in this Japanese RRS registry. The small sample size of this study did not allow for the analysis of factors associated with LOMT among deteriorating children.
Further research involving the database with detailed information about LOMT is needed to better understand the factors influencing the LOMT decisions and the process of LOMT, to support shared decision making among children, their families, and health care providers.
Conclusions
We have demonstrated that LOMT were present in 6% of children with clinical deterioration, with 3% existing before RRS calls and 3% implemented after RRS calls. Children with LOMT were less likely to receive intensive care and showed a higher mortality rate than children without LOMT. Overall, further discussion is needed to determine the role of RRS for children with LOMT issues.
Footnotes
Acknowledgments
Authors' Contributions
T.T. contributed to conceptualization, methodology, software, validation, writing—original draft, visualization, and project administration. Y.S. was involved in conceptualization, methodology, validation, resources, and writing—review and editing. Y.K. carried out conceptualization and writing—review and editing. T.K. took charge of conceptualization, resources, and writing—review and editing. K.S. was in charge of conceptualization, supervision, writing—review and editing, and project administration.
Ethics Approval and Consent to Participate
The institutional review board of Nagoya City University Graduate School of Medical Sciences and Nagoya City University Hospital approved this study (approval number: 60210077, August 24, 2021) and waived the requirement for informed consent because of the observational nature of the study.
Availability of Data and Materials
The data in this article were provided by the In-Hospital Emergency Committee in Japan under license. The datasets used and analyzed during this study are available from the corresponding author on reasonable request with the permission of the In-Hospital Emergency Committee in Japan.
Consent for Publication
This article has been reviewed by all coauthors and permission for publication has been granted.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.