
Abstract
Objective:
The electronic health record (EHR) has emerged as a fundamental tool but has focused on physical care delivery. Psychosocial screenings and interventions are central to palliative care that supports whole person care models; however, EHR innovations to capture psychosocial care have not been optimized.
Material and Methods:
A narrative review was conducted from 2009 to March 2023. EMBASE, PubMed, and PsychINFO were queried to identify articles that discussed EHR tracking of psychosocial care in palliative care.
Results:
Eight articles met inclusion criteria representing a broad range of works in palliative care. Three themes emerged in the narrative review: (a) quality improvement strategy to support EHR tracking in collaboration with key stakeholders, (b) clarification of psychosocial domains for documentation and measurement, and (c) lack of standardization in data collection tools and processes.
Discussion:
This narrative review contributes to a limited body of literature on EHR extraction of complex sources of distress in palliative care. The designation of four domains (social history and distress, psychological symptoms, spiritual needs, and patients' goals and preferences) defines psychosocial practice aligned with palliative care quality metrics. Recommendations highlight the importance of shared priorities and collaboration with key stakeholders to fully execute on the clinical utility of EHRs. Future work will continue to evaluate data collection tools and systematic approaches to capture psychological needs and social environment and its impact on health outcomes and quality of life.
Conclusion:
This review will expand on opportunities for automated reporting of psychosocial care in the context of seriously ill.
Introduction
Palliative care conceptualizes patients as “whole persons” within a holistic, patient, and family-centered framework. Distinct from medical acuity in the traditional disease-focused treatment model, palliative care identifies and responds to a multitude of psychosocial needs that accompany a serious illness. Sources of psychosocial distress, which can be cognitive, behavioral, emotional, social, and/or spiritual in nature, manifest on a continuum throughout the disease trajectory.1,2 Psychosocial care instills an ecological approach recognizing contextual implications, such as environmental and social factors, in understanding and adapting to illness. 1 Environmental and social factors including housing and employment instability, food insecurity as well as mental health conditions and substance abuse are psychosocial drivers that influence health outcomes, acute care utilization, and costs.3,4
Psychosocial assessment and intervention are an essential tenet of palliative care practice. Although accepted as a foundational element in the field of palliative care, the direct impact of psychosocial dimensions of care on service utilization and patient experience are poorly described in practice and research. 5 This is, in part, because psychosocial care addresses complex needs and associated distress, which can be broad and variable. Thus it is difficult to universally define the essence of psychosocial care. Furthermore, psychosocial interventions have been considered “soft” and existing data criticized for lacking reliability and validity. 6
Capturing psychosocial care accurately has been particularly challenging in electronic health records (EHRs). There is not a systematic approach to collect information on the multidimensional view of patient needs.3,4,7 Enhanced data collection would foster more sufficient quantitative data to extract social factors and the effectiveness of psychosocial interventions in addressing nonphysical sources of distress.6–9 Meaningful use of health information technology was promoted through the passing of the U.S. Health Information Technology for Economic and Clinical Health (HITECH) Act in 2009, which prompted widespread adoption of EHRs. 10 In the digital age of health care since HITECH, the physical aspects of illness in the EHR and the collection of clinical information such as medical history, vital signs, laboratory results, and medications are a practice standard.3,4 Psychological conditions (like depression and anxiety and addiction issues) have physiological underpinnings and are more widely recognized as diagnoses in the medical model and EHR. 11 In addition, a variety of validated screenings tools in the EHR can track the progression and severity of psychological symptoms in mood disorders and addiction behaviors (i.e., cigarette smoking, alcohol use).2,12 However, psychosocial care extends beyond mental and behavioral health diagnoses and addiction medicine and is often complicated. 12 Patient screening around emotional and spiritual sources of distress can be more interpretive dimensions of care and hence more difficult to extract utilizing traditional methodology and clinical health informatics.5,8,9,13 When psychosocial interventions are provided, documentation addressing these quality metrics are difficult to monitor and evaluate in the EHR. 5
A systematic approach to capture psychosocial distress has been recommended by several national organizations, including the National Academy of Medicine (formerly the Institute of Medicine) and Centers for Medicare and Medicaid Services.14–16 Guidelines focus on patient-reported data elements around socially complex and diverse needs. Recommendations include the integration of a standardized set of social and behavioral determinants of health. Nevertheless, there is no consensus on consistent methodology across sites, and data are often siloed in different systems and components of the EHR.3,7,14,17,18 Existing evidence-based practice strategies using Patient Reported Outcomes Measurements Information System (PROMIS) in the EHR have been gaining traction and growing rapidly over the past few years.3,19,20 PROMIS are computer adaptive tests and instruments and are considered a gold standard. They are reliable, valid, sensitive to change, feasible, important to clinicians and public health, actionable, user-friendly, and broadly applicable in data management and reporting.6,10,21 Research has increased on tracking social and behavioral drivers of health in the EHR using PROMIS in a variety of general health care4,6,10 and specialty settings including oncology,19–21 primary care, 3 and behavioral health. 7 However, routine clinician documentation and tracking of psychosocial activities, beyond PROMIS, is a large component of psychosocial care delivery. Standardized measurements of psychosocial care and systematic data collection processes are needed to demonstrate high-quality practice metrics in palliative care. 5
In this era of data-driven health care, psychosocial care should be documented consistently alongside medical and clinical data in EHRs. This would reinforce a palliative approach that integrates psychosocial aspects of care into routine and specialized health care.1,22 Incorporating the collection of social needs via quality metrics into clinical informatics harmonizes contextual factors in the EHR, advancing personalized care and fostering clinical decision support within palliative care delivery.1,19,20 More sophisticated EHR tracking mechanisms for psychosocial care are just starting to be explored, offering a tremendously innovative opportunity to operationalize complete care delivery.5,23,24 This narrative review explores existing practices of integrating psychosocial care in EHR documentation through an examination of the literature related to capturing psychosocial dimensions of palliative care through EHR technology.
Methods
Information sources and literature search
EMBASE, PubMed, and PsycINFO databases were queried to identify articles on tracking and data collection of psychosocial care in EHRs within palliative care. Given the novelty and advancement of the research topic, the search was limited to articles published since widespread adoption of EHRs marked by the HITECH Act from 2009 to present. The following search terms were used: (“palliative care” OR “seriously ill patient population” OR “psychosocial care” OR “psychosocial support”) AND (“quality improvement”:ti,ab OR “data collection”:ti,ab OR “quality metrics”:ti,ab) AND (“electronic health record”/exp OR “ehr (electronic health record)”:ti,ab OR “electronic medical record”:ti,ab OR “informatics”).
Study selection
Mixed methods studies, quality improvement projects, and analysis and commentaries were included in the literature review; however, conference abstracts were excluded owing to the lack of robust information and detailed results. Because search terms were quite broad, a few recurring themes were prominent in the initial screening of titles and abstracts that were unrelated to the aims of the review. These were excluded from the review as they did not focus on tracking psychosocial care in EHRs. Excluded articles included those centered around EHR technology for care coordination and communication between providers, modern mobile technology modalities (i.e., iPads, cell phones) rather than the EHR, and targeted digital health interventions. In addition, the literature is saturated with articles that focus on goals of care and advance care planning documentation and reporting processes.25–29 Although these activities could be argued as within scope of psychosocial care in palliative care practice, the purpose of this review was to examine EHR capture of more diverse psychosocial needs and associated nonphysical distress that encompass whole person care models. Articles eligible for analysis that met further inclusion and exclusion criteria are outlined in Table 1.
Inclusion and Exclusion Criteria
EHR, electronic health record; PROMIS, Patient Reported Outcomes Measurements Information System.
One primary reviewer with 15 years of clinical experience in palliative and end-of-life care was involved. Additional palliative care clinicians and researchers and EHR content experts were consulted throughout the review process to reduce bias in the critical appraisal. Each article was reviewed in detail noting similarities and differences in setting and scope as well as study purpose. Themes that emerged included strategy, content of psychosocial documentation, and data collection processes within EHRs.
Results
The search resulted in a total of 143 texts across the 3 databases. EMBASE generated the largest search results with 69 articles, followed by PubMed with 46 articles, and PsycINFO with 28 articles. A hand search of reference pages for related articles resulted in another seven records for review. Duplicate articles were removed (n = 13) and the remaining 137 articles were screened by title and abstract eliminating an additional 102 articles. After a full-text review of these remaining records (n = 35), another 27 articles were excluded upon further examination owing to health care settings outside palliative care, exclusive focus on advance care planning or goals of care activities, or alternative EHR tracking source (i.e., mobile device) or purpose (i.e., interprofessional communication). Eight articles remained and are the subject of this review. See Figure 1 for a PRISMA flow diagram illustrating the search process.
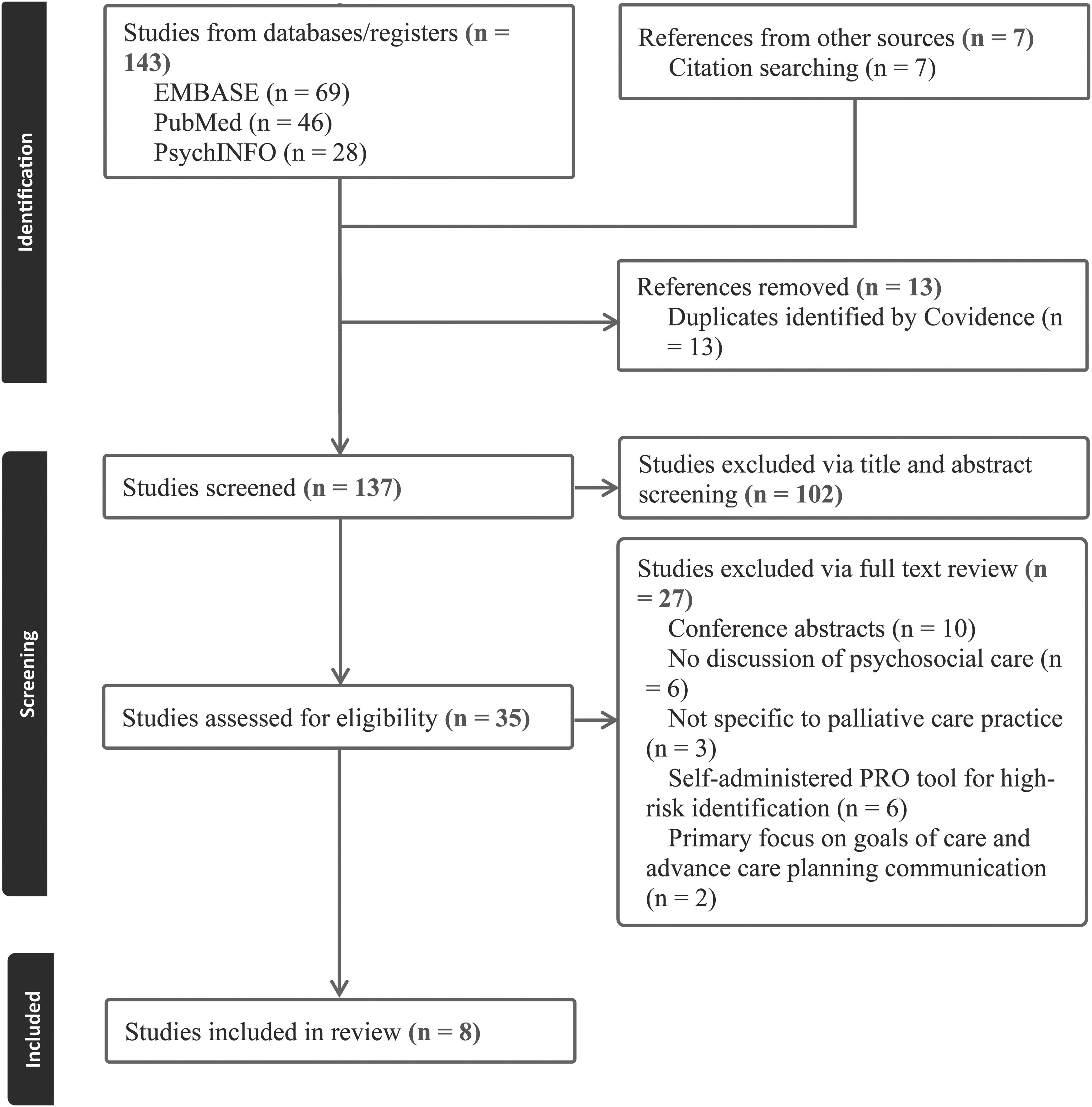
PRISMA chart with selection process of relevant articles.
The eight works analyzed (Table 2) in this narrative review varied in scope including two quality improvement demonstration projects and a single cross-sectional qualitative study, retrospective study, development process, systematic review, description of quality metrics, and “Top Ten Tips” article. Several articles were centered around specific characteristics or areas of palliative care including three distinct subpopulations: pediatric, 30 veterans, 31 and structurally vulnerable patients. 32 The articles also had different focuses with regard to international regions outside the United States including Canada 32 and Japan, 33 as well as, discipline including one study specific to palliative care social work. 5 Three overarching themes related to EHR tracking of psychosocial care in serious illness were apparent in the literature: (a) quality improvement strategy to support EHR tracking in collaboration with key stakeholders, (b) clarification of psychosocial domains for documentation and measurement, and (c) lack of standardization in data collection tools and processes.
Summary of Included Review Articles
NLP, natural language processing; PC-NCT, Palliative Care-National Clinical Template.
Quality improvement strategy to support EHR tracking in collaboration with key stakeholders
The literature proposed leveraging EHR utilization to optimize and report on whole person care in palliative care delivery through a quality improvement framework.23,24,30 This strategy requires consensus among broadly defined stakeholders around the definition and selection of appropriate quality measurements of psychosocial care.23,24,31 The identification of clinical champions and engagement with diverse stakeholders (i.e., clinical informaticists, computer programmers, EHR developers and analysts, and medical researchers) is critical to create consensus on quality metrics. The articles in the review aligned with arguments in other health care settings 10 that only through collaboration among a cross-section of key stakeholders can coordinated action improve individual and population health in the electronic age of health care.24,31
High-quality evidence-based data are needed to determine the effectiveness and impact of psychosocial interventions in addressing social needs and clinical outcomes. Psychosocial members of palliative care teams—which could be inclusive of social work, chaplaincy, pharmacy, navigation, and community health work—address systemic barriers and care disparities, enhance continuity in transitions, and reinforce communication among patients, families, and teams. 5 Although psychosocial support is a critical component of high-quality care, the absence of regulation contributes to variation in scope and care delivery as well as challenges in capturing interventions in the EHR. 23
The assessment and response to social, emotional, and spiritual needs are some of the most difficult domains to execute quality metrics in the care of the seriously ill. 23 Curtis et al. suggested evaluation of psychosocial care quality in terms of patient and family experience, quality of life, spiritual needs, and functional status while noting the lack of systematic assessments must be supplemented with patient and family reports. 23 The EHR has been underutilized in interprofessional palliative care delivery; the optimization of consistent patient-reported data elements around socially complex and challenging patient needs would promote quality improvement and more robust psychosocial research methodology. 13
Clarification of psychosocial domains for documentation and measurement
The literature reviewed demonstrates the variations in what palliative care researchers designate as psychosocial domains and meaningful for documentation and measurement in the EHR. Many studies have focused on advance care planning metrics, including documented goals of care discussion, identification of a surrogate decision-maker/health care representative, and presence of advanced directives in the chart or Physician Orders for Life Sustaining Treatment forms.13,23,24,34 However, psychosocial care extends beyond advance care planning activities in palliative care practice. Core psychosocial elements of palliative care encompass nonpain physical symptoms, emotional well-being, caregiving and social context, existential well-being, and communication, which can guide the clinical content of new informatics tools. 31
All eight articles included in the review highlight the importance of documenting psychosocial care through the lens of patient and family experience and health-related quality of life.5,13,23,24,30–33 The articles elicit a variety of terms to describe psychosocial care that add to the challenges in consistent tracking across EHRs within palliative care delivery.5,30–33 More specifically, several studies examine the presence of assessment and intervention of social, psychological, and spiritual aspects of care to document psychosocial domains.5,30,33 Although all these appear somewhat similar, the studies measured these psychosocial elements in slightly different detail or through related issues. For example, Christophel Lichti and Cagle study noted social care through safety concerns, financial and insurance needs, caregiver resources, and practical assistance and referral. 5
Goebel et al. documented social history through caregiving needs and military history, 31 whereas Masukawa et al. focused on social distress defined by economic issues, work and social roles, and family matters and relationships with others. 33 Some studies tracked psychological symptoms of anxiety exclusively, 20 whereas others included depression as well. 31 Measurements of spirituality also varied significantly among the queried articles. Some articles focused on the assessment of “spiritual pain,” 33 whereas others defined spiritual interventions as honoring cultural-specific needs, meaning-making and legacy counseling, or chaplaincy referral. 5 These differences demonstrate the ongoing controversy of how psychosocial care is defined and what is significant to measure in the EHR.
Although there is discrepancy among the articles in the specific elements of palliative care to prioritize and measure in the EHR, four categories of psychosocial palliative care emerged in the literature review: social history and distress,23,30–32 psychological symptoms,31,33 spiritual needs,23,31–33 and patients' goals and preferences.5,13,23,31 These domains provide an EHR design to structure components of psychosocial care and optimize use for tracking, data collection and research, and automated reporting. Defining a concrete psychosocial framework elicits more comprehensive measurement and benchmarking data and would prompt more valid, reliable, and complete collection of psychosocial metrics. 23
Lack of standardization in data collection tools and processes
The literature highlights the variety of clinical informatics tools available and used in EHRs. Both structured and unstructured data sources are used to collect information on psychosocial domains. The spectrum of EHR utilization highlights the idiosyncrasies in data on care delivery, billing, communication, and quality improvement. 23 Traditionally, EHR data from diagnostic codes, scheduling or consultation orders, symptom scores, and clinical events offer robust information on the trajectory of care and can prompt patient “flags” to identify high-risk patients.13,24 In addition to targeting physical signs and symptoms, similar EHR screening mechanisms could distinguish socially complex patients who may benefit from further psychosocial intervention through palliative care support.13,24
Clinic workflow and technology integration do not always coalesce. Thus, the EHR reflects only the care extracted from documentation, not necessarily the complete, whole person care provided. 23 The narrative nature of biopsychosocial assessment limits standardization and makes it particularly challenging to aggregate. This review illustrates the range of systematic data collection processes used including constructed flowsheets 5 and clinical narrative templates 31 as well as variation in reporting from using simple binary variables to indicate the presence of a psychosocial assessment and intervention 30 to more complex free-text format analysis. 33
The EHR is widely text based, creating challenges in accessibility of unstructured text data to aggregate reports on both patient care and patterns in population health management. 33 Narrative documentation templates are often used in biopsychosocial assessment and intervention. But they are difficult to quantify and evaluate for systematic identification of needs, demonstration of impact, and quality improvement. 5 Word recognition software and natural language processing (NLP), a branch of artificial intelligence, utilize computer science to interpret language from unstructured clinical notes.23,24,33 NLP algorithms have been used primarily to detect physical symptoms as a mechanism to identify patients who may warrant palliative care referral and intervention or indicate key metrics like goals of care and advance care planning documentation.23,24
However, the use of NLP technology has seldom been explored in pinpointing psychosocial factors and risk in palliative care practice. 33 Masukawa et al. utilized machine learning models based on NLP to accurately detect and analyze psychosocial content in EHR free text. The authors reviewed >1.5 million narrative clinical records and found 1.6% had documented social distress, 6.7% spiritual pain, and 8.1% anxiety; however, the severity of distress could not be distinguished. 33 The extraction of meaningful information and increasingly more complex constructs in EHR notes has aided in functionality for comprehensive distress and risk stratification. 33
In addition to mining text-embedded information, psychosocial information can be transformed into discrete elements in clinical narrative notes and automatically populated into reports via customizable templates, checklists, flowsheets, chart modules, and “smart” tools for data measurement and recording.13,23,24 National guidelines and clinical practice mandates have recommended specialty-specific psychosocial and distress measurement tools (i.e., National Comprehensive Cancer Network distress thermometer and Functional Assessment of Cancer Therapy). 24 Leveraging patient and family-reported data through these PROMIS tools create more comprehensive patient assessment and can then be merged into usable, customized flowsheets in the EHR and reporting dashboards. 24
Some practices collect and record social factors via health care professionals assessment and interview as part of routine workflow within their internal system, whereas others optimize local and national registries that offer a vessel of information for robust reporting on quality metrics and benchmarking. 24 Because social and behavioral data are stored in a variety of internal and external sources across a multitude of settings (i.e., home, clinic, community), it complicates the utility, workflow, and unification of data.
Discussion
This narrative review article expands on the body of literature on clinical informatics and palliative care. There is minimal knowledge and nominal published works specific to EHR assessment and interventions in the discourse of psychosocial care for seriously ill patients. EHR tracking metrics and procedures must be conducted systematically. 24 Best practices in documentation is a quality improvement initiative that requires consensus, collaboration, and support from key stakeholders.10,24
Defining what constitutes psychosocial care through quality metrics is a first step in establishing specific priorities for measurement.24,31 Palliative care quality metrics were originally formulated in the Clinical Practice Guidelines for Quality Palliative Care with the National Consensus Project in 2004. 35 They have continued to evolve to further define clinical domains of care and the establish best practices through the Measuring What Matters (MWM) project. 36 The Quality Data Collection Tool is a data entry system of 10 MWM indicators; however, documentation has been less consistent in the assessments, interventions, and outcomes around patients' emotional needs and spiritual concerns.37,38 This review discussed multiple methodologies in meaningful data collection including PROMIS, extraction of information within narrative notes, and external data sources.5,13,24,30,31,33
Strengths and weaknesses
Optimizing EHR tools and technology to showcase psychosocial impact is progressive and innovative, highlighting an under-researched area and outlining gaps in the existing literature. The limitations of this review centered around the small number of studies available as well as the variety of genres analyzed. There was a lack of quantitative studies for this narrative review as most of the texts were quality improvement and demonstration projects or tool development process articles. At the same time, the breadth of settings (i.e., veteran and structurally vulnerable populations) and scope (i.e., clinical decision support) represented in the emerging literature tackle the subject with greater vigor through more dynamic approaches and perspectives. Because the level of evidence is not strong and this was not a systematic review, there is a risk for bias in the article selection process.
The author and consulting reviewers are experts in the field with a solid knowledge base in the intersection of psychosocial practice and palliative care. The author and consultants' proficiency thus makes them skilled in identifying relevant content for the purpose and aims of this narrative review.
Implications for practice
In the shift from a disease to person-centric lens in health care, palliative care teams should lead efforts to capture social history, health behaviors, and patient-reported goals, values, and preferences. 1 Data analytic insights inform action and contribute to more effective supportive care management, service coordination, and resource allocation. More specifically, the identification of patient burdens and barriers to care shapes clinical decision-making and care planning tailored to patient needs and aligned with patient priorities.3,7 An informed approach to the provision of health and social resources guides caseload modeling and capacity planning and subsequently directs psychosocial resource and personnel requests.3,7,24
Stratifying risk burden and quantifying psychosocial interventions ultimately justifies the presence and professional value of traditionally nonbillable team members in minority disciplines (i.e., social work, chaplaincy) on interprofessional palliative care teams.5,8,9 Evidence-based research has begun to distinguish the unique contributions and clinical competencies of specialty practice, driven from advanced skills in facilitating the emotional and existential processing, meaning-making, and adaption to serious illness.5,8,9,39 EHR documentation reflects the nuances of this specialty psychosocial work in the palliative care clinical context. Enhancing visibility and communication around psychosocial needs in the EHR ultimately leverages the value of psychosocial care while advancing efficiencies in care management and comprehensive patient and family support. 5
Future research
It remains challenging to quantify psychosocial care and interventions through nonbillable touchpoints in the EHR. Care transformation must be coupled with evidence-based strategies and merge clinical practice with research. This review highlights potential opportunities in EHR technology and clinical informatics in expanding and enhancing quality metrics that guide goal-concordant care. The designation of four domains of psychosocial palliative care (social history and distress, psychological symptoms, spiritual needs, and patients' goals and preferences) set a foundation for EHR design and tracking in palliative care settings.5,13,23,30–33
Future research should align these domains with quality metrics within a psychosocial framework in palliative care. This would involve the refinement of more targeted best practices. For example, the interpretation of medical language and culture to clarify treatment options, tailored counseling theories and approaches, cultivation of prognostic awareness through targeted questions, leading anticipatory guidance in advance care plans, and optimization of quality of life through resource connections. These data would provide more aggregated reports with granular detail around palliative psychosocial care and contribute to an analysis of trends in acute care utilization when specific interventions are utilized.5,39 In addition to the technological development in EHRs, education and training is needed for palliative care clinicians to learn how to document psychosocial care in measurable ways and use the EHRs to their greatest potential.
Data to support the return on investment are critical and needed now for interprofessional palliative care program sustainability and growth. Clinical analytics that highlight the nonmonetary value and impact of social care would provide both data-based and narrative impact analysis. Nonmedical psychosocial interventions are typically not billable in fee-for-service models thus prompting the greater need to demonstrate value impact in the care of the seriously ill. Interventions that address risk factors related to social and behavioral needs in conjunction with reimbursement incentives can improve individual health outcomes and manage population health. 7 More rigorous research is needed to evaluate care delivery and reductions in health care costs to promote value-based care models.
Conclusion
This narrative review examined the existing literature on EHR tracking of psychosocial care within palliative care practice including the psychosocial domains of measurement, data collection tools and processes, and opportunities for quality improvement in partnership with key stakeholders. EHR utilization for the purpose of identifying high-risk patients for palliative care referral and primary focus on goals of care and advance care planning activities is not sufficient. There is growing interest and rapid advancements in EHR technology. Considering the importance of and attention to psychosocial factors in palliative care practice, enhancing quality metrics to establish and reflect comprehensive psychosocial care through data-driven EHR tools is imperative in the changing face of health care in the electronic age.
Funding Information
No funding was received for this article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.