
Abstract
Background:
Despite their essential role in language concordant patient care, medical interpreters do not routinely receive training focused on difficult conversations and may not feel comfortable interpreting these encounters. Previous studies, while acknowledging the need for increased support, have provided limited strategies targeted at enhancing interpreter training and improving interpreter comfort levels in difficult conversations.
Methods:
Fifty-seven in-person medical interpreters providing services at our quaternary and community hospitals completed a 21-question mixed-methods survey regarding their comfort levels and experiences surrounding serious illness conversations.
Results:
Most medical interpreters reported being uncomfortable interpreting conversations surrounding difficult diagnosis, poor prognosis, and/or end-of-life. Nearly all respondents (98%) indicated that pre-meetings and/or debriefings with the medical team are helpful, yet only 25% reported frequent participation in these meetings.
Conclusions:
Our study highlighted the significant variability in medical interpreter training as well as ranging comfort levels in interpreting difficult conversations. Medical providers should not presume that interpreters are instantly prepared for these encounters. Current findings call for novel training opportunities specific to medical interpreters and difficult dialogues, as well as improved adherence of interprofessional pre-meeting/debriefings when serious news is discussed.
Introduction
Medical interpreters are essential in language discordant medical interactions, ensuring clear communication for the patient and their support system surrounding diagnosis, prognosis, and options for treatment. 1 Furthermore, working in collaboration with interpreters positively impacts clinical care for patients with limited English proficiency (LEP)2–5 while also addressing and reducing health disparities related to language barriers.6,7 Despite medical interpreters’ important responsibility in patient care, significant variability exists in their training on serious illness conversations.2,8,9 There is an acknowledged need for increased support for medical interpreters as likely best practice with limited supporting data.10–13
Methods
Participants
Individuals employed by or contracted to provide in-person medical interpreter services at a large, urban, quaternary hospital or one of its three community affiliate hospitals within the Greater Philadelphia area were invited to participate. To maintain subject anonymity all communication was directed to previously identified managers of eligible participants. Emails were sent to n = 342 interpreters, participation was voluntary, and responses were anonymous; 57 participants consented and completed the survey (Fig. 1), which was exempted by the IRB at the investigator’s University.
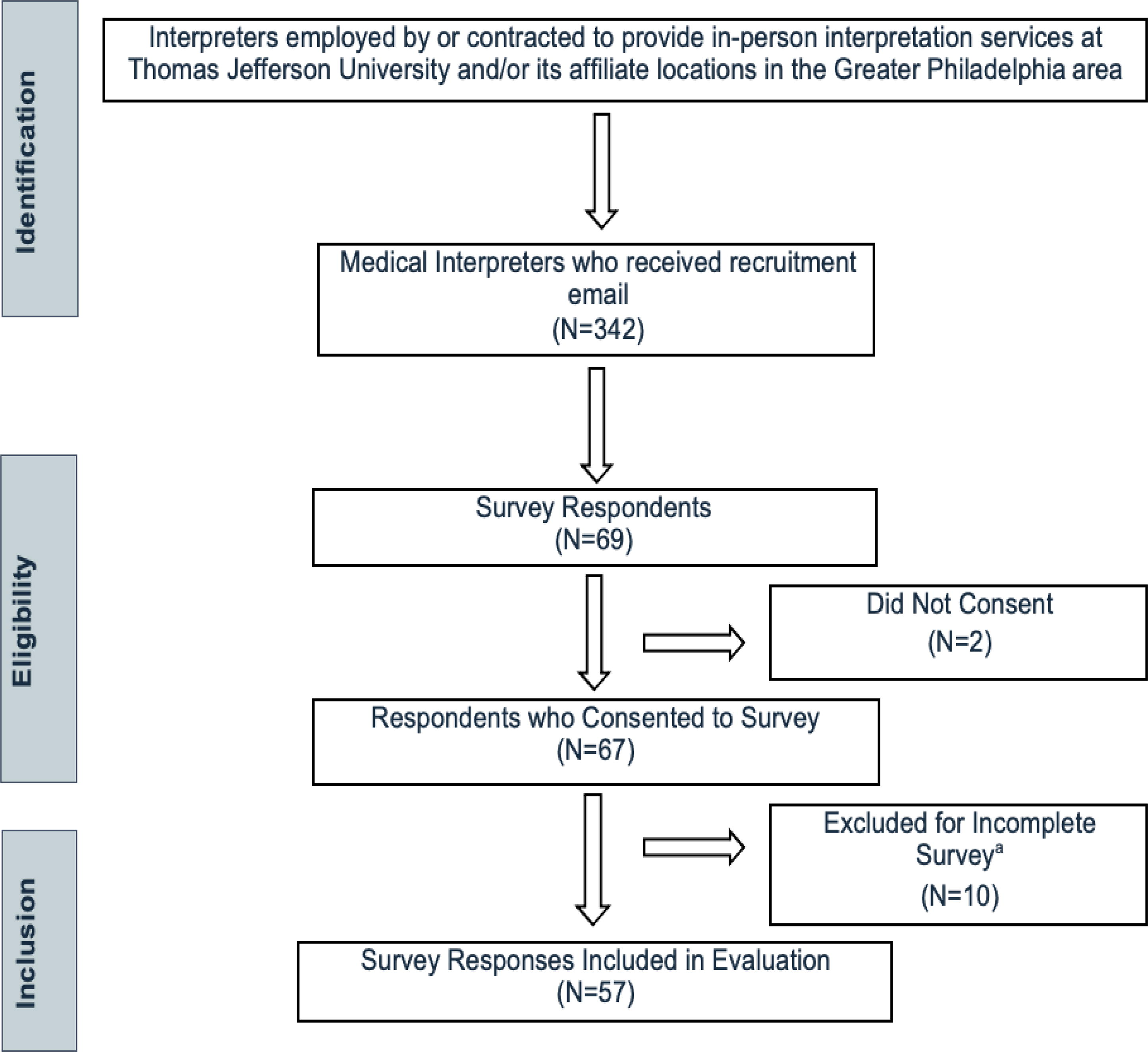
Flow chart of identification, eligibility, inclusion, and exclusiona criteria. aInvestigators recognized that the nature of the subject matter may be distressing to some, and respondents were instructed, before consenting, to skip any open-ended questions that they did not wish to answer. Resultant of that disclaimer, responses were only deemed “incomplete” if respondents chose to answer only demographic information within the survey.
Survey development, measures, and coding
A 21-item, cross-sectional mixed-methods online survey (Qualtrics, Provo, UT) was developed with input from hospital-employed interpreter leadership to ensure that questions were clear and representative of the background and skillset of interpreters within our system, and included Likert, yes/no, and open-ended responses (Supplementary Data S1). Question topics included demographics, education/training, familiarity with the specialty of palliative care (PC), and experiences and comfort levels in interpreting difficult conversations. Difficult conversations (DC) were defined as delivering serious news such as: a diagnosis, discussing poor prognosis, talking about goals of care, and/or end of life.
Analysis
Results were analyzed based on the four previously identified categories (demographics, education/training, familiarity with PC, experiences and comfortability with interpreting difficult conversations). Data were exported for frequency analysis, and relative frequency was reported. Statistical software included within the Qualtrics platform was used for further analysis of qualitative data including correlation and regression analysis. A ranked ANOVA was performed to examine relationships between the different variables. A chi-square test was performed to examine the relationships between years of employment and familiarity with PC and years of employment and comfort levels interpreting difficult conversations.
To control for the inevitable variability in open-ended responses, investigators conducted a thematic analysis of qualitative responses. 14 Inductive coding techniques aided in identifying themes present in responses to three open-ended questions. Once the themes were identified, three raters separately evaluated each response, categorizing each response based on their overarching theme. Multiple rounds of data coding and open discussion were conducted to address discrepancies and reach intercoder consensus (Supplementary Data S2). Key qualitative responses are referenced in this report to support quantitative findings. Further comprehensive analysis of qualitative results is ongoing and will be reported in subsequent work.
Results
Demographic information
Respondents (n = 57) were predominately female (82.1%), 79% were 45 years or older, and 72% have interpreted for >10 years. Seventeen interpreted languages were represented with 23% of interpreters interpreting more than one language; the most common languages interpreted were American Sign Language, Spanish, and Korean (Table 1).
Characteristics of Participants (n = 57)
Education and training
Significant variability exists in the education and training received by medical interpreters. A mere 16% of respondents sought certification at the national level 15 following initial training, while 19% did not complete and/or receive formalized training as defined by the National Council on Interpreting in Health Care 17 —reporting only language proficiency and/or on the job training. The most common training program completed was a 40-hour training course.
Most respondents (88%) received continuing education (CE) following initial training. CE was broadly classified, and only 43% completed CE specific to interpreting difficult news, end-of-life, and/or PC within their careers.
Familiarity with palliative care
Self-reported familiarity with the specialty of PC was high with 53% reporting being “extremely” or “very” familiar with PC. Increased time as a medical interpreter was correlated with increased familiarity, but the type of training received was not.
Experiences with interpreting difficult conversations
Only 18% of respondents indicated extreme comfortability in interpreting DC; 39% reported being neutral or uncomfortable in these encounters. Despite varying comfort levels, interpreters are frequently involved in DC with only 15% of respondents indicating rare or infrequent participation in this encounter type. Increased frequency of involvement in DC was significantly correlated with higher comfort levels. Self-reported comfort was not influenced by type of training received, participation in specific CE training, or time spent as a medical interpreter.
In assessing how the medical team can better support interpreters in these encounters, nearly all participants (98%) indicated that pre-meetings and/or debriefings are helpful, though only 25% reported frequent participation in these meetings. More frequent participation in pre-meetings was significantly associated with higher comfort levels in interpreting DC. Themes on how to improve interpreter experience included: information sharing (36%); cultural awareness (12%); allowing for processing of information (10%); improving accuracy of interpretation/aiding the interpretation process (7.3%); sharing medical terminology in advance of the encounter (7.3%).
Discussion
As the population of LEP individuals in the United States continues to rise,16,17 it is of pressing urgency for health care professionals to examine ways to provide language-concordant care. Collaboration with medical interpreters is both necessary and beneficial in providing quality care, particularly in conversations discussing serious news. While a growing body of literature, in addition to expert consensus, supports inclusion of medical interpreters in pre-meetings/huddles,8–13 these inclusion practices were not reflective in our experiences as in-patient PC consultants in an urban academic setting. This study explored in-person medical interpreter training, interpreter attitudes towards DC, and how to best support and improve interpreter interactions with health care teams.
Our results highlighted the variability in medical interpreter training. Of the 57 respondents, 24% had not received training specific to PC or DC. Requirements for qualified medical interpreters for spoken language, as set forth by the National Council on Interpreting in Health Care (NCIHC), are to complete a minimum of 40 hours of training and achieve competency in six areas: basic language skills, code of ethics, cultural issues, health care terminology skills, integrated interpreting skills, and translation of simple instructions. 18 Given the short duration of these courses and the vast amount of knowledge needing to be covered, interpreters-in-training may not receive education on PC or how to best prepare for DC leaving their exposure to be in real time, on the job. Additionally, CE beyond one’s initial training is only a requirement for certified interpreters, those who have completed additional training at the national level. However, certification requires additional time and cost and may not be required as minimums are often employer and/or state dependent.15,18
Disappointingly, completion of CE specific to PC in this sample was insufficient in significantly improving self-reported comfort with DC, though results are limited by small sample size. Results highlighted that frequent involvement/exposure is the strongest factor influencing one’s comfort. This supports previous studies involving role-play and case-based scenarios with interprofessional team members as likely having the greatest impact. 4 Our results also confirmed the importance of holding space for reflection and increased time for and education in self-compassion practices.12,19
When taking into consideration the non-response bias inherent in the survey’s design and that most respondents had over 10 years of work experience, the true measure of medical interpreters’ discomfort interpreting DC is likely higher than our findings. Cognizant of this, we suggest that medical teams not assume that an interpreter is prepared, professionally, or emotionally, to immediately interpret serious news.
Despite decades of mounting evidence for inclusionary practices and information exchange before patient encounters only 25% of interpreters are frequently or always included in these meetings at our teaching hospitals. Selected responses highlight this discrepancy:
“99% of the time Interpreters are learning the news as a medical team member is delivering it to the patient.”
“Many of the difficult assignments that I have had say ‘follow-up appt’ so it is easy to think it could be a simple assignment rather than ‘follow up appt after surgery to discuss terminal diagnosis.’”
Including medical interpreters in pre-meetings/huddles or debriefings has been recognized as a best practice19–24 and is confirmed in this survey to be not just helpful but correlated with higher comfort surrounding DC. Reevaluation of current medical team practices to ensure that these meetings standard practice holds promise as a significant opportunity, not only for improved communication, but for enhanced, supportive interprofessional collaboration and learning.
Limitations
Limitations of this study include a small response rate (20%) and a likely high non-response bias given the emotional topic and use of open-ended questions. This survey only assessed the attitudes of those providing in-person interpretation services, and therefore our results are not representative of interpreters who provide telephone or video services. Although we did not use a validated instrument in this pilot study, our survey questions were developed through consultation with literature and experts in the field.
Conclusions
Our results suggest that medical interpreters remain interested in further training on difficult conversations and PC topics, further supporting the time-sensitive need for implementation of curricular changes in interpreter education as well as medical team best practices. Despite frequent reliance of medical teams on interpreters for difficult conversations, our study reveals that only frequency of conversation positively influences one’s comfort in these conversations. Access to curriculum that can educate on PC topics and mimic the effect of frequency is needed. Future directions include development of novel interpreter-focused curriculum on difficult conversations, and development of a peer support system for local interpreter reflection and wellness. Furthermore, targeted trainings for house staff can address the gaps in medical provider education on best practices in interpreter utilization, and highlight the importance of formal pre-meetings/debriefings between the care team/interpreter before serious illness conversations.
Footnotes
Acknowledgments
The authors wish to express their appreciation to the medical interpreters who assisted in the development of this survey as well as all who participated in the survey. The authors would especially like to thank the Chinese Health Information Center at Thomas Jefferson University for their time, expertise, and commitment to our patients and their support system.
Authors’ Contributions
All authors made significant contributions to this article. K.W. conceptualization. K.W. & K.M. research and investigation, data curation and analysis, and original draft preparation. A.C. reviewing and editing.
Funding Information
This study did not receive any financial support.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.