
Abstract
Background and Objectives:
Spiritual care is an essential component of care for the terminally ill, because of its potential to positively impact patient perception of quality of life and dignity. However, it continues to be the least cultivated or even most overlooked aspect of palliative care and end of life. We performed a methodological review using bibliometric analysis to provide a holistic view of the scientific output published on this topic in the literature at the same time outlining present perspectives and research trends.
Methods:
In accordance with the BIBLIO checklist for reporting the bibliometric reviews of the biomedical literature, pertinent articles were retrieved from the Web of Science (WOS) database. The search string included “spiritual care,” “end of life,” and their synonyms. The VOSviewer (version 1.6.17) software was used to conduct comprehensive analyses. Semantic and research networks, bibliographic coupling, and journal analysis were examined.
Results:
A total of 924 articles were identified in WOS, and 842 were retrieved. An increasing trend in the number of publications is observed from 1981 to date, with a peak in the 2019–2021 timeframe. Most articles focused on palliative care, spirituality, spiritual care, religion, end of life, and cancer. The Journal of Pain and Symptom Management contributed the highest number of published documents, while the Journal of Palliative Medicine was the top-cited journal. The highest number of publications originated from collaborations of authors from the United Kingdom, the United States, and Australia.
Conclusion:
The remarkable increase in the number of publications on spiritual care observed in the years of the COVID-19 pandemic likely reflected global concerns, reasserting the importance of prioritizing spiritual care for whole-person palliation. Spiritual care is integrated with palliative care, in line with the latter’s holistic nature and the recognition of spirituality as a fundamental aspect of end-of-life care. Nurses and chaplains exhibited more involvement in palliative–spiritual care than physicians reflecting the belief that chaplains are perceived as specialized providers, and nurses, owing to their direct exposure to spiritual suffering and ethos, are deemed suitable for providing spiritual care.
Introduction
Terminal illness encompasses a myriad of experiences for patients, spanning physical symptoms (e.g., dyspnea, nausea), emotional challenges (e.g., depression), social isolation, and spiritual distress (e.g., deep inner questioning, death anxiety). These threaten to undermine the sense of meaning and value of life, as well as reduce quality of life (QoL) and dignity. 1 Therefore, the spiritual domain within the holistic biopsychosocial–spiritual framework is increasingly relevant for both individuals nearing the end of life (EoL) and those facing terminal illness. This relevance arises from the tripartite nature of humans, wherein health is the state of equilibrium and unity of the interconnected elements, which can be visualized as three “concentric circles.” The central circle represents the spirit, which enables connection to the Divine. The middle circle represents the soul, traditionally defined as the mind, will, and emotions. The outer circle represents the body, the material factor. These three circles collectively constitute and shape the entirety of an individual, and conversely, disease signifies an absence of this equilibrium and harmony.2–4 Spirituality, defined as an inherent and dynamic aspect of human nature, synthetizes how individuals explore and articulate meaning, purpose, and transcendence. Frequently intertwined with a sense of unity with the present, oneself, community, society, nature, and the profound or sacred, spirituality finds expression through beliefs, values, traditions, and habitual practices. 5
Likewise, spiritual care is an essential and intrinsic element of palliative care, pivotal in Dame Cicely Saunders’ conceptualization, and acknowledged and integrated into the World Health Organization’s (WHO) definition of palliative care for nearly two decades. Unmet spiritual concerns or needs may exacerbate distress for individuals at EoL, resulting in additional physical and emotional suffering.6,7 Therefore, the main goals of palliative care include enhancing the QoL for terminally ill patients, ensuring a peaceful and dignified death, and addressing not only physical suffering but also attending to their psychological and spiritual needs throughout their EoL journey. This is achieved through early identification, thorough evaluation, and management of the “multifaceted” aspects of their suffering.8,9
Remarkably, growing evidence underscores the significance of spiritual care in EoL scenarios, unveiling patients’ strong desire for health care practitioners to provide this type of care. 10 Similarly, multiple studies have highlighted the favorable impact of spiritual care on the QoL of diverse patient populations, spanning various age groups and medical conditions.11–13 Conversely, inadequate spiritual support from health care teams has been linked to adverse outcomes (i.e., diminished QoL, discontentment with care, reduced utilization of hospice services, escalated usage of aggressive treatments, and increased health care costs) being particularly pronounced among ethnic minority groups and patients exhibiting high levels of religiousness.14,15
Various initiatives have recently emerged to foster the integration of the spiritual aspect of palliative care into both research and clinical practice. These include the establishment of a Spiritual Care Taskforce by members of the European Association for Palliative Care, the formation of the Global Network for Spirituality and Health, and the initiatives led by the International Society for Health and Spirituality in the United States and Germany, respectively. Moreover, there have been efforts to develop training resources aimed at enhancing the spiritual care skills of health care professionals within the UK National Health System.16,17 Despite the emerging evidence recognizing its significance as a fundamental aspect of palliative care, spiritual care is still the most overlooked dimension within this domain.18,19
Although meta-analyses provide robust evidence by summarizing results from multiple studies, randomized controlled trials (RCTs) show cause and effect relationships, and systematic reviews give a comprehensive overview of all available evidence, bibliometrics involve using statistical methods to assess large quantities of bibliometric data from global scientific outputs from the perspective of their intellectual structure. 20 Aided by the results of the analysis of multiple studies on a specific subject, researchers can efficiently survey a vast body of literature, summarizing insights from thousands of articles in a short time. Given the undeniably crucial role held by research in laying the foundation for treatment decisions and considering the escalating publication volume, a rise in the number of studies based on statistical and bibliometric analysis across various important medical issues has recently been observed.21–23 To date, a bibliometric study of the growing body of published literature on the role of spiritual care in palliative medicine and EoL is yet to be performed.
Hence, this methodological review holds two primary aims. First, to delineate contemporary perspectives on spiritual care in palliative care and EoL by providing a bibliometric network analysis of existing published research and emerging trends in the field and identifying the most influential researchers, authors, journals, institutions, and countries. Second, to unveil cross-national collaborations and collaborative authorship networks, intending to stimulate further research endeavors in this area.
Materials and Methods
Data collection
The research follows the methodology described in existing bibliometric studies published previously24,25 and was conducted according to the BIBLIO checklist for reporting the bibliometric reviews of the biomedical literature (Supplementary Table S1). 26 The Web of Science (WOS, www-webofscience-com.web.bisu.edu.cn) online database—a bibliographic database of scholarly articles encompassing over 22,000 peer-reviewed journals worldwide—was used to conduct a comprehensive literature review on the role of spiritual care in palliative medicine and the EoL. Pertinent documents were retrieved using a search string that included terms such as “spiritual,” “pastoral,” “religious,” “dignity,” “existential,” and “palliative,” “terminal,” “end of life,” and “care.” The Boolean operators “OR” and “AND” were used as conjunctions to combine the abovementioned search terms and free words resulting in enhanced search precision. No restrictions on either language or year of publication were imposed. All data were accessed on November 22, 2023, and exported as a Microsoft Excel (.xlsx) worksheet. Both literature retrieval and data download were carried out on a single day.
Research methods
The search results were independently screened for potential eligibility at title/abstract level by two trained and experienced investigators (R.L. and J.D.U.). The final selection of retrieved studies was made following careful assessment of complete articles. When disagreement occurred, it was resolved by means of discussion under the supervision of a third senior investigator (F.M.).
Pertinent information fulfilling research requirements was extracted from the retrieved documents, encompassing details such as year of publication, journal information (including impact factor and quartile), title, authors, topics categorized according to WOS (assigned at the journal level and comprising ∼250 subject categories to reflect disciplinary differences that may exist among individual articles published in the same journal), keywords, and total number of citations. Journal Citation ReportsTM 2022 (Clarivate Analytics) served as the source for journal metrics.
The annual publication trend was manually calculated using a Microsoft Excel exported worksheet. For a comprehensive literature analysis and visualization of knowledge on the subject to be performed, the VOSviewer (version 1.6.17) software was used. A variety of aspects of the retrieved articles were analyzed, aiming to conduct a detailed exploration and visualization of the topic aided by bibliometrics. The aspects examined included:
Co-occurrence of keywords, which involved assessing potential connections or relationships (interconnection), using a co-occurrence or semantic network.
27
Co-citation, often known as “bibliographic coupling.” It quantified how frequently two documents were cited jointly by other works. This analysis used both the “source” (journal) and “author” as units of analysis to determine these relationships.
28
Co-authorship analysis (by countries), aiming to assess the collaborative publishing efforts in publishing among different institutions and nations. Furthermore, an additional analysis was performed to dissect the most productive organizations and explore their collaborations.
Table 1 presents a comprehensive glossary providing detailed explanations of the terminology relevant to bibliometric network analyses.
Glossary of the Terminology Relevant to Bibliometric Network Analyses (on the Left) with the Corresponding Explanation (on the Right)
Results
Our search strategy on the online WOS database from inception to November 22, 2023, resulted in a total of 924 documents. The identification, screening, and inclusion process of the studies is outlined in Figure 1. Out of the total number of documents yielded by our online search, 82 were deemed irrelevant to the research topic and were excluded. A total of 842 documents were retrieved and included in the present bibliometric network analysis.
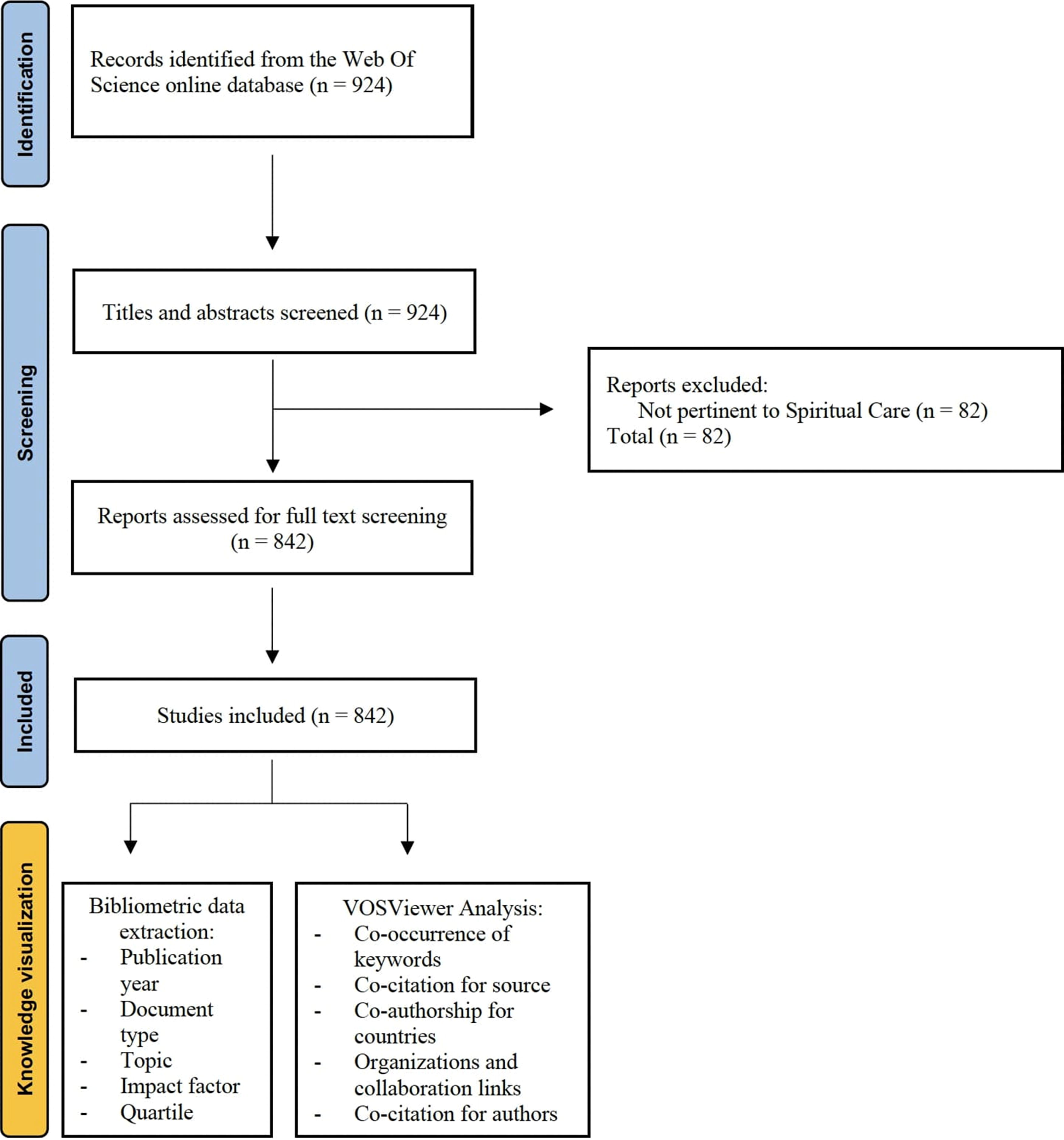
Flowchart of the study selection process.
Bibliometric analysis of publication output
Figure 2 summarizes the trend in the annual number of publications primarily focusing on the role of spiritual care in palliative medicine and the EoL. Starting from 1981, the year of the initial publication in this domain, a consistent upward trend is evident, reaching a peak in the 2019–2020 period. However, a decline in newly published documents emerged between 2020 and 2023, leading to an almost 50% reduction in the total number of published articles from n = 93 in 2020 to n = 57 in 2023.

Annual trend of published articles.
Journal metrics are summarized in Table 2, highlighting the top 10 most productive journals. Notably, the Journal of Pain and Symptom Management (2022 impact factor: 4.7) contributed the highest number of published documents, accounting for 87/842 (10.3%) of the total. Interestingly, most articles were published in high-ranked journals with approximately three-quarters of them being published by Q1 and Q2 journals. This may indicate that spiritual care is a topic of interest in the realm of palliative medicine research.
Top 10 Most Productive Journals and Metrics
Source: Journal Citation ReportsTM 2022.
In terms of the topics covered in each of the retrieved articles, the prevalence of various subjects based on the WOS database is summarized in Figure 3. The majority of articles revolved around healthcare science services (26%), followed by general internal medicine (12%), health policy services (11%), and nursing (11%).

Topics. One or more topics were recorded for each article.
Analysis of author cooperation network
An analysis of the author cooperation network was conducted to evaluate collaborative relationships among authors within the domain of spiritual care in palliative medicine and EoL. This involved identifying patterns of co-authorship, quantifying the extent of collaboration and co-citation, and analyzing the structure and dynamics of the network formed by authors and their collaborative ties. The aim was to elucidate knowledge dissemination and interdisciplinary collaboration within this field.
Bibliometric analysis of the keywords
This analysis focused on keywords provided by authors that appeared more than 5 times in the WOS core database. Out of 996 keywords, 69 met the abovementioned threshold, forming 9 clusters or “communities”—sets of closely related nodes. The most frequent keywords were “PALLIATIVE CARE” (appearing 288 times with a total link strength of 667), “SPIRITUALITY” (237/558), “SPIRITUAL CARE” (120/268), “RELIGION” (62/178), “END OF LIFE” (63/172), and “CANCER” (52/143) (Fig. 4).

Co-occurrence of keywords. The size of nodes indicates the frequency of occurrence. The curves between the nodes represent their co-occurrence in the same publication. The shorter the distance between two nodes, the larger the number of co-occurrence of the two keywords. The analysis provided 996 keywords, of which 69 met the threshold (5 items) and 9 clusters were obtained (different colors).
Co-citation analysis for sources (journals)
A descriptive analysis of the top 10 co-cited articles is presented in Table 3,7,19,29–36 with the most cited article (n = 829) being written by Puchalski et al. in 2009. 29 In our co-citation study, we used cited sources (i.e., journals) as the unit of analysis, setting a minimum citation threshold of 60. Out of 6417 sources, 54 met the threshold. For each of these 54 sources, the total strength of the co-citation links with other sources was calculated as well. The Journal of Palliative Medicine obtained 1052 citations and 23,896 links; Journal of Pain and Symptom Management had 985 citations and 22,847 links; and Palliative Medicine exhibited 726 citations and 18,335 links (Fig. 5).

Co-citation analysis for sources.
Top 10 Co-cited Articles
Co-authorship analysis (countries)
The co-authorship analysis was performed using a minimum threshold of 10 documents with the first author from a specific country. Among 70 countries analyzed, 22 met this criterion. England contributed 72 published documents with 81 links, the United States had 369 documents and 58 links, while Australia accounted for 59 documents and 55 links in our analysis (Fig. 6).
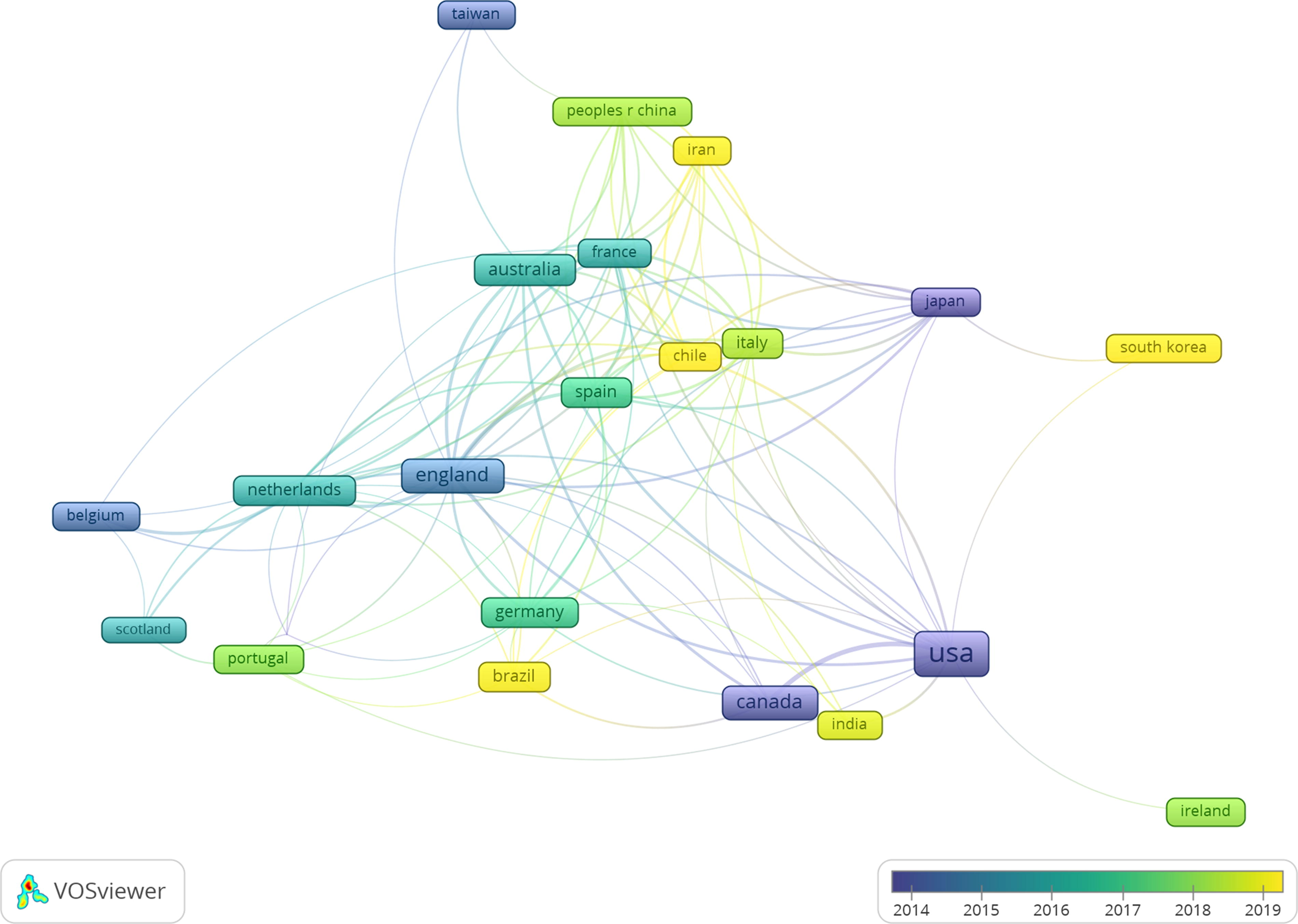
Co-authorship analysis for countries. Four countries reached the threshold of 10 documents. Clusters are organized based on year intervals.
The most productive organizations and their collaborations
We set a threshold of 10 as the minimum number of documents for affiliations (organizations). Out of 1295 organizations, 18 met such criterion. The total strength of citation links with other organizations was calculated for each of these 18 organizations. Notably, the Dana-Farber Cancer Institute (Boston, MA) produced 20 documents with a total link strength of 5927; Rush University (Chicago, IL) published 25 documents and had 5109 links; and Harvard University (Cambridge, MA) contributed 15 documents with 4484 links (Fig. 7).

The most productive organizations and collaboration links.
Co-citation analysis (authors)
In our co-citation study, the unit of analysis was the author, requiring a minimum of 40 citations per author. Among 10,732 authors, 38 met this threshold, and their total co-citation link strength with other authors was calculated. Notably, Christina Puchalski emerged as the most cited author with 209 citations and a total link strength of 1441, followed by Tracy Ann Balboni with 189 citations and 1409 links. In addition, Harvey Max Chochinov obtained 287 citations and 1317 links, ranking third in the analysis (Fig. 8).
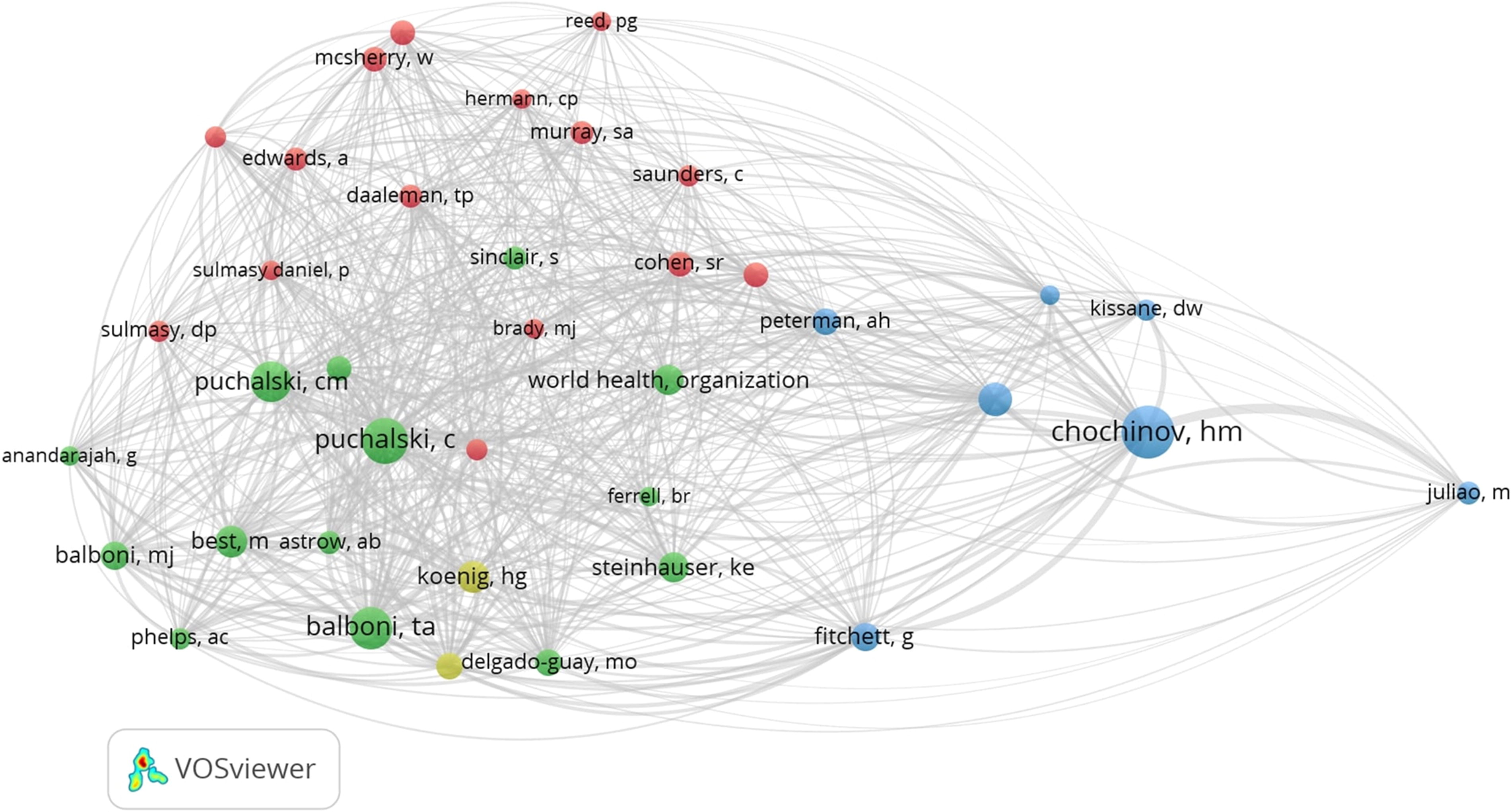
Co-citation analysis for authors.
Discussion
This is the first bibliometric analysis of the published literature which focuses on the relationship between spiritual care, palliative care, and EoL. Similarly to what happens in other sciences (e.g., sociology, economics, and, more generally, the historical sciences), the idea of “pure data” does not exist, as data itself are open to multiple interpretations. This also applies to this bibliometric analysis, which demands critical interpretation of the information gathered from the retrieved dataset, and as such, multiple relevant elements can be deduced from our investigation.
Our research has underscored that some journals have shown a keen interest in the topic of the role of spiritual care in palliative medicine and EoL. For instance, the Journal of Pain and Symptom Management, the Journal of Palliative Care, and the Journal of Palliative Medicine have published 87, 49, and 37 papers, respectively. Consequently, authors intending to publish on spiritual care should focus primarily on these journals. More specifically, the Journal of Palliative Medicine also emerged as the most-cited journal, with 1052 citations and 23,896 links. This observation may indirectly reflect that researchers have long perceived the Journal of Palliative Medicine as the leading target journal for their investigations in the field of spiritual care. Furthermore, as the number of citations tends to reflect the quality of articles, we suggest that clinicians and researchers interested in the topic of spiritual care carefully scrutinize the top 10 cited publications first.7,19,29–36
It is also interesting to note that the majority of the studies concerning the relationship between spiritual care and the terminal phases of life were published in the 2019–2021 period, with a 42.9% increase compared with the previous 3-year period (2016–2018). This coincided with the time when the world was hit by the COVID-19 pandemic. There are various potential factors that could account for this finding.
First, the pandemic’s profound impact, including heightened isolation, loneliness, and vulnerability, alongside the strain on health care systems and the burden of serious illness and caregiver overload, has highlighted the importance of prioritizing spiritual care for whole-person palliation. 38 Such emphasis aimed to enhance the QoL and the experiences of patients and families grappling with spiritual crises amid the life-and-death scenarios inherent in COVID-19. 39 In such challenging contexts, where the complexity and severity of disease created unforeseen changes resulting in anxiety, fear, stress, and loss of hope, spiritual care has emerged as a significant coping strategy. 40
Second, in that context, death—which had long been placed on the margins of most people’s personal and social lives—increased in relevance throughout Eastern and Western societies bringing back that mortal aspect of life that seemed to have been, if not eradicated, ignored, at least in the West. 37 Third, while the pandemic limited access to traditional sources of spiritual support (i.e., religious services, religious leaders, and family visits),41,42 hospitals sought to bridge the gap through novel technological communication tools (i.e., video calls and telephone conversations). 43
Hence, the notable increase (42.9%) in publications on spiritual care during the pandemic may also reflect a collective effort within the scientific community to address the spiritual needs of the patients during these trying times. This trend aligns with broader shifts observed in palliative care research, as highlighted by Wang et al., which have focused on system improvement (61.8%), patient care (27.0%), and bereavement support (6.5%). 44
Semantic network exploration serves as a pivotal element in network analyses, as it clarifies the themes of research and the objectives within a specific field. Our bibliometric analysis shows that the term “spirituality” in the context of the EoL consistently intertwines with “palliative care.” This association is in line with both the holistic nature of palliative care and the recognition of spirituality as a fundamental aspect of patient experience at the EoL and can be attributed to several factors supported by existing research.
First, palliative care aims to provide—by its nature—holistic support to patients facing life-threatening illnesses. It not only focuses on physical symptoms but also addresses psychosocial and spiritual needs by recognizing spirituality as one of the key domains of palliative care, alongside physical, psychological, and social aspects. 45
Second, research has demonstrated that spirituality can provide patients with a sense of meaning, purpose, and connection, helping them to cope with illness, find comfort, and experience peace and acceptance in their final days. 46
Lastly, contemporary guidelines and standards of practice in palliative care emphasize the need for health care providers to assess the spiritual needs of patients alongside physical and psychosocial concerns as part of comprehensive EoL care. 47
Interestingly, our analysis also revealed that the words “spirituality” and “religion” were associated with “palliative care” as well. While this connection may appear obvious at first glance, upon more careful evaluation, it encompasses two intrinsically different paradigms. Although often used interchangeably, the terms “spirituality” and “religiosity” are distinct in many ways. While religiosity pertains to specific beliefs and principles adhered to within a religious framework, spirituality represents a more informal state of existence. 48 Spirituality is a dynamic and evolving process that, while incorporating the beliefs and practices of religious communities, extends beyond religion to encompass how individuals find ultimate meaning, purpose, and transcendence through avenues such as vocation, family, or nature. 49 While spirituality may manifest through religious rituals, it can also be experienced and expressed within broader contexts (e.g., interpersonal relationships, cultural interactions, or encounters with nature). For many terminally ill patients, spirituality and religiosity play vital roles in their experience and response to illness, particularly aiding in the acceptance of diagnosis. This was highlighted in a study by Balboni et al., where 88% of respondents identified religion and spirituality as crucial factors in helping them adapt to their illness. 30
Another element emerging from our bibliometric study is that the majority of research on spiritual care and EoL matters originated from the Anglo-American region (namely, the United States and the United Kingdom). This observation may be attributed to several factors. While these regions host several renowned research centers (e.g., Harvard University in Cambridge and the Dana-Farber Cancer Institute in Boston, both in Massachusetts) with a keen scientific interest in palliative care, there is also a strong cultural connection between EoL discussions and spiritual care in Anglo-American cultures. Despite the increasing global recognition of professional spiritual care and its association with improved health outcomes, the provision of spiritual care in different settings may have unique culture-specific aspects because of diverse spiritual approaches. Our investigation aligns with American studies indicating a significant interest in spiritual care among patients, ranging from 35% to 54%.15,50–52 In addition, spirituality was found to play a significant role in countries with established spiritual care services, notably among older persons and Black and Latinx populations in the United States. 53 Interestingly, an investigation by Best et al. conducted in Australia suggested a similar desire among patients to discuss spirituality, despite the country being more secular compared with the United States. 54 Conversely, while tensions between religious and secular identities may impact spiritual care provision, research focusing on the spiritual care needs of Muslims in Israel conducted by Baddarni et al. indicated that this tension may be less relevant for Israeli Muslims. 55 As a result, efforts are ongoing to develop culturally valid tools for accurately identifying predictors of interest in spiritual care, tailored to specific cultural contexts (i.e., Spain, Iran, or African American communities).56–58
Another remark that can be inferred from our analysis is that nurses and chaplains are significantly more engaged in the palliative–spiritual care “dimension” than physicians (Fig. 4). This finding aligns with the prevailing notion that specialized providers (i.e., chaplains) have traditionally assumed responsibility for addressing patients’ spiritual needs. 59 In an Australian study by Keall et al., this was deemed the primary approach to addressing spiritual and existential needs, 60 whereas referrals were seen as part of a collaborative team approach in hospice care in an investigation by Belcher et al. 61 Likewise, nurses, having direct exposure to spiritual suffering and fostering genuine relationships with patients, were also considered as appropriately placed to provide spiritual care. 62 Consequently, spiritual care has long been viewed as integral to the role and holistic ethos of nursing, 63 as evidenced by nurses’ acknowledgment of this responsibility, with 92.6% concurring in the United Kingdom’s largest national nursing survey on spirituality and spiritual care. 64 Moreover, various studies have shown how nurses’ personal experiences of loss and illness shape their spiritually integrated approach.60,61,65,66 In contrast, medical care over time has increasingly fractionalized the different biopsychosocial-spiritual aspects of individuals, ultimately relegating spirituality.67,68 This, coupled with the observation by Ford et al. that trainee physicians perceive discussing religious and spiritual matters as requiring advanced communication skills beyond standard training, 69 may explain the limited role doctors play in providing spiritual care. Nonetheless, research by Post et al. found that a significant percentage of patients want their physicians to inquire about their spiritual needs, 70 and numerous studies have demonstrated that discussing patient spirituality can enhance physician awareness of factors influencing decision making, strengthen doctor–patient relationships, increase patient satisfaction, improve QoL, and enhance communication.18,30,71–73
In summary, while these findings highlight the importance patients attribute to physicians addressing their spiritual concerns and viewing them holistically, they also acknowledge the challenges doctors face in discussing spirituality. They also indicate the potential benefits in facilitating effective practice and addressing patients’ unmet spiritual needs, which may adversely affect their well-being.
Study Limitations
This is the first bibliometric analysis aiming to provide insights from existing evidence on spiritual care, palliative medicine, and EoL topics. Nevertheless, it is crucial for readers to acknowledge certain study limitations.
First, bibliometric studies cannot replace systematic reviews or meta-analyses that yield conclusive findings for evidence-based medicine. However, when used on bibliometric datasets, clustering techniques offer a visually impactful overview.
Moreover, our literature review relies solely on the WoS database. We made this choice due to the inability to conduct citation and co-citation analyses within the PubMed database. In addition, the increasing adoption of WOS for bibliometric analysis in recent years influenced our decision.
In addition, a further notable limitation of this analysis concerns the time factor. Newer publications have had fewer opportunities for citations in subsequent works compared with earlier published papers. Therefore, while the current findings are subject to change, our contribution presents an appealing “snapshot” of previously published data at the time of the present publication.
To conclude, another potential constraint of this analysis pertains to the structure of the underlying network. Since the connections between publications rely on citations or word associations only, keywords, the frequency of words cited throughout the text, affiliations, and other factors exert a substantial influence on the representation of the outcomes.
Conclusion and Future Perspectives
The current bibliometric network analysis focusing on the role of spiritual care within palliative medicine and EoL care emerges as a pivotal resource showing potential to direct forthcoming research in this realm. This study has elucidated who the leading scholars and central research groups are while also providing a holistic view of scientific output published on this topic in the literature. Although our investigation does not directly improve patient management, as a result of the detailed analysis of all the articles on the issue of spiritual care in EoL and palliative medicine, we still believe that the most influential studies, the most focused topics, global productivity, and their discussion provide important statistical information on this subject for clinicians, scientists, and health care providers involved in caring for the terminally ill.
Moving forward, it is crucial for upcoming research to prioritize cultivating an interdisciplinary dialogue that spans beyond the realms of the medical and philosophical sciences, extending into sociology and cultural anthropology. This will ensure a more comprehensive exploration of these themes, ultimately fostering a deeper understanding of the same.
Moreover, to facilitate the broader practical integration of spiritual care into clinical practice, establishing additional research networks becomes paramount. Such effort aims to spread best practices and expand the scope of incorporating spiritual care into diverse clinical settings worldwide.
Footnotes
Acknowledgment
The authors would like to thank Kate Gralton for English-language editing.
Authors’ Contributions
J.D.U.: Conceptualization, study design, investigation, methodology, and writing—original draft. C.C.: Investigation, methodology, and writing—original draft. R.L.: Methodology, data curation, and writing—original draft. V.L.: Supervision, data curation, and writing—reviewing and editing. E.M.: Investigation, methodology, and writing—reviewing and editing. F.M.: Supervision, data curation, and writing—reviewing and editing.
Availability of Data and Materials
Further information is available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This article did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.