
Abstract
Background:
Naldemedine, a peripherally acting opioid μ receptor antagonist, is effective for prevention of opioid-induced constipation (OIC); however, evidence on its use in children is limited.
Objective:
To evaluate the efficacy and safety of naldemedine in pediatric patients with OIC.
Design, Setting/Subjects:
Retrospective analysis of 32 pediatric patients with OIC treated with naldemedine in a single institution in Japan from June 2017 to March 2021.
Measurements:
Efficacy was evaluated in 13 evaluable patients with bowel movement (BM) response, defined as those with at least three BMs in the first 7 days after naldemedine initiation and an increase of at least one BM from baseline. Safety was evaluated by examining adverse events (AEs) based on the Common Terminology Criteria for AEs (v5.0).
Results:
BM response was recorded in 11 of the 13 patients (85%), and the number BMs per day significantly increased from 0.43 before naldemedine to 1.00 after naldemedine (p = 0.025). The most common AE was diarrhea, observed in 16 of the 32 patients (50%), and all instances were grade 1 or 2. In three of the 16 patients, naldemedine was discontinued owing to worsening diarrhea.
Conclusions:
In pediatric patients, naldemedine resulted in a high rate of BM response and increased the BM frequency, indicating its efficacy. In some patients, grade 2 diarrhea required naldemedine discontinuation, suggesting that it should be used with caution in pediatric patients. Further studies are warranted to determine the optimal naldemedine dose in pediatric patients.
Introduction
Opioid analgesics have a long history of use in the management of chronic cancer and noncancer pain and are widely used in children as well as in adults.1,2 Side effects of opioid analgesics include drowsiness, nausea, vomiting, and constipation. Opioid-induced constipation (OIC) has been reported in 51%–87% of adult patients with cancer and in 41%–57% of adult patients with noncancer pain.3–7 OIC is associated with poorer quality of life. Importantly, in children, OIC is also a cause of decreased adherence that requires immediate intervention. 8 OIC, which is caused by decreased gastrointestinal motility via opioid μ receptors in the gastrointestinal tract,9,10 differs from nonopioid-related constipation as it impacts a variety of gastrointestinal functions including motility and secretion. 11 Conventional medical therapy for OIC uses osmotic or colon-stimulating laxatives. 5 However, these agents may have limited efficacy as they do not address the underlying cause, which is distinct from that of nonopioid-related constipation. 12 Naldemedine, a peripheral opioid μ receptor antagonist that exerts its effect through a different mechanism than conventional laxatives, was approved for the treatment of OIC in Japan in March 2017; naldemedine is also used overseas.13,14
Our hospital is a tertiary hospital that accepts severely ill pediatric patients, some of whom use opioids and suffer from OIC. The overall safety and efficacy of naldemedine do not differ between patients aged 65 years and older and those of all ages 15 ; however, the efficacy profile of naldemedine and associated adverse events (AEs) in children remain unclear. In the present study, we aimed to evaluate the efficacy and safety of naldemedine in children with OIC.
Materials and Methods
Patients
This retrospective study included patients aged <19 years with OIC who received naldemedine in the National Center for Child Health and Development in Tokyo, Japan from June 2017 to March 2021 (Fig. 1). Patients who were treated with naldemedine for fewer than 7 days and those whose bowel movement (BM) status was unknown, not documented in the medical records were excluded. The general OIC criteria are described in the Rome Committee’s criteria for OIC diagnosis (Rome IV criteria); it is intended for adults and is very difficult to apply to children. In this study, as infants and toddlers who had not yet established their will were included, we used their medical record entries such as defecation frequency and their own complaints as references. The diagnostic criteria for OIC in this study were as follows: BM less than three times/week, straining, residual stools, separate hard lumps like nuts, and abdominal distention. We excluded two patients who received prophylactic naldemedine in our assessment of efficacy.
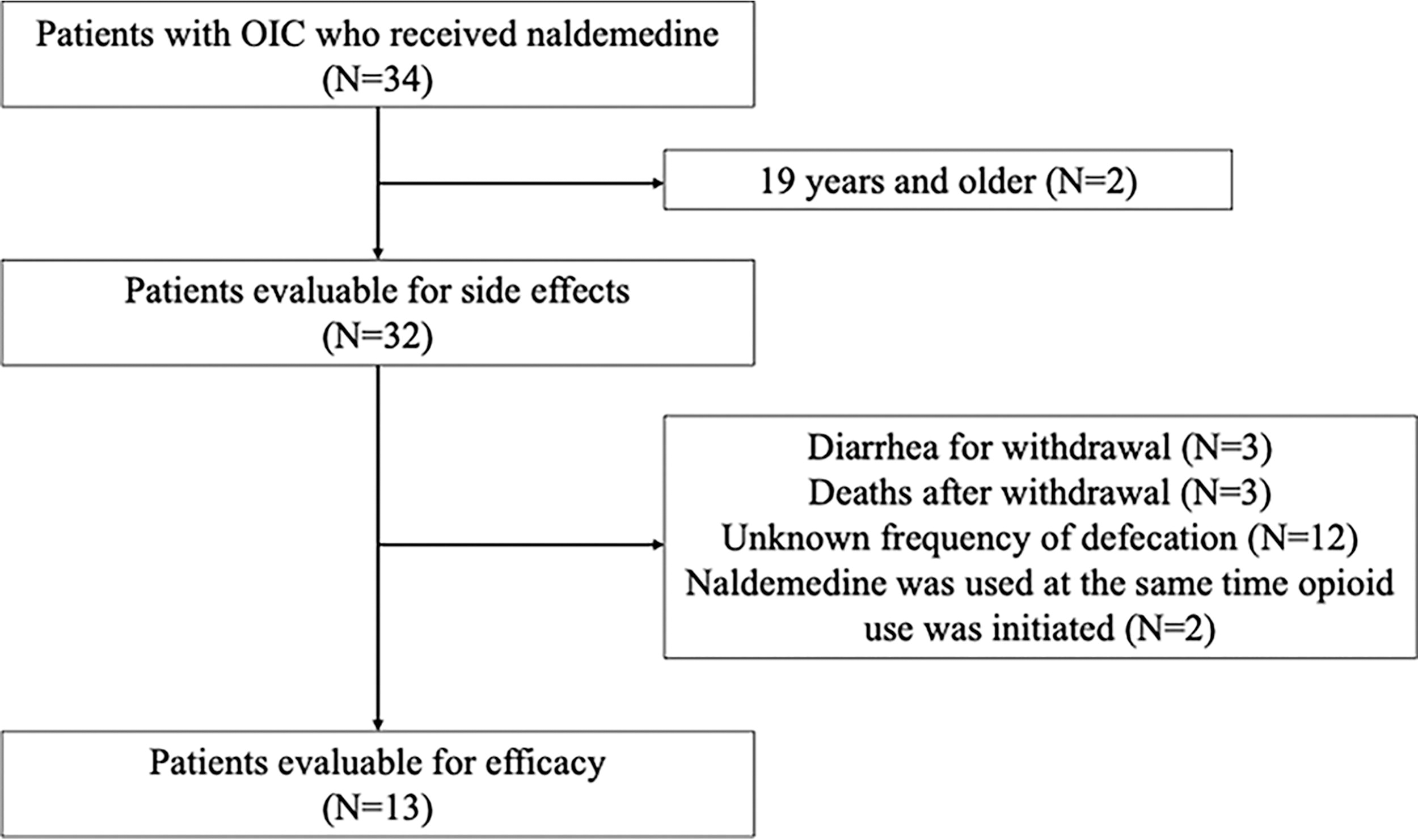
Patient selection flow. Evaluable patients had defecation frequency for at least 7 days and 7 days before and after the naldemedine initiation.
Study procedures and assessment
Clinical data were retrospectively collected based on the review of the medical records. Efficacy was evaluated in 14 patients who received naldemedine for at least 7 days and could be observed for at least 7 days before and after the start of naldemedine initiation. The primary outcome was the rate of BM responders. BM responders were defined as those who had at least three BMs in 7 days after naldemedine initiation and those with an increase of at least one BM within 7 days of naldemedine initiation compared with the number of BMs during the 7 days before the naldemedine initiation. The secondary outcome was the change in the number of BMs before and after naldemedine. Additional laxative use at the start of naldemedine initiation and additional laxative use after naldemedine were also evaluated. The use of a new laxative within 7 days after the initiation of naldemedine initiation was defined as the use of additional laxatives. Safety was assessed using the Common Terminology Criteria for AEs version 5.0 based on the review of AEs that occurred within 7 days of naldemedine initiation. Regarding the evaluation of fecal characteristics, diarrhea was defined as any stool described as diarrhea or muddy/watery stool in the medical records. For cases classified as diarrhea, the average number of BMs per day during the 7-day period before and after naldemedine initiation was calculated and the change in the number of BMs after naldemedine initiation was evaluated using a grading scale. Grade was rated on a scale of 4 about diarrhea, stomachache, increase aspartate aminotransferase (AST), increase alanine aminotransferase, vomiting, opioid withdrawal syndrome. In this study, the number of patients for whom efficacy can be evaluated is smaller than the number of patients for whom side effects can be evaluated owing to reasons such as unknown frequency of defecation.
Statistical analysis
All statistical analyses were performed with EZR (Saitama Medical Center Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). A p value of 0.05 was used as the level of significance. Wilcoxon’s rank-sum test was used to compare the number of BMs per day before and after naldemedine.
This study was conducted after obtaining approval (approval no. 2021–081) from the Ethics Committee of the National Center for Child Health and Development and it was conducted with informed consent from patients. The results of this study are stored in our hospital (Department of Pharmaceuticals, National Center for Child Health and Development, 2–10–1 Okura, Setagaya-ku, Tokyo, Japan).
Results
Study cohort
The background characteristics of the study cohort are summarized in Table 1. In this study, all patients had one or more of the following symptoms: BM less than three times/week, straining, residual stools, separate hard lumps like nuts, and abdominal distention, all of which met the criteria for OIC. The study did not narrow down the target diseases but did not include patients with chronic pain. One patient was given naldemedine for a nonserious illness but was excluded because he was over 19 years of age. The median age was 9 (range, 0.6–18) years. The median opioid doses during the 7-day period before and after naldemedine were 0.5 (range, 0–11.7) and 0.7 (range, 0–10.5) mg/kg/day, respectively, with no statistically significant difference (p = 0.37). The minimum opioid dose before naldemedine was 0, as two patients received naldemedine simultaneously with the initiation of opioid initiation. The median naldemedine dose was 0.0058 (range, 0.0012–0.020) mg/kg/day.
Patient Characteristics
Patients with one or more of the following: BM less than three times/week, straining, residual stools, separate hard lumps like nuts, and abdominal distention.
Results are shown as median (Min–Max).
Dose of opioid analgesics was used by converting into equivalent oral morphine dose.
The rate of BM response
As shown in Table 2, 11 of the 13 patients (85%) were BM responders according to the study definition. Four of the 13 BM responders were taking additional laxatives. Therefore, 78% of the BM responders were not on additional laxatives.
Proportion BM Responders
The frequency of BMs
Among the 13 BM responders, the median number of BMs per day significantly increased from 0.43 before naldemedine to 1.00 after naldemedine (p = 0.025) (Fig. 2A). Five of these patients used additional laxatives after naldemedine. Conversely, in 9 BM responders who did not require additional laxatives, the median number of BMs per day significantly increased from 0.43 before naldemedine to 1.0 after naldemedine (p = 0.029) (Fig. 2B).
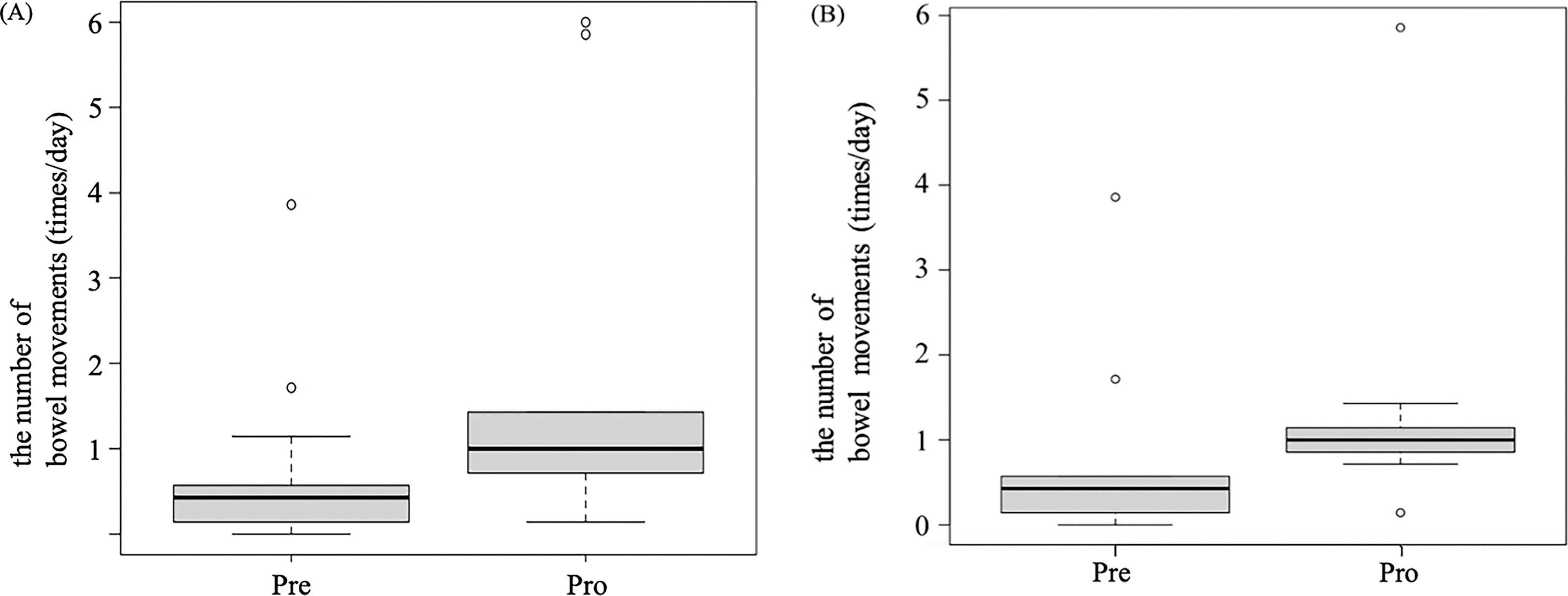
Change in defecation frequency from baseline with naldemedine initiation. Change in the number of bowel movements per day after the initiation of naldemedine. The rate of bowel movement frequency (times/day) during the 7-day period before and the 7-day period after the initiation of naldemedine was calculated in
Safety of naldemedine
Diarrhea, which occurred within 7 days of initiating naldemedine, was the most common AE, occurring in 16 of the 32 patients evaluated for AEs (50%) (Table 3). Three of the 16 patients discontinued naldemedine (19%); in these three patients, the duration of opioid use was 14 (range, 4–33) days. One of the three patients refused to take the naldemedine owing to anal pain caused by excessive number of BMs, and the remaining two patients discontinued naldemedine owing to excessive watery stools at the discretion of the physician. All three patients (9.4%) recovered to have tangible stools after naldemedine discontinuation, and worsening of diarrhea was not observed.
Adverse Events During the Treatment Period
The number of adverse events (%) that occurred within 7 days of starting naldemedine.
Grade 1 and 2 diarrhea was observed in 12 (38%) and 4 (13%) patients, respectively, whereas grade 3 or more severe diarrhea was not observed in any of the patients. The median naldemedine dose was 0.0075 (range, 0.0070–0.0086) mg/kg/day in four patients (13%) with grade 2 diarrhea and 0.0054 (range, 0.0012–0.020) mg/kg/day in the remaining 28 patients.
Other AEs were grade 1 abdominal pain in three patients (9.4%) and grade 1 elevated AST, which was transient, in one patient. Abdominal pain improved with hot compress therapy in all patients. No patient developed opioid withdrawal symptoms, such as sweating or vomiting. Diarrhea occurred in 11 patients (34%) during the first 3 days of naldemedine initiation. Seven of the 32 patients (22%) took naldemedine after dinner; three of these patients (9.4%) experienced sleep disturbance owing to nocturnal diarrhea.
Discussion
This is the first study that evaluated the efficacy and safety of naldemedine in pediatric patients, and the BM response rate was 86%. This response rate is comparable with previous studies in adults and could be used effectively in children.16–17 In this study, we used a different approach to determine BM response, which excluded self-defecation because many of the patients in the present study were nearing end of life due to primary disease or had difficulty taking medication due to cancer pain and used transrectal or suppository therapy before or at the same time as naldemedine. The BM frequency was also significantly increased in nine patients who did not receive additional laxatives after naldemedine, suggesting that naldemedine would increase the frequency of BMs. These results are similar to the number of self-defecations per week reported in a phase II Japanese–Korean study of patients with cancer treated with naldemedine. 17
Regarding the safety of naldemedine, the rate of diarrhea was 38%, which was higher than that reported in adult patients with cancer in one Japanese–Korean interventional study (1108V9222) and two phase III studies in Japan (1331V9236 and 1332V9237).18–20 However, our review of the medical records of patients with grade 1 diarrhea revealed the resolution of constipation and bloating and the improvement in quality of life following naldemedine, suggesting that grade 1 diarrhea might not be necessarily an AE in these patients. There were four cases of grade 2 diarrhea and three cases that led to discontinuation. In clinical trials of naldemedine in adults, diarrhea has been reported to occur in a dose-dependent manner; diarrhea, particularly moderate or severe diarrhea, was more frequently observed in patients treated with 0.4 mg naldemedine compared with those treated with 0.2 mg naldemedine in a phase II study.17,21 Assuming an adult body weight of 50 kg, the naldemedine doses of 0.2 and 0.4 mg correspond to 0.004 and 0.008 mg/kg/day, respectively. In the present study, grade 2 diarrhea occurred in all patients treated with at a minimum naldemedine dose of 0.007 mg/kg/day, confirming that grade 2 diarrhea might have occurred in pediatric patients receiving a naldemedine dose that was equivalent to the 0.4 mg naldemedine dose in adults. This finding implicates that naldemedine might be associated with more severe diarrhea in children treated with naldemedine at doses akin to the high adult doses.
The incidence of naldemedine-associated diarrhea is highest on the first day of initiation and gradually decreases thereafter. 22 In the present study, diarrhea was also observed in 11 patients between days 1 and 3 and resolved in three of these patients. In the remaining eight patients, the diarrhea may have been transient in the early phase of naldemedine initiation, as the patients showed a gradual and marked recovery of stools after the fourth day of continued initiation and no worsening of diarrhea was observed. Transient diarrhea can also lead to poor adherence; therefore, the possibility of diarrhea in the early days of naldemedine initiation should be shared with the medical staff, the patient, and the patient’s family. In addition, large amount of nocturnal stools led to sleep disturbance in three patients who took naldemedine after dinner, requiring temporary treatment discontinuation. A phase III validation study including patients with cancer in Japan (V9236) 16 reported that the median time to first BM after naldemedine initiation was 4.67 hours, indicating that the drug should be administered during the day.
The main study limitations are the small sample size and the retrospective study design. Not all stool characteristics that were documented in the medical records were assessed using a common assessment method, and some were based on patient self-assessment. It is possible that not all diarrhea episodes might have been recorded or assessed in the medical records and that the rate and severity of diarrhea might have been underestimated. In addition, the present study did not evaluate the association between drug interactions and efficacy. It should also be noted that the patients included were severely ill patients and not chronic pain patients. Future studies with larger cohort sizes are warranted to confirm the current study findings and to determine the optimal dose of naldemedine in pediatric patients with OIC.
Conclusions
Naldemedine induced BM response and increased the BM frequency, indicating its efficacy in pediatric patients. Grade 2 diarrhea observed in some patients required the discontinuation of naldemedine, suggesting that it should be used with caution in pediatric patients.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
We have no conflicts of interest.