
Abstract
Background:
Gastrostomy (feeding) tubes are one way of managing swallowing impairments (dysphagia) in patients living with serious illnesses. For patients, families, and health care providers to make well-informed, preference-aligned decisions regarding gastrostomy tube placement, each group must understand the other’s goals, concerns, and perspectives.
Objective:
Thus, the goal of this scoping review is to characterize the factors influencing gastrostomy tube placement decisions for people with serious illnesses.
Methods:
We first identified relevant studies in a systematic manner, using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram to model our screening process. We then used deductive thematic analysis to describe major themes, reporting the data with descriptive statistics such as percentages. Studies were categorized by their primary participant populations (patients, caregivers, and health care providers), with subthemes organized within the major themes of goals, concerns, considerations, and decisional preferences.
Results:
When considering gastrostomy tube placement, the top themes for patients were extending life (56% of studies), decisional control (56%), quality of life (48%), physical and social limitations and image (44%) and personal factors (44%). For caregivers, the primary themes were decisional control (71% of studies), extending life (50%), personal factors (50%), maintaining nutrition (43%), and knowledge (43%). Finally, health care providers prioritized decisional control (58% of studies), knowledge (53%), quality of life (47%), extending life (42%), and societal factors (42%).
Conclusions:
Our results highlight key factors that may help center patient preferences when making gastrostomy tube-related decisions, as well as critical areas where more research is needed to help improve decision-making surrounding gastrostomy tube placement. Providing adequate knowledge and understanding patient preferences is critical for patients to make high-quality medical decisions regarding gastrostomy tubes.
Introduction
Difficulty swallowing, or dysphagia, is a common sequela of many health conditions that carry a high risk of mortality and negatively impact a person’s daily function or quality of life. Defined as serious illnesses, in many of these health conditions, including amyotrophic lateral sclerosis (ALS), Parkinson’s disease (PD), multiple sclerosis (MS), progressive supranuclear palsy (PSP), dementia, advanced cancer, heart failure, and chronic illness in aging adults with multiple comorbidities, dysphagia is expected to develop at some point during the disease process. In fact, the prevalence of dysphagia can be as high as 65% in advanced cancer,1,2 98% in ALS, 3 85% in advanced dementia, 4 and 82% of hospitalized adults over the age of 80. 5 For most patients with serious illnesses, dysphagia has a low likelihood of resolving, resulting in reduced quality of life 6 and increased mortality 7 throughout the duration of the disease process.
When dysphagia is not expected to improve, best practices for its management are unclear and treatment strategies may require significant tradeoffs. Gastrostomy tube placement is one way of managing dysphagia in these cases; however, in the absence of published data suggesting that gastrostomy tube placement improves patient outcomes in these populations, decision-making surrounding dysphagia management is challenging and practice patterns are highly variable. 8 Because the evidence regarding the benefits of gastrostomy tubes in these populations is mixed regarding survival and life expectancy,9,10 the decision for their placement could be considered “preference-sensitive,” meaning the choice depends primarily on the personal preferences of patients and caregivers. The literature, however, suggests that factors such as provider preference, socio-economic status, and cultural considerations, may also play a role in determining whether individuals living with serious illnesses should receive a gastrostomy tube.11,12
Patient-centered care is a key element of high-quality care where patients and their families or caregivers are active team members in the medical decision-making process. 13 For patients, caregivers, and healthcare providers to work effectively as a team, it is critical for each to understand the other’s goals, concerns, and perspectives when facing a medical decision, such as whether a gastrostomy tube should be placed. To date, there has been limited work synthesizing the existing literature on the factors considered by individuals with serious illnesses, caregivers, and healthcare providers regarding gastrostomy tube placement. With the goal of optimizing patient-centered dysphagia management for individuals with serious illnesses, as a first step, we conducted a scoping review to identify the factors influencing gastrostomy tube placement decisions for this population.
Methods
Search strategy
To find studies related to gastrostomy tube placement, two authors (T.H.K. and B.J.P.) developed a search query using subject headings and terms related to decision-making factors (i.e., quality of life, patient preference, and perspective) and nutritional modes (i.e., feeding, nutrition, and gastrostomy). The search was conducted in PubMed, CINAHL, and PsychInfo databases and included articles published before June 15, 2022, using the following terms: “quality of life” or satisfaction or “level of comfort” or “focus groups” or interview* or survey* or thoughts or perspective* or experience* or misconce* or feel* or attitude* or decision making or psychology or “patient preference”[mesh] or belief* or perception*) and (feeding or enteral or nutrition or gastrostomy or “enteral nutrition”[mesh]) and (tubes or percutaneous endoscopic gastrostomy or PEG) and patients. The articles obtained were then imported into Covidence for data management and extraction. Additional articles were identified through forward and backward citation searches. For forward citation searches, we looked within our search databases for recent literature that cited the articles found using our search terms. For backward citation searches, we used the reference section of articles found using our search terms to identify articles meeting our search criteria. All studies underwent title and abstract screening before moving to the full-text review.
Study selection
Covidence was used to conduct title screens, abstract screens, and full-text reviews and to track agreements and disagreements regarding study inclusion. The study team was comprised of three speech-language pathologists and one clinical research coordinator. Title screens, abstract screens, and full-text reviews were completed by two members of the study team. A third team member was used to review instances where there were disagreements between the initial two reviewers. Articles met inclusion if they were in English and pertained only to adult populations with serious illnesses, including ALS, PD, MS, PSP, dementia, advanced cancer, heart failure, and chronic illness in aging adults with multiple comorbidities.
Because our search was focused on perceptions of gastrostomy tubes, articles that focused on different types of gastrostomy tubes, comparing gastrostomy tube types, or procedures for gastrostomy tube insertion were excluded. We also excluded secondary studies, which we defined as articles that were not the original sources of data but rather summarized previously published findings. These included commentaries, synopses, and narrative reviews. Additionally, we excluded articles that did not have available full-text versions, that were published in languages other than English, or that were unrelated to chronic serious illnesses.
The selection process is visualized in Figure 1 based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews Checklist. In total, our search yielded 1733 studies. After eliminating duplicates, screening titles and abstracts, and reviewing full-text articles, we ultimately included 60 articles for data analysis.
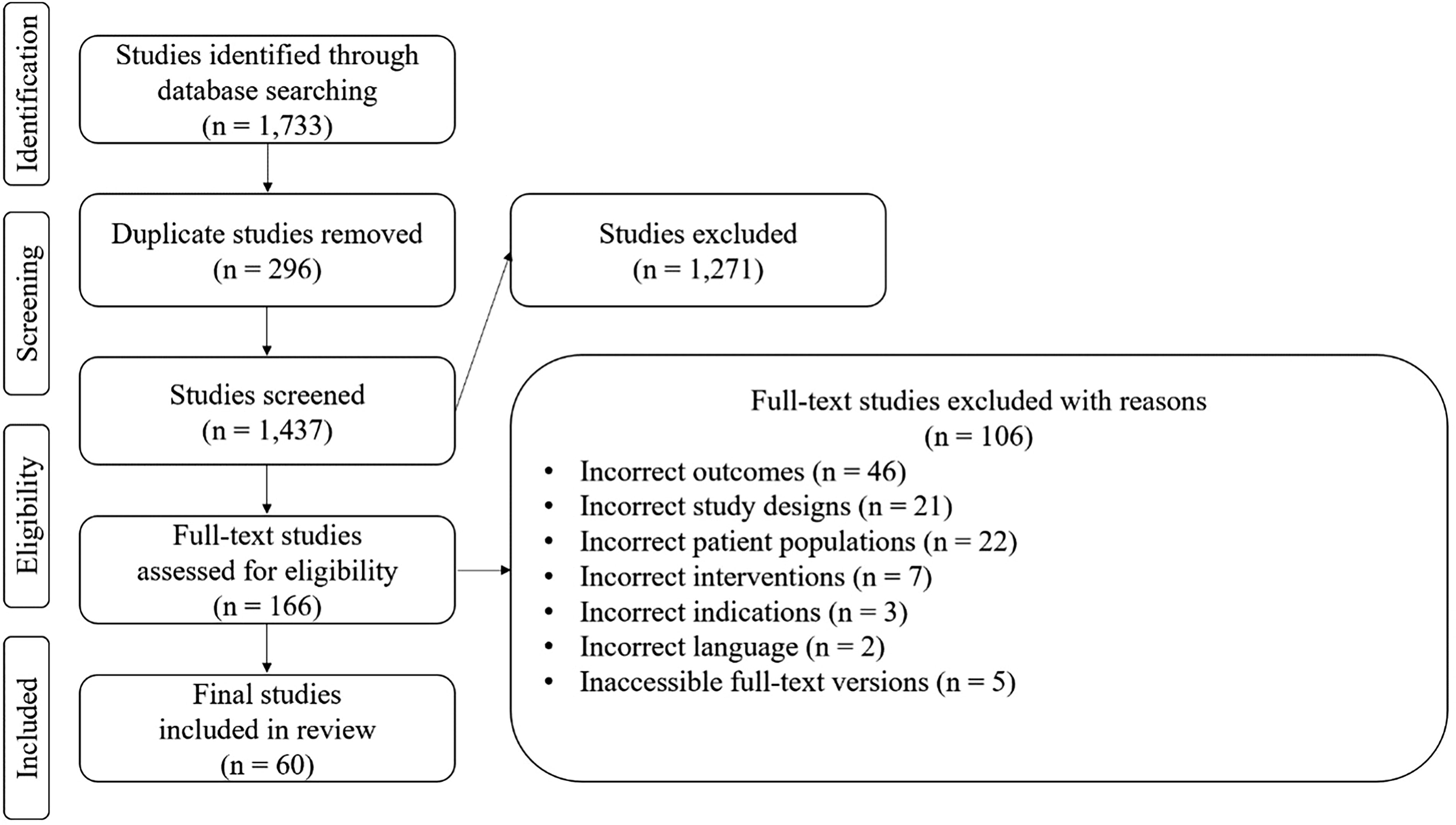
Literature search and selection process.
Data extraction and analysis
We performed a deductive thematic analysis of the data. 14 The first author (B.J.P.) developed a preliminary set of subthemes based on prior knowledge of the subject. Then, all study team members identified and coded articles using the preliminary set of subthemes if deemed appropriate or by adding additional subthemes when perspectives regarding gastrostomy tube placement that did not match or were not included in the preliminary set were identified. After initial coding by the study team, two authors (B.J.P. and T.H.K.) examined the final set of codes for overlap within subthemes. The second author (T.H.K.) then reviewed the articles for inconsistencies, ensuring that all appropriate codes were included without decontextualization. The subthemes within each category were then tallied by study population (patient, caregiver, healthcare provider) and across all studies.
Results
Thematic analysis
The subthemes were then grouped into four main categories by two authors (B.J.P. and T.H.K.): goals, concerns, considerations, and decisional preferences Table 1. The “goals” category included preferences for gastrostomy tube placement and had five subthemes. “Concerns” involved apprehensions regarding gastrostomy tube placement and had four subthemes. “Considerations” included social-ecological 15 factors that may influence whether a person should or could receive a gastrostomy tube and consisted of six subthemes. “Decisional preferences” covered factors related to decisional control (i.e., the power of the individuals involved in gastrostomy tube placement decision-making), satisfaction, and regret and had two subthemes.
Top subthemes
The most prevalent themes among all studies were decisional control (60% of all studies), extending life (50%), and quality of life (45%). For patients, the five most frequently reported themes were extending life (56% of patient studies), decisional control (56%), quality of life (48%), physical and social limitations and image (44%), and personal factors (44%). For caregivers, the five themes were decisional control (71% of caregiver studies), extending life (50%), personal factors (50%), maintaining nutrition (43%), and knowledge (43%). For healthcare providers, the themes were decisional control (58% of healthcare provider studies), knowledge (53%), quality of life (47%), extending life (42%), and societal factors (42%). Table 2 lists the populations and subthemes for each article.
Themes and Subthemes of Patient, Caregiver, and Healthcare Provider Perspectives of Gastrostomy Tube Placement
PEG, percutaneous endoscopic gastrostomy.
Details of Included Studies, Including Populations and Themes
ALS, amyotrophic lateral sclerosis.
Goals Related to Gastrostomy Tube Placement
Concerns Related to Gastrostomy Tube Placement
Considerations Related to Gastrostomy Tube Placement
Decisional Preferences Related to Gastrostomy Tube Placement
Top subthemes by category
Goals
Extending life was the most reported goal across all studies (50% of all studies) and for each group (patient, caregiver, and healthcare providers). Maintaining nutrition was the second most reported goal for all groups, appearing as a primary theme in 37% of all studies. However, the third most reported goal differed among the groups, with eating by mouth (30% of patient studies) being the third most reported goal for patients and reducing symptom burden (36% of caregiver studies and 11% of healthcare provider studies) for caregivers and healthcare providers. Table 3 lists the most reported goals for gastrostomy tube placement compared by group.
Concerns
Physical and social limitations were the most frequently reported concern across all studies (40% of all studies) and the most frequently reported concern for patients and healthcare providers (44% of patient studies and 42% of healthcare provider studies). Medical complications were the second most reported for patients and healthcare providers (37% of patient and healthcare provider studies) and the most reported concern for caregivers (42% of caregiver studies). The second most reported concern for caregivers was evenly split between caregiver burden and physical limitations (29% of caregiver studies). Concern for gastrostomy tube maintenance was the third most reported concern across all studies (18% of all studies); however, it was the least common concern among the caregiver studies, with only 2 of 14 studies containing this theme. Table 4 lists the most reported concerns about gastrostomy tube placement compared by group.
Considerations
Overall, quality of life was the most frequently reported consideration of all three groups (45% of all studies), followed by personal factors (43%). However, the order of priority differed among the groups. For patients, the most common consideration was quality of life (48% of patient studies), followed by personal factors (44%) and knowledge (30%). In contrast, for caregivers, personal factors were the most found consideration (50% of caregiver studies), followed by knowledge (43%); quality of life and societal factors were both the third most reported consideration (36%). For healthcare providers, knowledge was the most reported consideration (53% of healthcare provider studies), followed by quality of life (47%) and societal factors (42%). Table 5 lists the most reported considerations for gastrostomy tube placement compared by group.
Decisional preferences
Only two subthemes emerged in this category. The subtheme of decisional control was the most prevalent, appearing in 60% of all studies. Alignment with care preferences was identified in 23% of all studies. Table 6 lists decisional preference themes found in the literature compared by group.
Discussion
The goal of our review was to identify factors involved in gastrostomy tube placement decisions for individuals with serious illnesses. Although there are some common factors, there are also differences in the goals, concerns, and considerations of patients, caregivers, and healthcare providers. Our results highlight key factors that may assist in centering patient preferences when making decisions related to gastrostomy tubes. Moreover, we identified several critical areas where further research is needed to enhance decision-making practices surrounding gastrostomy tube placement.
Gastrostomy tube-related decisions are complex
Our findings highlight the fact that for people living with serious illnesses who develop dysphagia, the decision to have a gastrostomy tube placed is influenced by many internal and external factors. Both healthcare providers and caregivers are frequently involved in the decision-making process and bring with them a unique set of perspectives to the decision, contributing to the large range of considerations one must reflect upon when making this decision.
As such, it is not surprising that current research indicates that patients often feel that they are excluded from medical decisions, 76 that doctors often fail to communicate adequate information, 77 and that medical information can be difficult to understand. 78 Shared decision-making is a collaborative process between patients, caregivers, and healthcare providers that encourages patients to actively weigh the risks and benefits of a treatment and match it to their personal preferences. 79 Implementing tools to help facilitate shared decision-making in gastrostomy tube-related decisions may improve decision quality, support patients in deciding the means of treatment, and address commonly reported barriers to patient-centered care.
Understanding preferences for decision making is important for patient-centered care
This study defines “decisional control” as the power of the individuals responsible for ultimately deciding whether to place a gastrostomy tube. For patients, caregivers, and healthcare providers, decisional control was the most reported factor, highlighting the importance of the preferences of the gastrostomy tube decision maker. Interestingly, the literature suggests that as many as 31% to 52% of patients and caregivers prefer not to be the primary decision maker, opting instead to defer the decision to physicians, who are seen as the medical experts.18,32,63 When patients and caregivers feel that they lack sufficient information, communication, or time from healthcare providers, they may feel uncomfortable making decisions related to gastrostomy tubes.28,53,67 Therefore, it is critical that healthcare providers provide sufficient decision-related information and inquire about the preferred roles of patients and their caregivers in the decision-making process.
Extending survival is a top priority for individuals living with critical illnesses
Factors associated with extending survival were unsurprisingly a top priority for all three groups. However, it remains unclear whether gastrostomy tube placement positively impacts survival in individuals with severe illnesses. For individuals with advanced dementia, the literature clearly states that gastrostomy tubes do not extend survival. 80 For those with ALS, the findings are mixed. Some studies suggest that gastrostomy tube placement provides a survival benefit 81 while others indicate that it reduces life expectancy.10,82 For many diseases, the impact of gastrostomy tube placement on survival has yet to be studied. Research in this area is challenging due to the heterogeneity of the disease processes and the difficulty of overcoming selection bias related to gastrostomy tube placement-related decisions. Despite these barriers, more research in this area is crucial to assist individuals living with serious illnesses in making well-informed decisions aligned with their preferences.
Future directions
To facilitate shared decision-making in clinical practice, help elicit patient preferences, and increase patient knowledge surrounding medical decisions, tools such as decision aids can be used to supplement physician counseling. 83 Decision aids have been designed and implemented for >150 diseases, 84 such as dysphagia management decisions for caregivers of patients diagnosed with advanced dementia. 85 These decision aids, however, may not be suitable for individuals with other types of serious illnesses. Unlike many people living with advanced dementia who are unable to communicate their care preferences, individuals with other serious illnesses (i.e., advanced cancer, heart failure, etc.) can actively engage in the medical decision-making process. Future work focused on the development of tools such as decision aids to promote and optimize shared decision-making surrounding gastrostomy tube placement for other serious illnesses may help patients make well-informed decisions that align with their preferences.
Limitations
A limitation of our study was the exclusion of non-English studies. This may mean that our review did not fully capture the experiences of non-English-speaking individuals with serious illnesses, caregivers, or healthcare providers. Future studies should compare non-English studies with those discussed in this article to identify any differences in the feelings, perceptions, and decision-making factors among patients, caregivers, and healthcare providers regarding the use of gastrostomy tubes in serious illnesses.
Additionally, we attempted to explore these factors broadly, including studies from a range of life-limiting illnesses such as ALS, PD, dementia, and metastasized cancer. In doing so, we may not have sufficiently captured factors specific to certain diseases. Additionally, as prior knowledge was used to define an initial set of themes, some degree of confirmation bias cannot be ruled out. Future studies should investigate whether there are disease-specific goals, concerns, considerations, and decisional control factors associated with gastrostomy tube placement and use other methodologies such as unstructured interviews to confirm findings.
Conclusion
To our knowledge, this is the first study summarizing the feelings, perceptions, and decision-making factors of patients, caregivers, and healthcare providers regarding gastrostomy tube placement in individuals with serious illnesses. By understanding the similarities and differences between the three groups in these areas, we gain greater insight into the priorities of these important stakeholders. This study serves as an important first step toward improving patient-centered dysphagia management in vulnerable populations with serious illnesses.
Footnotes
Authors’ Contributions
Conception: B.J.P. and T.H.K. Data acquisition: B.J.P., T.H.K., B.A.M., and L.M. Analysis: B.J.P. and T.H.K. Article preparation: B.J.P., T.H.K., B.A.M., and L.M.
Data Availability Statement
Derived data supporting the findings of this study are available from the corresponding author upon request.
Funding Information
This work was funded by a grant from the NIH National Institute of Neurological Disorders and Stroke (Grant Number K23NS123369; principal investigator: B.J.P.). B.J.P. receives research and salary support from the NIH National Institute of Neurological Disorders and Stroke (Grant Number K23NS123369) and salary support from MGH Institute of Health Professions. T.H.K. receives salary support from MGH Institute of Health Professions. B.A.M. receives salary support from Massachusetts General Hospital, Patient Centered Outcomes Research Institute (PCORI) (Grant Number IHS-2022C1-26100), and the American Board of Internal Medicine (ABIM). L.M. receives salary support from MGH Institute of Health Professions.
Author Disclosure Statement
No competing financial interests exist.