
Abstract
Background:
Access to timely, age-appropriate palliative care services and end-of-life communication are two standards of care for adolescents and young adults (AYAs) living with cancer where cure is uncertain or unlikely. Health professionals’ capacity to facilitate these standards is critical. This study aimed to understand AYA oncology health professionals’ experienced practices in, and barriers to, delivering these standards of care across palliative care and end-of-life communication in Australia, New Zealand, and the United Kingdom (UK).
Procedure:
We invited health professionals to complete a survey examining access, barriers to, and practices around these standards of care. Tailored to local settings, our survey assessed current delivery of palliative care and end-of-life communication services (including advance care planning [ACP]) and barriers to implementation of these.
Results:
In total, 148 interdisciplinary health professionals participated (89% female overall; 83% female in Australia, 88% female in New Zealand, and 98% female in the UK). Across countries, participants reported that most institutions had an AYA cancer program (74% overall). Introduction to palliative care services was most often prognosis dependent or “not at any uniform time.” ACP was less frequently introduced than palliative care. The most endorsed barrier to palliative care team introduction, as well as ACP, was “some team members not knowing how to introduce the topic.”
Conclusions:
Our results indicate that there are common barriers to AYAs receiving palliative care, end-of-life communication, and ACP. Given that health professionals’ confidence in this area can enable facilitation of early, age-appropriate communication, resources and training are urgently needed to bridge these practice gaps.
Key Message
Palliative care services and end-of-life communication are standards of care for adolescents and young adults (AYAs) living with cancer. Across Australia, New Zealand, and the United Kingdom, common barriers exist to AYA care meeting these standards. Training for health professionals to facilitate optimal communication is needed to bridge these gaps.
Introduction
Despite medical advances, 12–20% of adolescents and young adults (AYAs) aged 15–39 years 1 with cancer die within 5 years of diagnosis.2–4 These rates are likely an underestimate when mortality due to secondary, recurrent, and life-threatening late effects are taken into account. 5 In 2019, ∼396,000 AYAs aged 15–39 died from cancer worldwide. 6
Palliative care, including end-of-life care, is a vital consideration for this group. Palliative care is a holistic, interdisciplinary approach to supporting quality of life that aims to address the physical, emotional, social, and spiritual aspects of living with a serious illness.7,8 Contrary to misconceptions that palliative care concepts are about death and dying, palliative care can lead to better psychological, quality of life, and medical outcomes for young people irrespective of prognosis.7,9,10 End-of-life care involves treatment, care, and support for people who are thought to be in the last year of life and can involve psychosocial domains such as assistance in attainment of meaning and maintenance of relationships at the end of life.11,12
For AYAs with potentially incurable cancer, end-of-life communication, including advance care planning (ACP), is also important. ACP involves planning for one’s future health care, including preferences regarding end-of-life medical care and decision making as well as how the patient prefers to be supported while living with a serious illness and how they want to be remembered if they die. 13 ACP tools can facilitate this process and support the goals and preferences of the AYA and their family, even as their physical functioning and ability to voice their own wishes decline.
International work by the collaborative Standards for Psychosocial Care of Children with Cancer and Their Families Workgroup (hereafter, the Standards Workgroup) determined that access to palliative care should be standard for children and adolescents with cancer.14,15 Following rigorous synthesis of international evidence, their best-practice standards of care for end-of-life communication stated that “Youth with cancer and their families should be introduced to palliative care concepts to reduce suffering throughout the disease process regardless of disease status,” (hereafter, Standard 1) and “When necessary youth and families should receive developmentally appropriate end of life care” (Standard 2). However, early evidence across several countries indicates that these two standards are likely not implemented well across oncology centers.16–18 Further, most children and young people were not being introduced to palliative care concepts routinely (Standard 1), nor were they receiving developmentally appropriate end-of-life care (Standard 2).16,17 Data also highlight that when end-of-life conversations do occur with AYAs, they often happen too late.19,20
We currently know little about whether and how these two standards of care are implemented beyond the United States. Understanding the state of current practice—including barriers to these standards of care—is critical to informing how the palliative care standards might be implemented more equitably in the future. International collaboration is needed to further understand this problem. 21 The Global Adolescent and Young Adult (AYA) Cancer Accord Alliance (a tri-partite international alliance comprised of three AYA cancer-focused organizations: Canteen Australia, Teenage Cancer Trust, and Teen Cancer America) funded our international collaborative group (The Global AYA Cancer Accord End-of-Life Study Group) to empirically address this gap by examining palliative care provision for AYAs with cancer in several regions within the Alliance: Australia, New Zealand, and the United Kingdom. We aimed to build upon work describing the provision of palliative care services for young people in other Global AYA Accord regions (i.e., USA, Canada, Europe, and Asia). 22 We devised three research questions:
According to health professionals providing care to AYAs with cancer,
Methods
Sample
We recruited interdisciplinary health professionals who self-identified as having treated at least one AYA-aged patient who had died from cancer. Reflective of local practices, the age ranges used were 15–25 years in Australia and New Zealand and 12–39 in the United Kingdom.1,21 An online survey link was distributed to health professionals from these three regions through emails to 14 professional organizations (Supplementary Data S1), social media, and via snowball sampling through our 26 investigators. Informed consent was obtained prior to participation. Ethical approval was provided by the South Eastern Sydney Local Health District Human Research Ethics Committee (Reference number 18/104) and the University of Southampton Faculty of Environmental and Life Sciences Ethics Committee (Reference number 52885). The Health and Disability Ethics Committees (New Zealand) determined that further review in New Zealand was not required.
Measures
Our survey was adapted from a U.S. cross-sectional survey about the palliative care domains determined by the Standards Workgroup 22 The 54-item survey contained fixed-choice and open-ended questions about: participants’ demographics, the availability, makeup and format of palliative care (relevant to Standard 1: palliative care) and ACP services (relevant to Standard 2: end-of-life communication) for AYAs in their setting, age of teams (when established), demand for services (patient volume), frequency/timing of patients’ introduction to these services, as well as the existence of routine palliative care referral timepoints (sometimes called “referral triggers”). We also asked about barriers to delivering these two standards of care, and whether the barriers were experienced personally by respondents and/or observed in other team members. In consultation with local investigators, we piloted and edited the survey to ensure its suitability in each country. This resulted in slight differences between each country’s survey (e.g., terminology regarding “private” health facilities; full surveys can be shared upon request with the authors).
Data collection and analysis
Participants completed the survey online through QualtricsTM. In line with best practice approaches, 23 we verified that our survey data represented unique data from humans (rather than bots) by checking our data for open-ended response content, completion time, and repetitive IP addresses. We analyzed data using SPSS v27, using descriptive and univariate statistics to describe the sample, including frequencies, means, standard deviations, and ranges. Due to missing data, all percentages use the total number who answered the question as the denominator. In analyzing data related to health care services available in different palliative care programs, we used weighted averages to account for the relative importance (weight) of scores in the dataset, therefore considering how often a service was more frequently used and reflecting the relative importance of the responses.
Results
Participant characteristics
We recruited 148 interdisciplinary health professionals (Australia n = 71, New Zealand n = 34, and UK n = 43, total n = 148). No apparent instances of bots submitting data were identified. We were unable to calculate a response rate due to the use of open advertisements in recruitment. Our sample was mostly female (89%), with varying professional experience (range: 1–43 years; SD = 9.7; Table 1) and nurses being the largest subgroup. Participants described working in settings where their AYA cancer services generally operated outpatient and hospital-based clinic consultations and consultations in the home setting (reported by 77.9% and 68%, respectively), while it was less common for settings to have dedicated inpatient beds for AYAs (31.2%).
Characteristics of Health Professional Survey Respondents and Their Health Setting Contexts
Other included pediatricians, occupational therapists, medical trainees, radiation therapists, leisure therapist, exercise physiologist, general practitioners, emergency specialists, and other support workers.
Multiple answers permitted.
Other included nongovernment organizations and private practice.
Item not included in UK survey due to local health professionals considering it inappropriate for UK setting.
Other included nongovernment organizations, community organizations, and charities.
AYA, adolescent and young adult; SD, standard deviation.
Research question (RQ) 1: What palliative care services are available for AYAs with cancer in their setting?
Most participants reported that their center had an AYA palliative care program cancer patients could access (74%). The largest subset of participants reported that palliative care services were being delivered to AYAs by adult services (41%), followed by pediatric services (29%) and AYA-specific palliative care programs (12%). A minority of participants reported that no palliative care services were available for AYAs in their workplace (11%). For those who reported access to AYA palliative care programs, most reported that service capacity matched demand (69%), with some reporting that the demand exceeded their capacity (19%).
Table 2 details how characteristics of AYA palliative care programs varied (Supplementary Data S2 depicts country-specific data). The top three health professionals available within palliative care teams were physicians, registered nurses, and social workers. Only two services—symptom management and ACP—were reportedly used “often.”
Characteristics of Palliative Care Programs
Other included emergency specialist, exercise physiologist, general practitioner, occupational therapist, and radiation therapist.
For the UK survey, this item was split into two, of which one item regarding community hospice care generated 66.7%, and one item regarding community care through a community team generated 70.4%.
Items not included in survey adapted for UK settings, based on local health professional guidance, n = 49.
The weighted average takes into account the relative importance (or weight) of scores in the dataset. Here, we have scored “infrequently used” responses as one, “Sometimes used” as two, and “Often used” as three and reported the average of these scores. These weighted averages therefore take into account how often a service was more frequently used, reflecting the relative importance of the responses.
Item not included in UK survey due to error.
AYA, adolescent and young adult.
RQ2a: How, and when, is palliative care typically introduced?
Participants described the frequency of AYAs’ introduction to palliative care concepts and the general timepoint of these topics being introduced (Fig. 1). Almost half (46%) reported that palliative care concepts were “usually” or “always” introduced regardless of disease status (Supplementary Data S3: country-specific data).
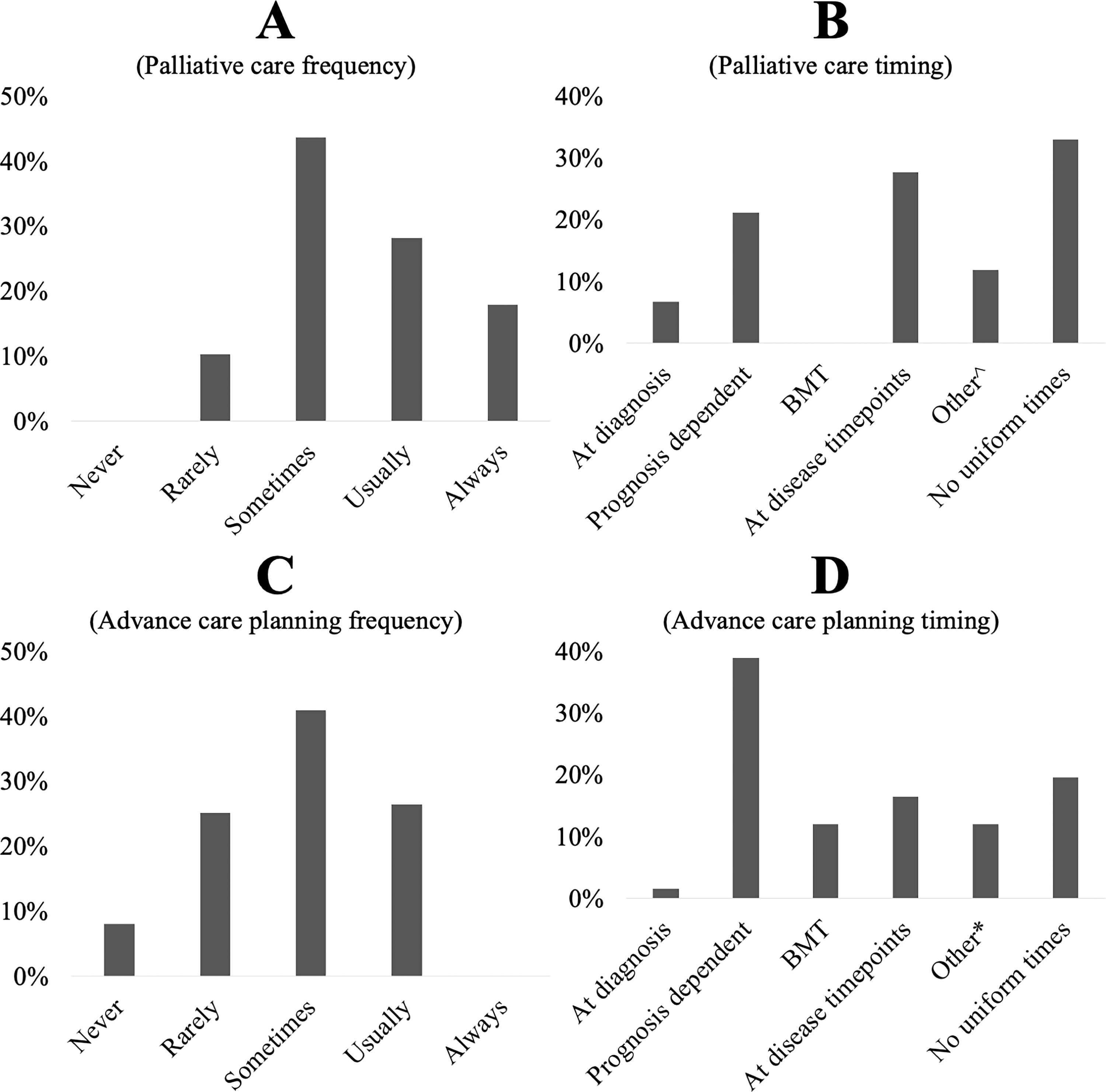
Frequency and timing of access to palliative care concepts and advance care planning tools for adolescents and young adults (AYAs) with cancer and their families.
Routine palliative care referrals were reported by just under half of our sample (45%), who reported that the most common scenario where routine referrals occurred was for new cancer diagnoses with an estimated prognosis less than a certain percentage (Fig. 2; country-specific data presented in Supplementary Data S4).

Routine referral scenarios for palliative care and advance care planning tool introduction for adolescents and young adults with cancer and their families.
RQ2b: How, and when, are ACP tools typically introduced?
Compared with palliative care referrals, it appeared less common for there to be scenarios where ACP tools were routinely introduced to AYAs and their families (Fig. 2). While 45% of participants had endorsed the presence of routine scenarios that would prompt a palliative care referral, only 28% participants identified routine scenarios for the consideration of ACP tools. The nature of scenarios where ACP tools were routinely considered also differed to palliative care referrals generally, with the most common scenario where ACP tools were routinely considered was for patients with “Difficult to manage symptoms or high symptom burden” (36%), followed by patients with a “Diagnosis of refractory disease” (33%).
RQ3a: What barriers to palliative care do health professionals perceive?
The top five most endorsed barriers were “Some team members not knowing how to introduce the topic” (72%), “Parental negative perception of palliative care” (72%), “Some team members not wanting to diminish hope” (66%), “Patient negative perception of palliative care” (59%), and “Late referrals” (59%). All barriers listed in the survey were endorsed by at least 22% of respondents (Table 3; country-specific data in Supplementary Data S5).
Barriers to the Introduction of (A) Palliative Care and (B) Advance Care Planning Tools with AYAs with Cancer and Their Families
Participants were asked to endorse all perceived barriers, and so percentages do not sum to 100%. n = 65 total responses to the palliative care item, n = 67 total responses to the advance care planning (ACP) item.
Denotes the five barriers chosen most frequently as participants’ single-most impactful, top barrier to the introduction of palliative care.
Denotes the five barriers chosen most frequently as participants’ single-most impactful, top barrier to the introduction of ACP tools.
N/A, not applicable, item not included with relation to ACP tools.
AYA, adolescent and young adult.
Across barriers, participants tended to report that they observed these barriers more frequently in others than personally in their own practice (Fig. 3).

Barriers to palliative care for adolescents and young adults with cancer, and whether barriers are perceived as personal or observed in others.
RQ3b: What barriers to ACP tool use do health professionals perceive?
All barriers were endorsed by at least 22% of respondents (Table 3), with the five most commonly endorsed barriers being “Some team members not knowing how to introduce the topic” (67%), “Some team members not being aware of the benefits of ACP tools” (52%), “Some team members not being aware of the scope of ACP tools” (51%), “Some team members not wanting to diminish hope” (49%), and “Parental negative perception of ACP” (49%).
As with barriers to introducing palliative care, participants reported more frequently that barriers to using ACP tools were observed more in others than experienced personally (Fig. 4, country-specific data Supplementary Data S6).

Barriers to advance care planning (ACP) tool use for adolescents and young adults with cancer, and whether barriers are perceived as personal or observed in others.
Discussion
Our survey of 148 health professionals from Australia, New Zealand, and the UK found that consistent with U.S. data, 22 interdisciplinary palliative care services were available to AYAs in most settings, however, few specialist palliative care services were available. Despite this access, health professionals reported that only two services—symptom management and ACP—were used “often” in their setting. This suggests that while palliative care is not synonymous with end-of-life care, it may still be primarily used in this way. Other services, including counseling and rehabilitation-oriented therapies such as occupational, physical, and child life therapies, were used less frequently (although it is unclear whether this is due, at least in part, to the limited availability of these services). These lesser-used services may also require timely introduction (i.e., when a patient is still relatively well and able to engage with these therapies) to yield the greatest benefit to quality of life over a longer period. 24 Differences in the relative usefulness of some services for older AYAs (e.g., child life therapies for >18-year-olds) may also impact their uptake. As more AYAs live longer with uncertain or poor-prognosis cancers, 25 this finding is suggestive of missed opportunities to utilize the full interdisciplinary team to maximize quality of life.
Health professionals most often reported that there were “no uniform times” that palliative care was introduced. Given that specialist palliative care is often introduced for AYAs too late, or not at all,26–29 it is important to consider whether systematic approaches might prompt timelier palliative care. We found routine palliative care referrals were somewhat less likely to be used compared with the U.S. data (45% vs. 56%). 22 This accords with research showing routine referral procedures do not consistently translate into palliative care referrals. 30 However, our findings stand in contrast with Weaver and colleagues, 22 who found that sites with routine referral procedures were 3.4 times more likely to introduce palliative care regardless of disease status. Symptom and quality of life profiles may prompt involvement of palliative care to benefit patients: in one recent Canadian study, AYAs whose symptoms and quality of life were routinely screened using patient-reported outcome measures in clinic were more likely to receive palliative care services, particularly when symptoms were worse. 31 Further work is needed, internationally, to better understand what models of care best support optimal palliative care service delivery for AYAs with cancer and to align workforce and service capacity to deliver these models of care. This is particularly important given known issues surrounding availability of specialist palliative care workforce 32 and training. 33 Taken together, data highlight unique benefits and potential limitations to specialist palliative care services for AYAs with cancer and suggest that integrated, multidisciplinary services may be required to meet the varied needs of this population.31,34
Our data highlight that communication of palliative care concepts continues to challenge health professionals. Less than half our sample reported that palliative care concepts were usually/always introduced to AYAs. Barriers cited by health professionals were predominantly emotional and interpersonal in nature. “Some team members not knowing how to introduce the topic” was the top-ranked barrier to introduction of palliative care concepts in general, and ACP conversations in particular. Other strongly endorsed barriers included fears about parents', or patients', negative perceptions of palliative care, and concerns that introducing palliative care might diminish hope. These findings reflect challenges navigating relational aspects of palliative care communication and speak to the emotional burdens involved for health professionals in guiding these conversations. Palliative care conversations are emotionally challenging even for experienced health professionals, and supporting the dual processes 35 of hope-driven living, and illness-orientated planning, is a nuanced balance to strike. Training approaches drawing on the expertise of wider interdisciplinary teams, 33 and involving psychologists and social workers in particular,37,38 will be important for training that can target these relational skillsets.
Formal ACP tools can help enable end-of-life conversations to occur. 39 Our data highlighted, however, that health professionals felt that their team was typically unaware of the scope of ACP tools. Training may be needed to support health professionals to gain an in-depth understanding of how these tools can support AYAs’ quality of life across the care trajectory. For example, the Voicing My Choices ACP communication guide supports AYAs to consider and express their preferences on topics including social and family support, meaningful activities, and considerations regarding legacy postdeath. 40 Data show that this tool reduces AYAs’ anxiety around end-of-life planning. 13 Researchers are also examining the potential for Voicing My Choices to be integrated within a resilience-building intervention for AYAs during cancer treatment. 41
We found that health professionals consistently perceived palliative care communication barriers as more problematic for their team members than for themselves. This is consistent with research finding that health professionals believe resources to aid in health-professional-to-parent communication would be useful for junior staff but not for themselves.42,43 Notwithstanding participant self-selection, this pattern may reflect an “optimism bias,” 44 whereby health professionals overestimate the likelihood of these barriers occurring for others while also underestimating the extent to which they applied to themselves. This could also impact whether health professionals engage with further training on this topic.
Limitations
While our cross-sectional, online survey methodology offers a snapshot of current practices at a broad scale in Australia, New Zealand, and the United Kingdom, several limitations warrant acknowledgment. First, we were not able to calculate a precise response rate, and we did not require participants to name their setting, so it is not possible to link our findings to specific sites. Second, due to the variability of the services examined, we could not unpack determining factors for service availability and practices. Future research should build on these findings using prospective designs where greater causality may be attributable to different service and clinical practice factors. Lastly, our sample represented a mix of disciplines and clinical experience—a strength given the study was undertaken early in the COVID-19 pandemic (the survey was open and recruited from different avenues across March 2019 to December 2020). However, the pandemic may have disproportionately affected some health professionals’ capacity to participate. For instance, our sample appears weighted toward female nursing practitioners from relatively lower-volume sites (<50 AYAs/year). As such, our pragmatic recruitment approach, which relied upon participant self-selection, means our findings may not represent broader trends in AYA oncology in the countries surveyed. Further investigation in this area should build upon these methods and look to benchmark current practices and service capacity using consensus-based international collaborations, including exploring the utility of validated instruments.
Future directions
This study needs replication in lower- and middle-income countries and in populations speaking a language other than English, where other barriers to the integration of palliative care may exist. 45 Further research is also needed spanning the AYA age range internationally—and looking at how palliative care is implemented in adult compared with pediatric settings. Gaps also remain in understanding how these standards might be implemented for AYAs as cancer care trajectories become increasingly personalized with precision therapies uncertain prognoses.25,46 Future research addressing these questions to include AYA patients’ and families’ voices using participatory methodologies will be critical. 34 ,54 Directly including AYAs in codesigning health-system change initiatives will be crucial to narrow these practice gaps in person- and family-centric ways.
Conclusion
While age-appropriate palliative care appears mostly accessible, palliative care referral “regardless of disease status” remains far from routine for AYAs in Australia, New Zealand, and the United Kingdom. Attention is needed to address several key barriers to health professionals’ capacity to deliver optimal palliative care and end-of-life communication to AYAs with cancer in these countries.
Footnotes
Acknowledgments
In addition to the named authors, The Global Adolescent and Young Adult Cancer Accord End-of-Life Study Group also included, Afaf Girgis, Ahmed Al-Awamer, Anne Kirchhoff, Celeste Phillips, Douglas Fair, Hanneke Poort, Fiona Schulte, Jennifer Mack, Joan Haase, Karen Wernli, Leigh Donovan, Pamela Mosher, and Susan Trethewie. This work was supported by the Inaugural AYA Psycho-Oncology Research Acceleration Grant (2018–2020) funded by the Adolescent and Young Adult Cancer Global Accord, an international alliance comprised of Canteen Australia, Teen Cancer America, and the Teenage Cancer Trust. U.S.D. wishes to thank the AYA Cancer Global Accord mentors who provided helpful guidance in the development and undertaking of this study, in particular Prof Pandora Patterson and Dr Fiona McDonald (Canteen Australia), Prof Dan Stark (University of Leeds, UK), and Dr Norma D’Agostino (Princess Margaret Cancer Center, Canada), and Prof Bradley Zebrack (University of Michigan, USA).
Authors’ Contributions
Conceptualization: U.S.D., H.E., A.S.D., M.S.W., A.R., L.W., A.A., L.S., M.C., R.F., A.H., T.L., R.C., and C.W. Methodology: U.S.D., H.E., A.S.D., M.S.W., A.R., L.W., A.A., L.S., M.C., R.F., A.H., T.L., R.C., and C.W. Software: U.S.D. and H.E. Validation: U.S.D. and H.E. Formal analysis: U.S.D. and H.E. Investigation: U.S.D. and H.E. Resources: U.S.D. and H.E. Data curation: U.S.D. and H.E. Writing—original draft: U.S.D. and H.E. Writing—review and editing: All. Visualization: U.S.D. and H.E. Supervision: U.S.D., H.E., L.W., and C.W. Project administration: U.S.D., H.E., M.C., L.W., A.R., M.W., A.S.D., and L.S. Funding acquisition: U.S.D., H.E., A.S.D., M.S.W., A.R., L.W., A.A., L.S., R.F., A.H., T.L., R.C., and C.W.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
U.S.D. was supported by an Early Career Fellowship from the Cancer Institute of New South Wales (ID:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.