
Abstract
Having a family member hospitalized in the intensive care unit (ICU) can be a stressful experience for family members, encompassing both psychological and spiritual distress. With over 5 million ICU admissions annually in the United States, it is imperative to enhance the experiences and coping mechanisms of ICU family members. In particularly challenging situations, some family members even face psychological effects known as post-intensive care syndrome—family, which includes anxiety, depression, and posttraumatic stress. The distress may be worsened when patients and families experience poor communication or medical care, which has been shown to be more common among minoritized populations including Black and Hispanic patients and families. Family members’ emotional and spiritual distress also has an effect on the medical decisions they make for the patient. While research has delved into the impact of spiritual care for ICU family members, further investigation is still needed to determine the most effective approaches for delivering such care. This narrative review will describe a conceptual model aimed at guiding future research in this endeavor. The model proposes that chaplains provide emotional, spiritual, and information support to ICU family members. This affects both their ICU experience, decision making, and outcomes for the patient and family. This process is also affected by characteristics of the family such as race, ethnicity, and economic status. This model helps identify gaps in research, including the need for randomized trials of spiritual care that identify mechanisms underlying outcomes and demonstrate impact of spiritual care, and consider race, ethnicity, and other characteristics.
Introduction
An intensive care unit (ICU) admission represents a significant life crisis that often triggers profound distress for the patient’s family, both during and after hospitalization. This psychological distress has been labeled as post-intensive care syndrome—family (PICS-F), encompassing symptoms such as anxiety, depression, and posttraumatic stress. 1 Research indicates up to one-third of family members of all ICU patients are affected, with rates increased to one-half, if family members also serve as a surrogate decision maker or if the patient dies. 2 Considering over 5 million ICU admissions occur annually in the United States, the extent of psychological suffering among family members is substantial. 3
There is also evidence ICU family members experience religious and spiritual (R/S) distress, a closely related but distinct dimension of distress that has received less attention.4–6 R/S distress also affects medical decision making, and R/S support may influence the outcomes of decisions such as preferences for and even receipt of comfort care at the end of life.7–9 Medical decision making involves an interaction of cognitive and emotional processes, and chaplains have specialty training and clinical experience in addressing these processes.10,11 However, the existing evidence suggests chaplains’ spiritual care is inconsistently available in the ICU setting.12,13
Experiences in the ICU of serious illness, mortality, and grief are also affected by an individual’s R/S, culture, and other social factors, including beliefs about death and dying, the nature of suffering, or the use of rituals and practices. Race and ethnicity also have effects on the ICU experience due to differences in culture and beliefs and historical inequities.14–16 Inequities in health outcomes for Black and Hispanic patients have been well documented in the United States and contribute to increased life-threatening illness and mortality.17,18 Black and Hispanic patients experience lower quality serious illness communication, with fewer goals of care conversations and less prognostic communication.19,20 Attention to these factors in medical care has been shown to improve outcomes for patients and families.21,22
This narrative review will describe research on the psychological and R/S distress of ICU family members and the spiritual care available to them. We will then recommend a conceptual model to guide future research about the role of spiritual care in addressing ICU family distress, including a description of the research that supports the model’s elements.
Establishing a clear and empirically supported definition of spirituality is necessary for advancing research. An international group of palliative care experts proposed the following definition, which identified several key domains of spiritual experience:
Spirituality is a dynamic and intrinsic aspect of humanity through which persons seek ultimate meaning, purpose, and transcendence, and experience relationship to self, family, others, community, society, nature, and the significant or sacred. Spirituality is expressed through beliefs, values, traditions, and practices. 23
This definition is consistent with the training and standards of practice of chaplains.24,25 Board-certified health care chaplains are highly trained professionals equipped to provide R/S and emotional support to patients and family members with diverse R/S backgrounds as well as those without any religious affiliation. 25 Chaplains have extensive training including a master’s degree and a year of clinical pastoral education training (similar to an internship/residency). They are trained to listen deeply to the individual to address diverse R/S concerns and respond to the person’s needs. Proselytizing about one’s faith or personal beliefs is a violation of chaplain ethics. 11 Chaplains also are trained to address aspects of R/S that have been shown to affect medical decision making, positioning them to support the decision-making process in collaboration with the health care team. Given their rigorous training, chaplains possess pertinent yet often underutilized skills to address family members’ ICU-related distress.
The Gap Between ICU Family Members’ Needs and ICU Spiritual Care
A family member’s experience of an ICU stay can be stressful and traumatic. The term PICS-Family describes this psychological distress and includes depression, anxiety, and peri- and posttraumatic stress.1,26 Family members may also experience complicated grief if the patient dies.1,2,27 These symptoms are persistent for at least 24 months in a subset of people. 28
Research about ICU family members’ R/S concerns and distress is limited, but some key features are emerging. One study conducted interviews with family members of ICU patients who were close to death or for whom a decision to withdraw advanced life support had been made. 4 Four broad spiritual themes were identified, including (1) comfort and peace, (2) connections and reconnections, (3) personal tributes, and (4) spiritual rituals and practices. In another study, family caregivers described spiritual distress as suffering related to a loss of meaning, purpose, and connection. 5 Other elements of their spiritual distress included questioning core beliefs about life and death and feelings of guilt or regret in the relationship with their family member.
There are validated measures of spiritual distress that can be useful in ICU family research. Several of these constructs are included in the functional assessment of chronic illness therapy—spiritual well-being scale, a widely used measure of spiritual well-being that addresses three dimensions: peace, meaning, and faith. 29 A measure has also been published that addresses the spiritual construct of peace with the single item, “Are you at peace?” 30 A related concept is spiritual pain, validated as a single item phrased similarly to other items on the Edmonton Symptom Assessment Scale.31,32 This item asks the patient to rate spiritual pain, defined as “a pain deep in your soul/being that is not physical.” This single-item spiritual pain measure has been validated in caregivers of patients with advanced cancer in the outpatient setting. The Religious and Spiritual Struggles scale measures three broad types of R/S struggle: intrapersonal, interpersonal, and divine. 33
Recognizing the importance of spiritual care in addressing the R/S and emotional distress of ICU patients and their family members, expert panels have published clinical guidelines for spiritual care in the ICU. One 2003 panel identified spiritual support as one of the crucial domains of end-of-life care and outlined three quality indicators: (1) continuously assess and document the spiritual needs of both the patient and family, (2) facilitate access to spiritual resources, and (3) encourage and support spiritual and cultural practices that provide comfort to the patient and family. 34 After conducting an extensive literature review another expert panel published clinical guidelines for family-centered ICU care that emphasize spiritual support from a spiritual advisor or chaplain to meet the expressed desire for spiritual care among families. 35 Another team utilized a Delphi process to develop a clinical guide for ICU clinicians in identifying family members experiencing spiritual distress and initiating conversations about spiritual needs. 36
A recent JAMA systematic review highlighted the significance of R/S considerations for patients with serious illnesses and their family members. 22 Based on existing empirical evidence, this expert panel recommended routine incorporation of spiritual care into the medical care of patients with serious illnesses and involvement of specialty practitioners of spiritual care, such as chaplains, in their treatment. While the review included research on family caregivers, the recommendations focused on patients themselves and their families. As important as these guidelines are, it should be noted they do not address the specifics of best-practice spiritual care for families of patients with serious illness or in the ICU.
Despite the importance of spiritual care for patients and families in the ICU, research indicates many do not have access to a chaplain during their ICU stay, or only encounter one when the patient is nearing death or has already died.12,13 Studies have revealed significant variability in the frequency of chaplain involvement. One study analyzed the records of 4169 patients admitted to ICUs in a single medical center over a six-month period and discovered only a small proportion of these patients (5.9%) had documented chaplain visits, with the majority of these visits at the time of death. 13
In a retrospective chart review of 254 patients who died in one of 4 U.S. medical ICUs or were discharged to hospice, our team found that 78% of the patients or family members received some spiritual care; the proportion receiving spiritual care increased as the patient’s neared death or discharge. 12 Emotional and spiritual support was provided in the majority (77%) of the chaplain visits. Only 15% of the chaplain visits included decision-making support, such as participation in family meetings or goals-of-care conversations. We found that receiving chaplain visits was associated with greater ICU length of stay. 37 Longer stays may have provided a greater opportunity for receiving spiritual care. 38
Another study audio-recorded ICU family meetings and found chaplains were included in only 2 of 249 ICU family meetings. 39 Though R/S concerns were raised in 40 of 249 meetings, usually by the family, in most cases, the clinician did not respond to the concern. This study demonstrates that R/S is rarely addressed by the rest of the ICU team. Some of the variation in the frequency of spiritual care provided by a chaplain may be explained by the chaplain’s incorporation into the ICU team.
Research to Support ICU Spiritual Care: Recommendations and Conceptual Model
In light of the gap between ICU family needs and current ICU spiritual care practice, we recommend research that will support more consistent provision of spiritual care for ICU patients and their families. We propose a conceptual model to guide that research; the model describes how spiritual care contributes to family members’ ICU experience and associated outcomes. The model also considers how other family characteristics, such as religion, race, or ethnicity, contribute to the ICU experience and outcomes.
Our prior conceptual work and empirical research have led to the development of a model proposing that clinician communication involves the domains of information, emotional support, and spiritual support.40,41 These domains affect the surrogate’s experience in the ICU, including their coping and distress, and their decisions about the patient, particularly highly charged medical decisions about life and death. These processes affect surrogate outcomes such as long-term psychological and spiritual well-being as well as patient care, especially near the end of life. 42 While the prior model applies to family communication generally, our present model focuses on the provision of spiritual care to the ICU family. This spiritual care is primarily provided by chaplains, who are the experts in spiritual care, although other clinicians are able to provide basic forms of spiritual support (Fig. 1).24,43
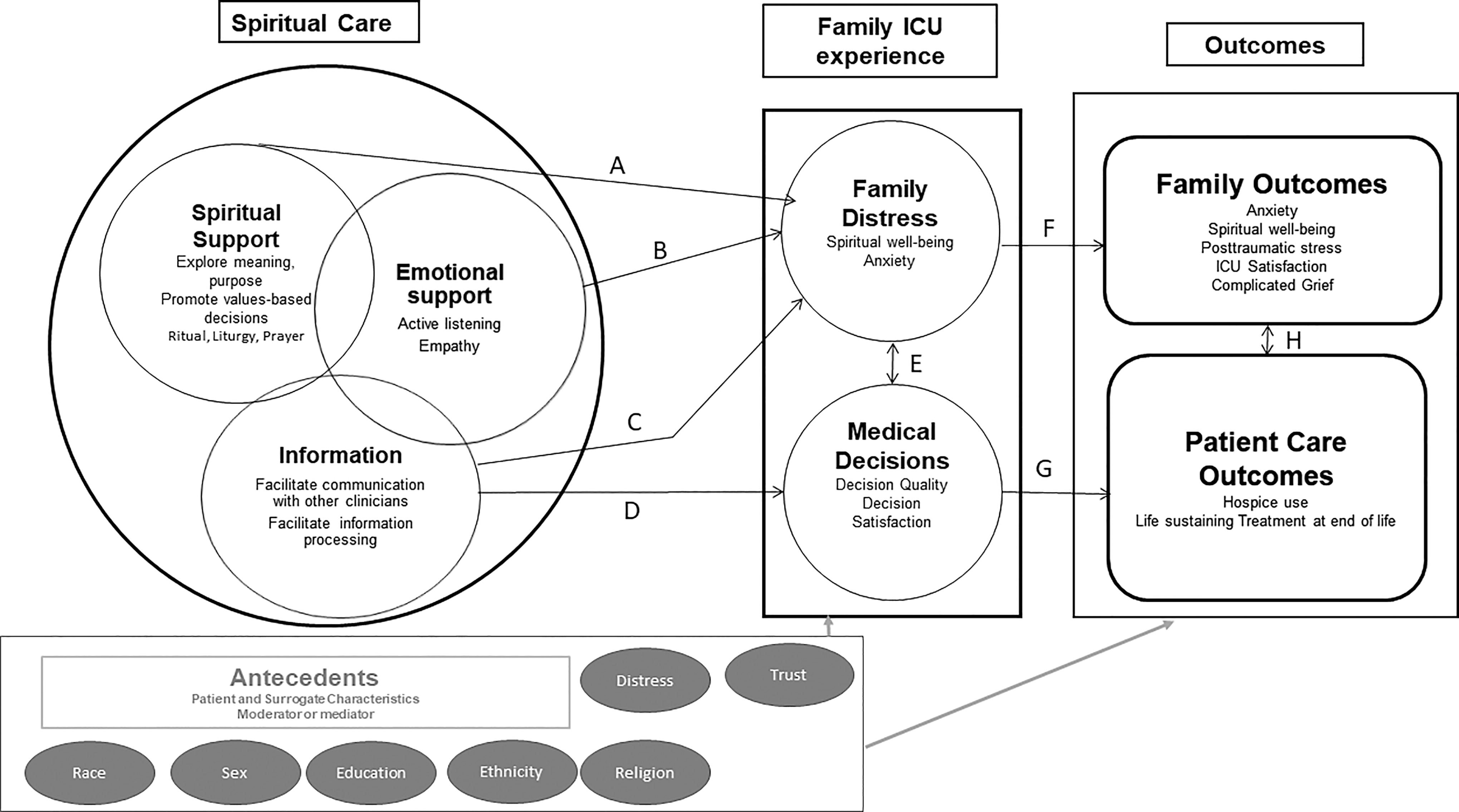
Conceptual model showing the impact of spiritual care on the family intensive care unit (ICU) experience and patient/family outcomes.
Prior conceptual work on surrogate decision making in the hospital identified two core dimensions of communication: information, and emotional/spiritual support. 40 These two distinct dimensions were confirmed using factor analysis during development and validation of a survey of clinician-surrogate communication. 41 This observational data also showed that emotional and spiritual support provided by the health care team is associated with lower anxiety, depression, and posttraumatic stress for the surrogate when measured—six to eight weeks after hospital discharge. 42 We hypothesize that both spiritual and emotional support lower the distress that families experience in the ICU (Fig. 1, arrows A and B), leading to better long-term family outcomes (Fig. 1, arrow F). While this analysis combined emotional and spiritual support, spiritual care theory and research can further refine the model by distinguishing features of emotional and spiritual distress and support.44,45 Emotional distress includes concepts such as anxiety, depression, and posttraumatic stress and is directly supported by interventions such as expressions of empathy. R/S distress includes crises of meaning and concerns with the sacred or transcendent and can be addressed by exploring questions of meaning and purpose or providing rituals, liturgy, or prayer. 46
The relationship with information seems to be more complicated. Our research found that the quality of information is associated with better ratings of decision making by surrogates (Fig. 1, arrow D). However, when controlling for emotional support, higher ratings of information were associated with higher posttraumatic stress scores (Fig. 1, hypothesized to act through arrows C and F). 42 This unexpected finding suggested that information without emotional support may worsen stress. 42 An early trial in the ICU found that a communication intervention involving a family meeting and a brochure resulted in reduced posttraumatic stress symptoms and had an effect on care at the end of life. 47 However, a systematic review of ICU interventions showed that while most studies affected medical care, especially at the end of life, most did not have an effect on psychological outcomes, 48 and in one study posttraumatic stress was higher in the intervention group. 49 One intervention directly focused on addressing avoidance and providing coping tools showed promise in a pilot study, suggesting targets for future support interventions. 50
Another possible explanation is that the way information is presented may affect decision making and outcomes. Most information about the medical condition is delivered by physicians and nurses. However, chaplains may be especially well suited to support the family in processing the information and coping with its emotional impact, reducing family distress (Fig. 1, arrow C). As information increases, so does the emotional and spiritual support needed to parse the meaning of the information. 42 When an information deficit exists, the family’s sense of uncertainty and vulnerability makes emotional and spiritual support important for coping. 51 A chaplain caring for a family may address information deficits or gaps by communicating with the interdisciplinary team and advocating for additional information. 12
Two studies demonstrate how ICU chaplains’ activities align with the three domains outlined in our conceptual framework: information, emotional support, and spiritual support. One study described chaplain activities for 254 patients in the medical ICU and their caregivers, which are provided in Table 1. These activities have been categorized according to the three domains in our conceptual model. In this sample, chaplains delivered R/S and emotional support in 76.7% of cases, while providing information and decision-making support in 14.8% of cases. 12
Spiritual Care Activities for Medical Intensive Care Unit Patients and Family Caregivers, Categorized by Domain of Religious or Spiritual Support a
Data from Labuschagne et al. 12
In total, 485 chaplain visits with 254 MICU patients and family caregivers.
E, emotional; I/DM, information and decision making; MICU, medical intensive care unit; R/S, religious/spiritual.
A separate investigation focusing on chaplain care and family satisfaction with ICU care and decision making presented a table delineating chaplain activities (see Table 2). 52 Once again, these activities were categorized according to the three domains from our conceptual model. In more than 90% of cases, chaplains provided R/S and emotional support, while in over 70% of cases, they engaged in discussions about decision making.
Spiritual Care Providers’ Self-Reported Activities a
Data from Johnson et al. 52
Activities were reported from 285 chaplain questionnaires representing 244 ICU patients.
ICU, intensive care unit.
The research about chaplains’ effectiveness in improving patient and family outcomes in general, and in the ICU context specifically, is small (arrows F and G). 53 Two studies have examined the effects of spiritual care on family members’ satisfaction with ICU care when the patient died in the ICU. Among 356 family members, ratings of satisfaction with spiritual care were positively associated with ratings of overall satisfaction with the ICU experience based on the Family Satisfaction in the Intensive Care Unit (FS-ICU) survey. 54 In the second study, greater levels of spiritual care were associated with higher satisfaction ratings with ICU decision making (Satisfaction with Decision-Making subscale) and overall satisfaction with ICU care (FS-ICU). 52 In a study of factors associated with posttraumatic stress disorder (PTSD) symptoms of 306 ICU surrogates at three-month follow-up, investigators found that surrogates’ reports of insufficient religious support were significantly associated with worse PTSD. 55
Two randomized controlled trials have examined the effects of spiritual care interventions on patient (rather than surrogate) outcomes. One found positive effects on the anxiety of hospitalized patients with chronic obstructive pulmonary disease 56 ; the other found positive effects on religious coping for coronary artery bypass graft surgery patients in a cardiovascular critical care unit. 57 One small pilot study studied a spiritual care intervention for 31 family caregivers of outpatients with advanced illness. 58 Study participants had a positive response to the intervention and there was a trend toward lower spiritual distress. A randomized trial examined the use of chaplains as ICU navigators. 59 The study relied on chaplain trainees (residents) to deliver the intervention and suffered from low fidelity. The chaplain met with fewer than half (44%) of the intervention group patients within the first 24 hours and participated in fewer than one-third (32%) of family meetings for the intervention group patients. As with the study by Labuschagne and colleagues mentioned above, 37 these investigators also found longer ICU length of stay in the chaplain navigator intervention group.
Our single-center randomized trial of spiritual care in the ICU setting provides early evidence that highly specialized emotional and spiritual support provided by chaplains can improve the long-term well-being of the surrogate. 60 At follow-up, anxiety in the intervention group was significantly lower than that of controls. The percentage of family caregivers with a clinically important change in their anxiety improvement was 65.2% in the intervention group versus 49.2% in the control group. The odds of an improvement exceeding the MCID were three times higher in the intervention group in adjusted analysis and was over three times higher for spiritual well-being. Satisfaction with spiritual care was also higher. The study sample was 21% Black but lacked religious or ethnic diversity. This study provides evidence for the effects of spiritual care on family outcomes, but more work is needed to fully elucidate the pathways proposed in our model and the effect of other social and cultural variables such as religion, race, and ethnicity (antecedents in the model).
The role of spiritual care in facilitating medical decision making in the ICU
When a patient lacks the ability to make their own medical decisions due to incapacitation, their surrogate decision maker, typically a designated family member, assumes the responsibility of making decisions that align with the patient’s values and preferences. This task is often fraught with challenges, including uncertainties about the patient’s wishes, strained family dynamics, and the emotional toll of witnessing a loved one’s illness. Making medical decisions on behalf of another individual necessitates careful consideration and the ability to navigate conflicting priorities. 61
While evidence suggests a potential link between spiritual care and medical decision outcomes, few studies have examined the effect of spiritual care on medical decisions (arrow D) and patient outcomes (arrow G). Existing research has primarily focused on broader hospital settings or patients capable of making their own decisions. One study spanning over 3000 hospitals found that institutions with spiritual care departments reported higher rates of hospice enrollment. 62 A study of patients with advanced cancer found that greater spiritual care from the medical team, including a chaplain, was associated with higher quality of life at the end of life, lower use of life-sustaining treatment at the end-of-life and greater hospice enrollment among these patients.7,63 They found that patients who received more spiritual support from their own faith communities had higher use of life-sustaining treatments at the end of life, suggesting that hospital chaplains may play a much different role in decision making than religious communities. 9 While these studies do not describe the mechanisms in the observed associations, it is possible that spiritual support from chaplains helps patients and their families cope with death and, therefore, accept comfort-focused care in a timely manner at end of life. Further research is needed to assess these associations in the ICU setting.
Spiritual and emotional support may also affect decision making through other mechanisms that are conducive to chaplain interventions (arrow D). Attending to the emotional state of the decision maker affects the decision-making process (arrow E). 64 Terror management theory proposes that awareness of death can cause intense anxiety, which can in turn lead to attentional narrowing, with reduced memory and cognitive processing.65,66 Specific communication strategies improve decision making, such as expression of positive emotions, empathy, and practicing accommodation or modifying one’s style to create connection. 64 Chaplains are highly trained in the interpersonal aspects of communication, including active listening, recognizing and responding to emotions, and in using spiritual care interventions to reduce anxiety and promote a sense of peace. These interventions have the potential to influence the cognitive processes of decision making. 46
Other researchers have examined how chaplains perceive their role in both medical decision making and advance care planning (ACP). In a survey involving 463 chaplains, with 37% of them working in ICU settings, Wirpsa and colleagues discovered that 70.6% of chaplains reported providing support to families in decision-making processes; 48% mentioned communicating patient values and beliefs to the health care team, while 42% reported assisting patients and families in clarifying factors relevant to decision making. 10 Chaplains emphasized religion’s influence on decision making, leading the researchers to develop a comprehensive five-stage model outlining the chaplains’ involvement in shared decision making: information sharing, processing, clarification, decision making, and providing support. Wirpsa and colleagues curated a book containing nine in-depth case studies supplemented with commentary, showcasing the various ways chaplains collaborate as partners in shared decision-making processes. 67 In terms of ACP, a separate study involving data from over 200 chaplains revealed that the vast majority (90%) actively assist patients with ACP, considering it a crucial aspect of their role. 68 During discussions on ACP, chaplains address patients’ hopes and fears by (1) exploring and normalizing fears, worries, and doubts; (2) engaging in conversations to integrate faith, values, and preferences into ACP discussions; and (3) providing education, empowerment, and advocacy to support patients and families through the process. 69 In the conceptual model, we propose that chaplains have a role in clarifying information with the medical team (Fig. 1, arrow D). Through decreasing spiritual and psychological distress (Fig. 1, arrows A and B), they support the family member in processing information and making decisions (Fig. 1, arrow E). This, in turn, may affect the outcomes of patient care (Fig. 1, arrow G).
The influence of family members’ prior life experience on ICU experience and spiritual care
The prior life experiences of ICU family members (Fig. 1, antecedents, gray arrows) significantly influence their ICU experience and may influence the impact of spiritual care. While numerous mediation and moderation relationships may exist between these antecedents and outcomes, we show only two representative arrows for simplicity. Two of these antecedents, race/ethnicity and R/S, may play pivotal roles in mediating or moderating the relationships between spiritual care, family members’ ICU experiences, and their long-term outcomes.
Many studies have reported associations between R/S beliefs and involvement and preferences for and receipt of more life-sustaining treatments and lower enrollment in hospice at the end of life.7,9,70 One pivotal study showed that patients with high religious coping scores had more life-sustaining treatments at the end of life compared with those with low scores (13.6 vs. 4.2%). 9 It is important to note that in this study only a minority of patients in either group received life-sustaining treatments at the end of life, suggesting that both religious and nonreligious patients are open to comfort-focused care at end of life. Our research team has measured several domains of R/S for surrogate decision makers and found that most domains were not associated with the patient’s preferences or receipt of hospice or life-sustaining treatments. The strongest association was between a belief that a miracle might save the patient and lower hospice use. 71 Chaplains possess specialized knowledge of diverse R/S beliefs and practices regarding medical care and end-of-life scenarios. They adeptly navigate these beliefs and practices in caring for ICU patients, ranging from Jehovah’s Witnesses refusal of blood products to requests for specific religious rituals as death approaches or occurs. Such rituals encompass practices like the Sacrament of Anointing of the Sick for Catholics and smudging ceremonies accompanied by prayers for Native Americans. 72
Impact of race and ethnicity on the ICU experience
Race and ethnicity have several potential effects on the ICU experience, due to differences in culture and beliefs and historical inequities. Compared with White persons, Black and Hispanic persons report higher levels of R/S involvement and importance. For example, while 75% of White persons report that religion is somewhat or very important in their life, the proportion who report this is 84% for Hispanics and 91% for Blacks. 73 R/S also plays a more important role in coping with a family member’s ICU stay for Black and Hispanic family members. Two studies provide evidence this is the case. In one study, investigators conducted race-homogeneous focus groups with Black, Hispanic, and White surrogates of seriously ill patients or patients who had recently died. 74 All of the surrogates described end-of-life decision making as burdensome; key contributors to this were uncertainty about a family member’s prognosis and their wishes for treatment. The investigators reported that compared with the other groups, the Black family surrogates emphasized the importance of support from their R/S. Another study observed the interactions between family members and patients in the ICU. 75 Compared with the White family members, both Black and Hispanic family members were more likely to provide spiritual care to their loved ones (e.g., reading sacred texts). This suggests the particular importance of offering spiritual care to Black and Hispanic ICU families while realizing that there is diversity within these groups and there will be variation in the need for this care.
Inequities in health outcomes for Black and Hispanic patients have been well-documented in the US and contribute to increased life-threatening illness and mortality.17,18 Inequitable treatment in the health care system is one major contributor to poor outcomes and includes worse management of medical conditions and disrespect for religious and cultural beliefs and practices. Black and Hispanic patients are less likely to be provided with prognostic information or have a goal of care conversation in the hospital setting.19,20 Black patients are also less likely to receive hospice care at the end of life and more likely to receive life-sustaining interventions.76,77 The reasons for this are complex and include disparities in communication from clinicians about ACP and end-of-life care, reduced access to hospice care, and patient and family preferences for care at the end of life shaped by deeply held religious and cultural beliefs. 14 The data on the effect of distrust on end-of-life decision making has been mixed, and it is important not to assume that preferences for life-sustaining treatment are based on mistrust rather than genuine preferences; many Black patients do express an acceptance of death and preferences for comfort-focused care in some circumstances.78–81
If distrust in the health system is present, it may be the result of poor communication or poor quality care in the past, a further indicator of the need for culturally sensitive communication. 79 Distrust also impacts ongoing communication and decision making and may increase patient and family stress.82,83 Differences in preferences for ICU treatments must be respected while ensuring that high-quality informational support is provided. Chaplains are particularly attuned to the religious and cultural aspects of decision making and therefore have an important role in navigating decision making in the ICU setting.10,67
This research points to the particular importance of spiritual care for Black and Hispanic ICU family members and to several ways that chaplains’ spiritual care for these family members can influence families’ ICU experience and related outcomes. These include providing R/S support, including R/S rituals that provide comfort and reduce anxiety. Because of their association with trusted R/S institutions such as Black churches, chaplains may be able to build relationships of trust with ICU family members, which can be used to strengthen relationships and facilitate high-quality communication with other members of the clinical team. Facilitating high-quality communication with the clinical team, as well as participating in family meetings with Black and Hispanic families may also contribute to goal-concordant decision making for these families.
Future Directions
Family members of ICU patients are a population with high psychological and R/S distress who are in need of interventions to improve their well-being. R/S are also important in ICU decision making for many patients and families. Despite this, there is great variability in the frequency of contact of ICU families with chaplains. Advocacy, better funding, and system change are needed so that patients with high needs for spiritual, emotional, and informational support have access to chaplains in the ICU setting.
While the research about the effects of spiritual care with ICU family members is growing, it is evident from this overview that it is still quite limited. Based on this review and conceptual model, we propose several specific research topics for future investigation:
Rigorous research can provide evidence for the nature and extent of spiritual care for ICU families in order to improve outcomes for both the patients and the family members themselves.
Conclusion
This narrative review underscores the critical role of spiritual care in addressing the profound psychological and spiritual distress experienced by ICU family members. While current empirical evidence and clinical guidelines strongly support the provision of spiritual care as a standard ICU practice, our review highlights significant gaps in the evidence base and the availability and consistent delivery of such care. The proposed conceptual model offers a rigorous, evidence-informed framework to guide future research and interventions. Future studies should prioritize assessing various spiritual care interventions through randomized controlled trials and explore the mechanisms underlying their effects. Such studies should consider the influence of cultural, racial, and religious diversity, as well as race/ethnicity-based health inequities and other sources of bias on patient and caregiver-related outcome measures. Ultimately, advancing this research will be pivotal in ensuring that all ICU patients and their family members receive the compassionate, holistic care they deserve, paving the way for better long-term outcomes and more equitable care practices.
Footnotes
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
Authors have nothing to disclose.
Funding Information
A.M.T. was supported by a Mid-career Investigator Award in Patient-Oriented Research from the National Institute on Aging (K24AG053794). J.G. was supported by the National Institute on Aging of the National Institutes of Health under Award Number K23AG070234. D.W. was supported by a Mid-career Investigator Award in Patient-Oriented Research from the National Heart, Lung, and Blood Institute (K24HL148314).