
Abstract
Background:
Little is known about the aggressiveness of cancer care at the end of life (ACCEoL) for children with cancer in countries where palliative care (PC) is scarce.
Objective:
The aim of this study was to determine the frequency and time trends of ACCEoL in the pediatric population in a Western European country.
Setting/Subjects:
We conducted a retrospective cohort study analyzing children between 0 and 17 years who died of cancer in public hospitals in Portugal, from January 2010 to December 2015.
Measurements:
Hospital admissions during the last month of life were identified and we analyzed the length of stay and procedures performed. The ACCEoL was measured with a composite indicator.
Results:
We identified 300 children, with a median age of 9 years. A total of 58.7% were male and 31.3% had central nervous system tumors. We found at least one indicator of ACCEoL in 87.8% of patients. “More than 14 days spent in the hospital” (51.0%) and “more than one hospitalization” (43.3%) were the most frequent individual indicators. Infants and children with hematological malignancies had a numerically higher percentage of ACCEoL. We found no statistically significant differences in the frequencies of the ACCEoL among the subgroups. The prevalence of ACCEoL remained stable over the period.
Conclusions:
In our cohort about 9 out of 10 children with cancer experienced at least one indicator of ACCEoL, a rate higher than in countries with well-developed PC services. There is a need to improve the care in the last months of life for children with cancer.
Key Message
The study describes the aggressiveness of care at the end of life in pediatric cancer patients in Portugal, where palliative care was scarce during the period of the study. The high prevalence of children undergoing aggressive care in the last month of life highlights the importance of strengthening pediatric palliative care in the country.
Introduction
In high-income countries, malignant neoplasms remain the leading cause of nonexternal mortality in the pediatric population.1–3 Despite recent advances in early diagnosis and cancer treatment, a considerable proportion of these children will still die as a result of their disease.1,4
Towards the end of life (EoL), children with cancer are known to experience high levels of suffering from emotional and physical symptoms and poor quality of life, many of them receiving high intensity, aggressive, and life-sustaining treatments.5,6 Studies have shown that aggressive EoL care is associated with higher suffering (for both families and patients) and poorer bereavement outcomes. 6
The early integration of pediatric palliative care (PPC), alongside cancer-directed therapies, regardless of the expected outcome, is associated with a lower risk of high-intensity EoL care.7,8 Moreover, children undergoing aggressive EoL therapies and not referred to PPC teams more frequently die in hospitals rather than at home, which is not in keeping with many children’s and families’ wishes.7–11
Little is known about how many children dying of cancer experience aggressiveness of cancer care at the EoL (ACCEoL) in settings where palliative care (PC) and home-based care are scarce, the most common scenario worldwide. 12 Only a few studies evaluating high-intensity medical care at the EoL for children with cancer have been published, most of them from countries with advanced PPC implementation.13–16 These studies used adapted versions of the EoL aggressiveness indicators developed by Earle and colleagues and published in 2003.17,18
The purpose of this study is to describe the prevalence of ACCEoL and its trends over a 6-year period in pediatric cancer patients in a Western European country where PPC delivery was scarce during the study period.
Methods
Study population and the hospital morbidity database
We conducted a nationwide cohort study of all children with a diagnosis of cancer who died in public hospitals in mainland Portugal between January 2010 and December 2015. The term children was defined as patients from birth to 17 years old.
Data were collected from the Hospital Morbidity Database, provided anonymized by the Portuguese Health System Central Administration. This database contains information about all admissions in mainland Portugal public hospitals. For each admission, we had access to the age and sex of the patient, main and additional diagnoses, list of procedures performed during admission, length of stay, and discharge destination. Both diagnoses and procedures were classified according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
The following inclusion criteria were used: (1) age 17 years old or younger; (2) diagnosis of cancer, identified through the main or additional ICD-9-CM diagnoses codes (chapter “Neoplasms” codes 140–239), excluding benign neoplasms (210–229), carcinoma in situ (230–234), neoplasms of uncertain behavior (235–238), or unspecified nature (239); and (3) deceased at hospital. Information regarding patients’ age at the time of death, sex, malignancy type, and type of hospital where death occurred (cancer center or general hospital) was collected. After patient selection, all hospital admissions that occurred within the last month of life were identified and data were collected about the length of stay, diagnoses, and procedures. The cause of death (i.e., refractory/progressive disease vs. treatment complications) was not available. Treatment intent (curative vs. palliative) was also not available. Age at the time of death was organized into five categories—infants (birth up to 12 months of age), preschool aged children (1–5 years old), school-aged children (6–10 years old), preteenagers (11–14 years old), and teenagers (15 years old or older). Malignancy type was classified into three categories: hematological (ICD-9-CM codes 200–208), central nervous system (CNS) tumors (ICD-9-CM codes 191–192), and non-CNS solid tumors (ICD-9-CM codes 149–190, 193–196).
Setting
Portugal is a Western European country with a publicly funded health care system, guaranteeing universal health coverage and open access for all citizens. Pediatric oncology care in Portugal is mainly delivered through four Pediatric Oncology Units, two of them located in specialized cancer centers and two of them in teaching general hospitals. Patients can, nevertheless, be admitted to any other public hospital where death can also occur. Only public hospitals treat pediatric cancer in the country. Until 2013, PPC was not an officially recognized activity and only in 2015 the Ministry of Health recommended the creation of PPC teams and units in Portugal. This means that PPC coverage during the period of the study was scarce. 19
Indicators of ACCEoL
The selection of indicators of ACCEoL was based on previous similar studies, most of them in the adult population.13,14,16–18,20–24 Do-not-resuscitate (DNR) order, emergency department visits, and enrollment in phase I trials were not analyzed, as this information was not available. A group of pediatric oncologists was consulted, and their opinion was considered for the selection of indicators. This expert panel agreed to exclude tube feeding and transfusion of blood products, used in adult studies as indicators of aggressiveness, as these procedures are often used in children at the EoL with the intention of improving quality of life. 20 Admissions for the sole reason of chemotherapy administration were also excluded because different hospitals could have differences in practice when admitting a patient for chemotherapy and this procedure is already being considered in another individual indicator regardless of the setting of treatment administration. The primary outcome was defined as a composite measure of ACCEoL, positive when at least one individual indicator was present. The final list of individual indicators and respective ICD-9-CM codes (when applicable) can be found in Table 1. A secondary analysis of the primary composite outcome, excluding the indicators related to hospital admissions and length of stay, was not planned intentionally as the intervention-based indicators are particularly influenced by the possibility of under-recording in our database.
Indicators of Aggressiveness of Care at the End of Life Used and International Classification of Diseases, Ninth Revision, Clinical Modification Codes
ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; IV, intravenous.
Within the hospital, treatment occurred in a general ward or at the intensive care unit (ICU); this could not be differentiated in the Hospital Morbidity Database, as there is no code for “ICU admission.” We estimated this indicator through a proxy, considering admission to ICU as having occurred if at least one of the following ICD-9-CM codes was present: 38.91 (arterial catheterization), 89.61 (systemic arterial pressure monitoring), 96.70/1/2 (mechanical ventilation), or 39.65 (extracorporeal membrane oxygenation).
Statistics
Descriptive statistics (frequencies and measures of central tendency and dispersion) were used for the characterization of the sample: age category at the time of death, sex, malignancy type, and hospital type where death occurred. The percentage of patients who experienced the individual and composite indicators of ACCEoL was calculated. We used a binomial exact test to estimate the 95% confidence interval (95% CI). We also examined time trends between 2010 and 2015 for the whole cohort, using χ2 test for trend, and compared the frequency of indicator of ACCEoL between different groups (age category, sex, malignancy type, and hospital type where death occurred) using χ2 test. Significance was defined as p < 0.05. STATA®IC 12.1 was used for all the analyses.
Ethics
Ethics committee approval and informed consent were not needed for this study, as all data were routinely collected and had been previously anonymized.
Results
Sample characteristics
During the study timeframe, 300 children died of cancer in public mainland Portuguese hospitals (Table 2). Age at the time of death varied between 0 and 17 years (median age: 9 years, interquartile range: 4–14), school-aged children being the most prevalent age group (26.7%). The median age of death remained stable over the study period. Fifty-eight percent of the deceased were males. Non-CNS solid tumors were the most frequent malignancy type (41.4%), whereas CNS tumors and hematological malignancies represented 31.1% and 27.3% of the total diagnoses, respectively. Half of the children died in cancer centers (50%) (Table 2).
Characteristics of the Sample
Age at the time of death.
mo, months old; yo, years old.
Frequency of the individual and composite indicators of ACCEoL
Among the children included, 87.8% (95% CI: 83.3%–91.1%) experienced at least one of the individual indicators of ACCEoL. Analyzing the frequency of each individual indicator (Fig. 1
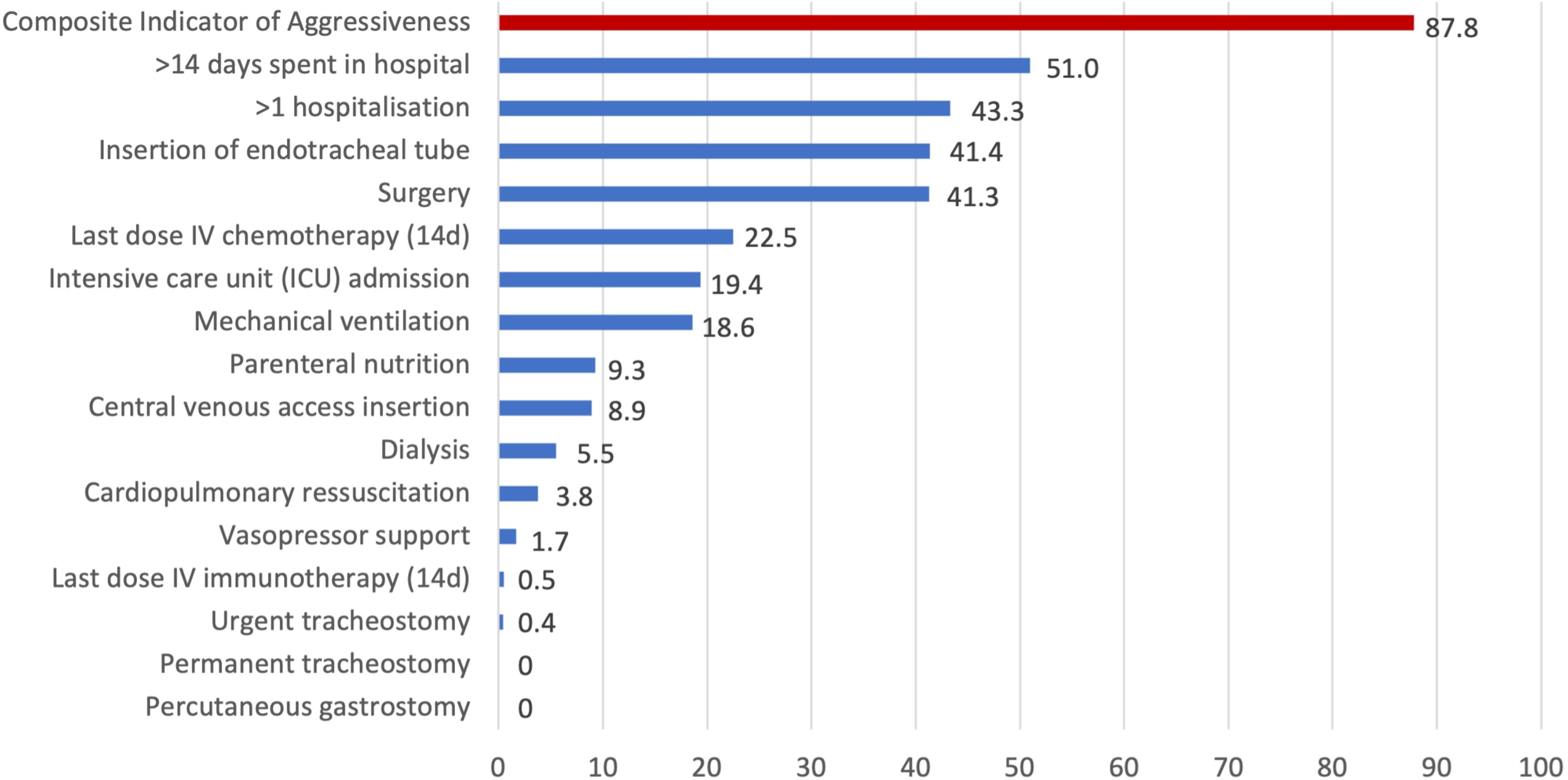
Frequency of individual indicators of aggressiveness of cancer care at the end of life. Intensive care unit admission was estimated with a proxy of procedures as described in the methods. d, days; IV, intravenous.
From 2010 to 2015, there were no statistically significant changes in the prevalence of ACCEoL over time (Fig. 2), with its frequency remaining stable (85.2% in 2010, 88.4% in 2015, p = 0.82). No significant changes were found for trends over time of each individual indicator during the study timeframe.

Trends of aggressiveness of cancer care at the end of life over a timeframe.
Comparing the frequency of the ACCEoL among different groups (age category, sex, malignancy type, and hospital type where death occurred), infants and patients with hematological malignancies had numerically higher percentages of ACCEoL (94.4% and 91.5%, respectively). Nevertheless, we found no statistically significant differences in the frequencies of the ACCEoL among the different subgroups (Table 3).
Frequency of Aggressiveness of Cancer Care at the End of Life Among Different Groups
Age at the time of death.
ACCEoL, aggressiveness of cancer care at the end of life; mo, months old; yo, years old.
Discussion
This is the first Portuguese cohort study to evaluate the ACCEoL in children with cancer and it is among the first ones to be developed in PPC scarce settings. 25 We found that 87.8% of patients experienced at least one indicator of ACCEoL. The most prevalent indicators were “more than 14 days spent in hospital” and “more than one hospitalization” in the last 30 days of life. The indicators remained stable during the analyzed period and there were no significant differences in the frequency of ACCEoL according to age category, sex, malignancy type, or hospital type where death occurred.
The rate of ACCEoL in our sample seems to be higher than reported in other studies using similar methodologies and indicators. A North American study found a frequency of ACCEoL of 40.6%, with only 17.6% of the children having more than one hospitalization in the last 30 days of life. 15 In a Taiwanese study, the frequency of individual indicators was also lower, with only 32.5% of patients having more than one hospitalization in the last 30 days of life. 23 Finally, an Italian study in children with solid tumors found an even lower frequency, with only 26% meeting at least one criteria for ACCEoL. 8 All three studies analyzed in-hospital and out-of-hospital deaths (home or hospice), although only the Italian publication analyzed ACCEoL rates at home (45.6%) or in hospice (23.5%) separately.
The higher rates of ACCEoL found in our study may have several explanations, including place of death, level of PPC implementation, availability of community support at home, and cultural aspects. All three aforementioned studies included patients in different care settings and the fact that our study only included patients who died in hospitals can possibly have constituted a selection bias, overestimating the level of ACCEoL. However, a similar French study, including only pediatric patients with cancer who died in the hospital, also found lower rates of aggressiveness, with 61.4% of patients undergoing hospital admissions or emergency department visits in the last 30 days of life and 28.8% receiving invasive procedures (e.g., intubation, mechanical ventilation, cardiopulmonary resuscitation). 26 Although we only included patients who died in the hospital, our sample probably reflects the Portuguese reality. Indeed, the Portuguese National Institute of Statistics reported 396 cancer-related deaths in children under the age of 19 years old from 2010 to 2015, 27 which shows that 75% of children who died with cancer were included in our study. The remaining 25% may include deaths outside the hospital (hospice or home). Since it was not possible to merge the data source used for our study (National Hospital Morbidity Database) with all the deaths reported by the National Death Certificate Database, we could neither estimate the exact proportion of hospital deaths nor include in the study children with a diagnosis of cancer who died elsewhere. However, the percentage of children dying of cancer at home in Portugal had previously been found to be low (9.6% in 2011). 28 It is important to emphasize that there is no published data on the preferred place of death for children dying from cancer in Portugal, so it is not possible to estimate whether this percentage could be higher if there was adequate PPC involvement and home support for families.
Another aspect potentially contributing to the differences found could be the level of PPC implementation. The delivery of aggressive treatments in the last weeks before death is associated with more severe and uncontrolled symptoms, 29 and these are some of the main causes of hospitalization, 30 increasing the likelihood of death occurring in the hospital. 8 Previous studies have shown that early PPC integration is associated with improved communication, the establishment of care goals, better control of symptoms and EoL quality indicators, less ACCEoL, and lower rates of hospital utilization.7,30–35 The higher rate of ACCEoL, especially frequent hospital admissions (43.3%) and longer hospital admissions (51.0%), could also be justified by the lack of home-based PPC and involvement of community professionals in the country. As a result, there could be a potential overestimation of ACCEoL, as children and parents would most likely have to stay in the hospital for EoL management, regardless of the preference over the place of death. However, both indicators are a very relevant metric of aggressiveness and these results reinforce the need for community PC support, together with further research on the preferred place of death. It has been shown that close to death, the presence of a qualified team who can deliver PPC at home enables better treatment of complications and symptom control.9–11,36 Consequently, it minimizes hospitalizations and reduces both the length of hospital stay and the use of intensive medical services.9,10,36 In line with these findings, both the Italian 8 and the French 26 studies showed that integration of a PPC team was associated with lower rates of ACCEoL. Since our study was based on administrative data, it was not possible to determine whether patients had access to PPC or the patients’ and parents’ preferred place of death. However, we know that access to home-based PPC and hospices was scarce in Portugal during the period of the study.
Lastly, we must also consider cultural differences. It has been recognized that cultural aspects and religion may affect decision-making at the EoL.37,38 One study analyzing EoL care in Southern European countries (Portugal included) revealed lower rates of DNR orders discussion and withdrawal of therapy when compared to Northern Europe. 39 These findings could be partially explained by cultural similarities in southern Europe, namely prevalence of the Catholic religion and the strength of family ties. 40 When implementing a PPC team and integrating it with the primary team, it is essential to consider these cultural differences. 7
Interestingly, the reported frequencies of insertion of endotracheal tube and surgery were similar (41.4% and 41.3%, respectively) in our study. A high prevalence of intubation in the last month of life (41.4%) was also reported in the Taiwanese study, 23 whereas a lower rate was found in the French study (28.5% of intubation and/or mechanical ventilation). 26 Regarding the frequency of surgery, similar rates were found in one American cohort (35.4%), 41 and in one Swiss study (35.0% of interventions requiring anesthesia, not only surgical procedures). 42 One hypothesis for these similar rates in our study is that children were intubated most likely to undergo surgery, rather than for the need of ventilatory support for respiratory failure. This is reinforced by the fact that the rate of patients who required mechanical ventilation (18.6%) was less than half of the rate of endotracheal tube insertion (41.4%). Smaller interventions (e.g., programmed insertion of the central line) may have contributed as well to this indicator. Indeed, one study reported that the procedures more often performed in the last months of life are intravenous access, feeding access, and tracheostomy insertion. 43
However, there are other indicators in our cohort whose frequencies are lower than previously reported in countries with advanced PPC. Based on the proxy definition, the estimated rate of ICU admission was 19.4%, which was numerically lower than in the Taiwanese (57.0%), 23 the French (34.4%), 26 and the North American (21.7%) 15 studies. An even lower prevalence was seen in an Italian cohort (7%) 8 but this could be explained by the fact that it only included patients with solid tumors. Regarding doses of intravenous chemotherapy in the last 14 days of life, the percentage of children who received intravenous (IV) cancer-directed therapy in our analysis was also numerically lower (22.5%) than the ones from the Taiwanese (52.5% in the last month of life) 23 and the French (25.3%) 26 studies, but higher than those described in North America (7.9%) 15 and Italy (14%). 8 Although we did not have access to the cause of death, the low rate of most invasive treatments (e.g., cardiopulmonary resuscitation [3.8%], dialysis [5.5%], vasopressor support [1.7%]) suggests that treatment-related mortality (and consequently the use of chemotherapy with curative intent) was infrequent and the majority of deaths were due to progressive/refractory disease. Interestingly, the low percentage of cardiopulmonary resuscitation (CPR) seems to contradict the otherwise high frequency of ACCEoL found in our study. This could be partially explained by underreporting and recording of CPR, but it is not likely that this is the sole reason. To the best of our knowledge, there are no studies evaluating CPR practice at the EoL in the general pediatric population in Portugal, but sociocultural differences or even different medical practices within countries could also be part of the explanation. This possibility may also explain why the Taiwanese study reported a much higher percentage of CPR in their cohort (16.7%–30.4% over the analyzed period), 23 whereas the French study reported a frequency of only 3.4%. 26
When compared with studies developed for the adult population dying from cancer, our results also revealed a higher proportion of ACCEoL. A very similar Portuguese study in adults found a prevalence of ACCEoL of 71.1%, 44 significantly lower than ours (87.7%). 45 In this study, almost all the individual indicators presented a lower frequency, for example, “more than 14 days spent in hospital in the last 30 days of life” (42.7% adults vs. 51.0% children) and “more than one hospitalization in the last 30 days of life” (25.1% adults vs. 43.3% children). 44 Similarly to our results, this Portuguese study found a very low percentage of CPR (1.1%), reinforcing the possibility that our results are explained by underreporting/recording or sociocultural differences. These differences between adult and pediatric studies have also been found in other countries. A study in the adult North American population found a frequency of a composite indicator of 22.4% 24 versus 40.6% in a pediatric study.15,24
Contributing to these differences may be the fact that death in the pediatric age in general, and among children with cancer, is not as frequent as in the adult population. 4 When compared to other pediatric subspecialties, pediatric oncologists are the ones who more frequently discuss palliation and EoL care. They are also the ones who more frequently report having had education on advanced care planning. 46 However, although more prepared than other pediatricians, many pediatric oncologists still experience significant anxiety around death and dying. 47 Compared to adult oncologists, pediatric oncologists are more likely to believe that their patients and their families have negative perceptions of PPC and that PPC adds too many health care providers to the managing team. 48
Similarly to other studies,15,44 we did not find any time trend in the frequency of ACCEoL. This may be explained by the fact that only recently a national strategy for PPC service development has been implemented. 25
Nonetheless, we need to interpret our results considering the study’s limitations. The use of anonymized administrative data does not allow linkage with other clinical information, for example, time since diagnosis, disease status (remission, refractoriness, relapse, progression), potentially curative treatment options still available, PPC team involvement, patients’ and parents’ preferences over the preferred place of death and cause of death. We could also not obtain any information regarding emergency department visits and DNR orders.
The strength of our study relies on the fact that it included children of all age groups, from all regions of mainland Portugal and with all types of cancer, and that we analyzed all children who died during hospital admission with a cancer diagnosis in this study period, representing the majority of children dying with cancer in the country.
Conclusion
Our study estimates that 9 out of 10 children dying of cancer in Portugal experience ACCEoL. Education and training of health care professionals on the role of palliative medicine,7,49 creation, and strengthening of PPC teams, integration of PPC team to the primary team, understanding of cultural differences,7,50 and implementation of home-based PPC, 10 are vital to achieve the goal of better EoL care for children dying with cancer. Continued assessment of ACCEoL patterns in the pediatric population in upcoming years, as well as child and parents’ preferred place of death, will be of utmost importance to evaluate the impact of the recent expansion of PPC training and specialized services in Portugal. 51
Footnotes
Acknowledgments
The authors thank the Health System Central Administration for providing access to the hospital morbidity database and the
Ethics Approval and Consent to Participate
Ethical approval was waived by the main academic sponsor of the research project—King’s College London Biomedical Sciences, Dentistry, Medicine and Natural and Mathematical Sciences Research Ethics Subcommittee (BDM, RESC), as all the information collected is freely/publicly available under appropriate request and personal opinions and thoughts were not sought. In addition, national ethical approval and informed consent were waived by the Ethics Committee of Instituto Português de Oncologia de Lisboa Francisco Gentil (IPO, Lisbon) since all clinical data used had previously been anonymized and coded to official administrative databases.
Consent for Publication
Not required.
Availability of Data and Material
Data are available on reasonable request. Data may be obtained from a third party and are not publicly available. All data relevant to the study are included in the article or uploaded as supplementary information. Raw data from the Hospital Morbidity Database were provided by the Portuguese Health System Central Administration. The study protocol and programming code are stored by the respective coauthors.
Authors’ Contributions
A.L.C.: Investigation, writing—original draft preparation, visualization, and project administration. L.G.D.N.: Validation, writing—original draft preparation, visualization, and project administration. D.M.B.: Conceptualization, methodology, formal analysis, data curation, and writing—review and editing. A.L.: Conceptualization, validation, writing—review and editing, and supervision. B.G.: Conceptualization, methodology, writing—review and editing, and supervision. S.L.: Conceptualization, methodology, resources, writing—review and editing, and supervision.
Author Disclosure Statement
A.L.C. and L.G.D.N.: No conflicts of interest to disclose. D.M.B.: Declares full-time employment from the European Society for Medical Oncology since September 1, 2023; participation as medical research fellow in research studies institutionally funded by Eli Lilly, F. Hoffmann-La Roche Ltd., and Novartis to Institut Jules Bordet (2021-2023); and non-financial interests as a board member of Associação de Investigação e Cuidados de Suporte em Oncologia (2022-2024) and member of American Society of Clinical Oncology, Associação Portuguesa de Cuidados Paliativos, Multinational Association of Supportive Care in Cancer, and Sociedade Portuguesa de Oncologia. A.L.: Meeting/travel grant from EusaPharma and MSD; nonremunerated leadership role as chair of the Pediatric Working Group of the Portuguese Palliative Care Association, of the Palliative Care Working Group of the Portuguese Society of Pediatrics, of the European Association for Palliative Care Children and Young People Reference Group and the Palliative Care Working Group of the European Society of Pediatric Oncology. B.G.: Scientific advisor of the La Caixa Foundation Programme of Comprehensive Care for People with Advanced Diseases in Portugal since 2018. S.L.: No conflicts of interest to disclose.
Funding Information
This work was supported by the