
Abstract
Background:
Limited knowledge and negative perceptions of palliative care (PC) can result in missed opportunities to access specialty PC. Patient, caregiver, and community education may improve knowledge and attitudes about PC.
Methods:
Pre- and post-session surveys along with qualitative interivews assessed whether participation in a novel 60-minute webinar about specialty PC changed participants’ PC knowledge and attitudes. Participants were recruited in collaboration with community based organizations and included self-identified patients, caregivers, healthcare providers, and other individuals interested in the topic.
Results:
A total of 118 participants completed pre- and post-session surveys. Participants demonstrated a significant increase in PC knowledge on the Palliative Care Knowledge Scale (10.6 vs. 12.5, p < 0.001). Pre-session attitudes were positive and further improved after the educational session. Qualitative interviews demonstrated that participants learned that PC provides more services than previously thought and could ask for a PC referral.
Conclusion:
We conclude that a 60-minute webinar improved knowledge and attitudes about specialty PC, including a willingness to ask for and accept a referral to PC.
Introduction
The availability of palliative care (PC) has increased over the last two decades, and the evidence for its benefits is growing.1,2 Despite PC’s growth, low awareness, limited knowledge, and negative attitudes about PC persist.3–8 Education for patients, caregivers, and the community is an important step to overcome barriers to patients asking for and accepting PC.3,5,9–14 While knowledge alone may be insufficient to promote behavior change, educational interventions rooted in social learning theories that address knowledge, attitudes, self-efficacy, and social norms may trigger behavior change.15,16 A systematic review found that a variety of PC educational interventions improved knowledge and attitudes among public, patient, and caregiver populations and noted a need for interventions rooted in adult learning principles. 17
We aimed to assess whether a novel webinar about specialty PC, designed using the theory of planned behavior, changes PC knowledge and attitudes among a purposive community-based sample that included patients and caregivers. Participants’ change in knowledge and attitudes about PC was evaluated with a pre/post survey, and perceptions of the session were captured by semi-structured interviews.
Methods
We partnered with community-based organizations (CBOs) to recruit participants through email listservs, newsletters, community calendars, and social media. A 60-minute webinar was chosen to fit with CBOs’ preexisting structures for delivering educational content to clients. Webinar content is described in Supplementary Data S1 and integrated principles of Ajzen’s theory of planned behavior, which describes that health behaviors are influenced by behavioral, normative, and control beliefs. 18 Webinars were conducted using Zoom (San Jose, CA: Zoom Video Communications Inc). This evaluation was reviewed by the Stanford University Institutional Review Board and deemed to be non-research/quality improvement (IRB-65638).
Pre- and post-session surveys assessed PC knowledge and attitudes. PC knowledge was assessed using the Palliative Care Knowledge Scale (PaCKS), a 13-item true/false/don’t know questionnaire.8,19 PC attitudes were assessed using a questionnaire adapted from Ajzen’s theory of planned behavior, which used a 5-point Likert scale to gauge participants’ level of agreement with 10 statements regarding behavioral, norm, and control beliefs.20–22 (Supplementary Data S2). The pre-session survey captured participant demographics, including prior awareness of and experience with PC. Pre- and post-session surveys were professionally translated and back-translated to/from Spanish using our medical interpreter services.
For PC knowledge, we collapsed incorrect answers and “don’t know” responses to dichotomized variables of “correct” or “incorrect.” The total PC knowledge score was calculated by totaling the number of correct answers out of 13 questions. For PC attitude, Likert scale responses were coded, including reverse coding where appropriate, to a 1 to 5 scale for analysis, with higher scores corresponding to more favorable attitudes. McNemar’s test was used to compare correct responses pre- and post-session for each knowledge item. Wilcoxon signed rank test was used to compare pre- and post-session total knowledge scores and scores for each attitude item. Statistical significance was set at p ≤ 0.05. Means and standard errors (SE) are reported. Analyses were conducted in JMP® Pro, Version 17 (SAS Institute Inc., Cary, NC, USA).
Semi-structured interviews were conducted among participants who volunteered for a telephone-based interview using a structured interview guide (Supplementary Data S3). Interviews were recorded with participant permission using Zoom (San Jose, CA: Zoom Video Communications Inc). Interviews were analyzed using a rapid qualitative approach. 23 Using audio recordings and contemporaneous notes from interviews, two analysts (ACN, AK) independently summarized participant comments into a matrix. The two analysts and a third author (GMS) then reviewed and discussed the matrix data and summarized thematic elements within each of the columns.
Results
Between May 2022 and September 2023, 14 educational webinars were held (Table 1). Attendance totaled 284 with an average of 20 attendees per webinar. Of those attendees, 42% (118/284) completed both a pre-session and post-session survey, with an additional 88/284 (35%) attendees completing only the pre-session survey (Table 2). Most participants were female, non-Hispanic, college-educated and had non-Medicaid insurance. Approximately half of the participants identified as white/Caucasian, a third as multi-racial or other, and a quarter as Asian (Table 2).
Community Partners, Target Populations, and Attendance at Webinars
Attendance numbers are based on the number of accounts logged in to each webinar. Multiple individuals may have been participating through any of the individual accounts.
Demographic Characteristics and Baseline Experience/Knowledge of Palliative Care Reported by Participants Who Completed the Pre-Webinar Survey (All Respondents) and Participants Who Completed the Pre- and Post-Webinar Survey (Participants)
PC, palliative care; SE, standard error.
Among individuals who completed both pre- and post-session surveys, participants self-identified as patients or persons living with a serious illness (32%, 38/118), caregivers (14%, 17/118), individuals interested in the topic (24%, 28/118), healthcare providers (18%, 21/118), or “other” (12%, 14/118). Most participants who identified as patients had cancer (71%, 27/38). Caregivers most reported caring for individuals with dementia (53%, 9/17) or cancer (29%, 5/17). Most participants had heard of PC (84%, 99/118), and 33% (33/99) of those who had heard of PC reported either having had a visit with PC or having a family member who had a visit with PC.
Fourteen participants completed interviews, which lasted between 5 and 24 minutes (median: 11 minutes). Nearly all interviewees (86%, 12/14) reported being a patient, caregiver, or a combination of both roles. Themes and supporting quotes are shown in Table 3.
Semi-Structured Interview Themes and Quotes
The mean PC knowledge score on the PaCKS increased from 10.6 [standard error (SE) 0.3] to 12.5 (SE 0.1) (range 0–13, p < 0.001). Compared to the presession responses, all but one item on the post-session survey showed statistically significant improvement in the proportion of participants answering correctly (Fig. 1 and Supplementary Data S4). Participants in the semi-structured interviews identified main learnings as recognizing that PC provides more services and support compared to what they thought prior to attending the session. This included learning that PC provides more than end-of-life care, that PC includes caring for caregivers, and that doctors are involved in the PC team. Participants wanted additional content about the availability of PC programs and to hear more about what the first visit with a PC team might be like.
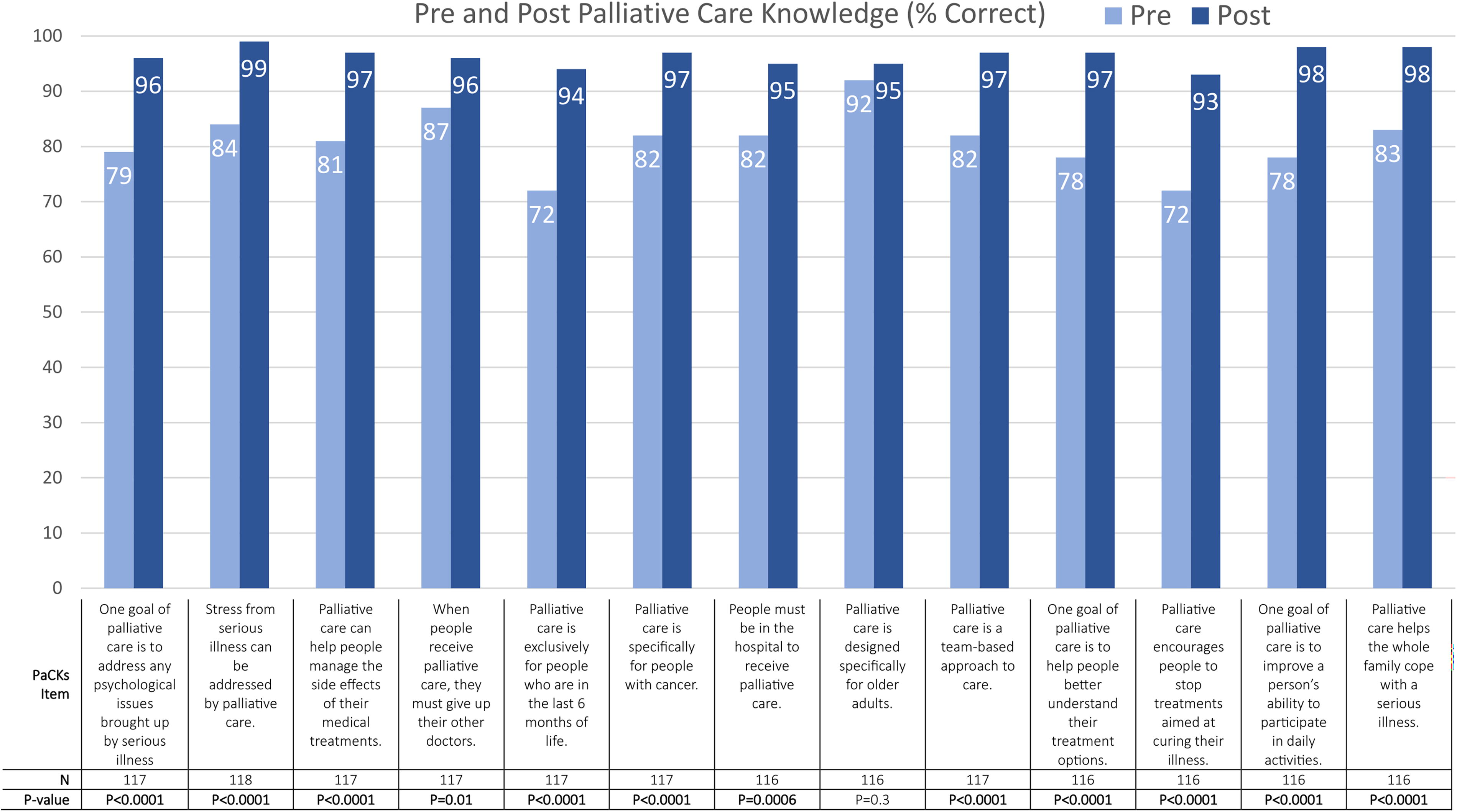
Change in knowledge as measured by the Palliative Care Knowledge Scale (PaCKS) questionnaire before (pre) and after (post) a webinar.
Changes in attitudes were statistically significant for each item and primarily reflected shifts from a neutral or somewhat positive attitude to more positive attitudes (Fig. 2). Participants shifted to feeling less unsure and less in agreement that a PC visit would be scary and were in greater agreement that a PC visit would be comforting and helpful. Interviewees described that participation led to feeling less scared, afraid, or worried, and specifically feeling less worried about the future and not feeling alone. Participants shifted to agreeing more strongly that their doctors and loved ones would support them in having a PC visit. Participants demonstrated some of the most positive post-session attitudes for control beliefs, including “I would have a palliative care visit if my doctor recommended it,” “I would have a palliative care visit if I felt it was needed,” and “I can ask my doctor for a referral for a palliative care visit.” Control beliefs were also explored in the semi-structured interviews, and most interviewees expressed that they felt able to ask for a referral to PC for themselves or a loved one after attending the session.

Change in Palliative Care Attitudes as measured by a survey based on the theory of planned behavior that was administered before (pre) and after (post) a webinar.
Discussion
This mixed-methods evaluation demonstrates that participation in a 60-minute educational webinar about PC is associated with improved knowledge and attitudes about specialty PC. The greatest improvements in knowledge occurred for the most common misperceptions about PC, including that PC is only for people at the end of life and that PC encourages stopping treatments.5,6,8,13,14,24–26 Interviewees corroborated survey findings, describing that they learned that PC offers more services than they previously thought and PC provides more than end-of-life care. Attitudes improved across all domains of the theory of planned behavior with a significant increase in participants disagreeing that a PC visit would be scary, representing improvement in one of the most common negative attitudes linked to patient and provider resistance to PC referrals.13,14,24–26 Interviewees corroborated these findings, describing feeling less afraid and less alone after learning about specialty PC, although generalizability of interviews was limited since most interviewees were patients or caregivers.
Compared to the public, our purposive sample had greater awareness, more accurate knowledge, and more positive attitudes about specialty PC before the webinar.3–5 This is expected as we recruited participants through organizations that primarily serve individuals with greater exposure to and knowledge of health care. Higher levels of awareness and knowledge about PC are anticipated among healthcare workers and have been noted among patients and caregivers, who comprised a majority of the participants in our evaluation.7,27 Demographic factors such as being female, white, older, or having higher educational attainment correlate to greater awareness and knowledge about PC and reflect the demographics of our sample.3–5,8 Our sample also reflects individuals who are interested, willing, and able to attend a 60-minute educational webinar about PC, which likely reflects a community distinct from the public. Despite our sample’s baseline awareness, knowledge, and positive attitudes, participation still showed significant improvements in knowledge and attitudes, making our findings encouraging as a “proof-of-concept” that this type of education can be effective in achieving the knowledge and attitude outcomes that could lead to improved timely access to specialty PC, especially among community members engaging in educational content through local CBOs.
Future work will need to explore educational interventions that reach a broader and more culturally diverse population with less baseline awareness and knowledge about PC. These endeavors will likely require unique interventions and utilize tools like social media to reach this population.
Footnotes
Acknowledgments
Claire Bleymaier, Jonathan Briganti, Denise Garlick (Cancer CAREpoint), Morrigan Bruce (Cancer CAREpoint), Claudia Bravo (Cancer CAREpoint), Jeanette Gonalez (Bay Area Cancer Connections), Sally Skidgel (Caltrans), Tina Choi (Travonde), Lynn Chao (Stanford Lung Cancer Support Group), Anjali Kapoor-Davis (ThyCa), Gary Bloom (ThyCa), and Flor Mendez (Vision Y Compromiso).
Funding Information
This work was supported by a Stanford Division of Primary Care and Population Health Seed Grant and an anonymous philanthropic gift.
Author Disclosure Statement
G.M.S., S.M.R.K., A.B., A.C-N., K.T., O.T.N., and L.M.H. received financial support from an anonymous philanthropic gift and an institutional seed grant from the Division of Primary Care and Population Health at the Stanford School of Medicine.