
Abstract
Background:
Medical aid in dying is legal in 10 states plus Washington DC, covering 22% of the U.S. population. Much has been written about the ethics of aid in dying, but little about evidence-based care, especially the medications used. We investigated the efficacy of four commonly used aid-in-dying medication protocols—using the time to sleep and time to death as proxies for efficacy.
Methods:
We performed an independent, secondary analysis on deidentified data from four organizations, comparing four different medication protocols. Descriptive statistics for time to sleep and time to death for the different medication protocols were calculated. Medication protocols included one sedative and three sedative/cardiotoxin combinations.
Results:
We analyzed data from 3332 death reports covering 2009 to 2023, comparing a single sedative medication protocol with three different sedative/cardiotoxin combinations. The sedative alone yielded the most rapid median time to death of 0.4 hours, but with days-long outliers. Two of the sedative/cardiotoxin combinations yielded median times to death of 0.8 hours. But from 2018 to 2023, as the medication combinations shifted, the mean time to death declined while the median remained relatively steady—confirming that these combinations reduced the incidence of longer deaths (especially extreme outliers).
Conclusion:
This first-time analysis of aid-in-dying medication protocols showed that while a sedative alone had the best median time to death, the most recent sedative/cardiotoxin protocol had an acceptable median time to death of 0.8 hours, but with fewer prolonged-death outliers.
Key Messages
This article is the first to analyze various medical aid-in-dying medication protocols.
Our sedative/cardiotoxin protocol produces acceptable time to death for patients receiving medical aid in dying care.
Developing an evidence-based paradigm for the practice of medical aid in dying is paramount to good patient care.
Introduction
The nascent field of medical aid in dying for terminally ill patients has fostered best practices by means of innovative data collection, analyses, and dissemination of the results to interested clinicians.1–5 The ethical aspects of aid in dying have been extensively discussed in the literature6–9 and the authors acknowledge the controversy about the practice. The ethical premise of this paper, however, is that when patients request medical aid in dying in states where it is a legal choice, they should receive the best evidence-based clinical care possible—established by peer-reviewed studies including those detailing the efficacy, risks, and safety of aid-in-dying medications.
Oregon implemented the first U.S. aid-in-dying law in 1997, 10 allowing terminally ill patients with less than six months to live to receive lethal medications for oral self-administration (no injections were permitted). As of this writing, 10 states and Washington DC have legalized aid in dying, covering 22% of the U.S. population, a substantial constituency.11–13
From 1997 to 2016, barbiturate secobarbital was the primary aid-in-dying medication14,15—to induce coma, respiratory suppression, and death. Occasionally, coma was not accompanied by sufficient respiratory suppression, with patients dying days after the ingestion from the secondary effects of prolonged coma. 10 This was not the patients’ nor waiting loved ones’ expected timing or quality of death. Data collected by the Oregon Health Authority showed that secobarbital was efficient, but not reliable. 16
In 2018, secobarbital fell out of favor 17 due to increased cost, decreased availability, and a desire for more reliable aid-in-dying pharmacology. But for a variety of reasons including stigma about the practice, medical institutions and pharmaceutical companies did not participate in aid-in-dying research. Bedside clinicians formed small groups to initiate new aid-in-dying protocols for their individual patients, using FDA-approved medications legally prescribed for this off-label purpose. From 2015 to 2019, three new protocols came into use from these groups.14,18
For this article, we gathered data from four independent organizations that monitored the efficacy and safety of the aid-in-dying medication protocols: End of Life Choices Oregon (EOLCOR) 19 ; End of Life Washington (EOLWA) 20 ; Bay Area End of Life Options (BAEOLO); 21 and the American Clinicians Academy on Medical Aid in Dying, now the Academy of Aid-in-Dying Medicine (Academy). 2 The Academy was formed in 2020 and initiated an extensive online data collection system to study the results of the pharmacologic protocols used in aid in dying. 22 State departments of health (mainly Oregon, Washington, and California) also gathered data, but only published aggregate summaries that did not directly link outcomes to the pharmacology used.16,23,24 We consider their results in our conclusions, but their aggregate data summaries could not be used in our database.
This paper intends to bring together data from multiple sources to form a joined database consisting of more than 3000 outcome reports. We used this first-time multiple-database analysis to make appropriate recommendations for both clinical care and future studies.
Methods
We performed an independent, secondary analysis of the Academy’s data on aid-in-dying medications as collected by their online reporting form. 22 Deidentified Academy data were provided to author (S.H.) for analysis in a Microsoft Excel spreadsheet. Data from EOLCOR, EOLWA, and BAEOLO were also made available through the Academy in the same format. The Community Health System Institutional Review Board 25 determined this study was exempt from U.S. Department of Health and Human Services regulation 45 CFR 46. 26
All sources contributed year and quarter of death, terminal diagnosis, medication administered, route of administration (oral, rectal, and feeding tube), time to sleep, and time to death. Age data was available from all organizations except EOLWA. Prior opiate exposure data (a Likert-type 4-point scale of naïve to major opiate tolerance) was only available from the Academy.
We studied two different time intervals, starting from the ingestion of the medications: time to sleep and time to death. Since the deaths took place in patients’ homes, without cardiac or other monitoring, these times were determined by bedside clinical criteria. Time to sleep: no longer responsive to loud verbal stimuli. Time to death: Apnea and lack of detectable pulses. For time to death, the authors established the following five analysis categories: under 2 hours (successful); 2 to less than 5 hours (acceptable); 5 to less than 10 hours (problematic); 10 to less than 20 hours (disturbing); and 20 or more hours (outlier).
The medication protocols analyzed were, in order of usage (all sedative/cardiotoxin medications were compounded from pure-agent powders, mixed to a suspension of 2–4 ounces. Secobarbital was typically obtained as 100 capsules from which the powders were extracted, thus including filler as well as medication. The powders were typically mixed to form a 4-ounce suspension):
Sedative (secobarbital) 10 g alone (1997–2020) Sedative/cardiotoxin combinations:
DDMP2 (2016–2022): digitalis 50–100 mg, diazepam 1 g, morphine 15 g, propranolol 2 g. DDMA (2018 to present): digitalis 100 mg, diazepam 1 g, morphine 15 g, amitriptyline 8 g. DDMAPh (2019 to present): digitalis 100 mg, diazepam 1 g, morphine 15 g, amitriptyline 8gm, phenobarbital 5 g.
Data analysis was done using SAS software. 27 Descriptive statistics described the time to sleep and time to death by category for the different medication protocols. Chi-square tests were used to compare categorical data for differences. Continuous data was not normally distributed, therefore non-parametric Wilcoxon rank sum tests were used to compare continuous data, and Spearman rank-order correlation was used to investigate numeric data by category differences. An ordinal logistic regression was done to compare all death categories. The dependent variable was the death category. The independent variables were medication protocol and route of administration, using all data. A separate analysis was performed using only Academy data since it was the most detailed. Ordinal logistic regression was repeated adding the potential confounders of age, terminal diagnosis, and tolerance levels to opiates. Statistical significance was set at a two-sided p < 0.05.
Results
Overall, 3332 records were available for analysis covering 2009 through 2023. EOLWA accounted for 1612 records (48%), the Academy 1236 records (37%), EOLCOR 428 (13%), and BAEOLO 56 (2%). Table 1 summarizes the baseline demographics.
Baseline Demographics
N varied by characteristic due to availability of data from each source.
Table 2 summarizes data from the four aid-in-dying protocols we considered. The mean time to sleep across all years and medication protocols was 6.3 minutes; the median was 5.0 minutes. Table 2 shows that the mean and median time to sleep varied little across drug protocols. Due to the quantity of data analyzed, the median time to sleep was statistically significant between the medication protocols (p < 0.001). If we consider only DDMA and DDMAPh, the statistical significance is reduced (p = 0.05). Clinically, this does not make a difference.
Medication Protocols and Times to Sleep and Death
Q denotes quartile.
Comparison of only DDMA/DDMAPh median time to sleep; p = 0.05.
Comparison of only DDMA/DDMAPh median time to death; p = 0.99.
DDMA, digitalis, diazepam, morphine, amitriptyline; DDMP2, digitalis, diazepam, morphine, propranolol; DDMAPh, digitalis, diazepam, morphine, phenobarbital.
Secobarbital ingestions resulted in the most rapid median time to death: 0.4 hours. DDMP2 yielded the slowest median time to death: 1.0 hours. Median time to death was statistically significant between the four medication protocols (p < 0.001). DDMA and DDMAPh had close to equal median times time to death: both 0.8 hours (p = 0.99).
Table 3 lists the time to death for each medication protocol by death categories (successful, acceptable, problematic, disturbing, and outlier). DDMP2 achieved desired goals consistently less than the other protocols in all timeframes (p < 0.001). DDMA and DDMAPh were nearly equal (p = 0.70).
Medication Protocols and Time to Death Categories a
Chi-square test of the entire table, p < 0.001; if only comparing DDMA to DDMAPh, p = 0.70.
From 2018 to 2023, during which the medications shifted from secobarbital and DDMP2 to DDMA and DDMAPh, 17 the mean time to death declined, while the median remained relatively steady (Fig. 1). This suggests that newer medication protocols reduced the incidence of longer deaths (problematic, disturbing, and outlier).
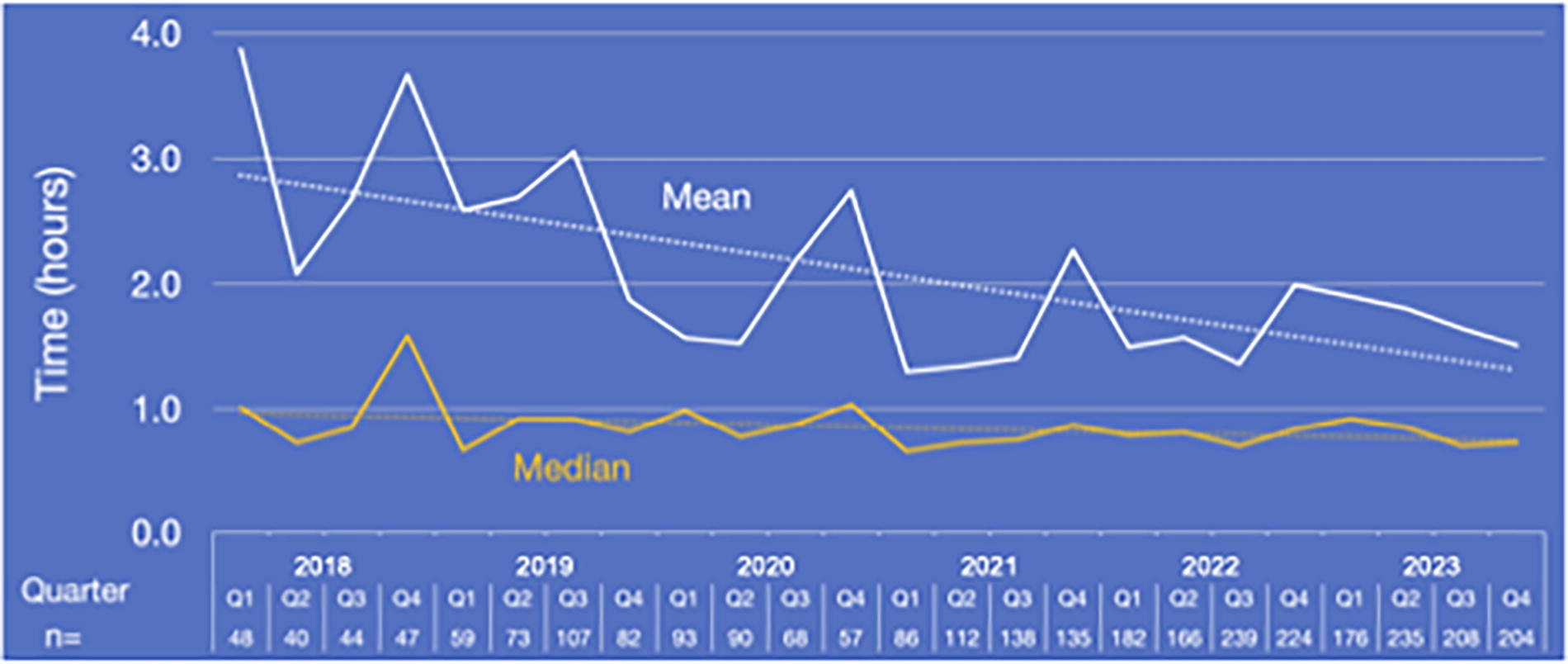
Time to death by quarter: 2018–2023. Spearman’s rank-order correlation of median is −0.045; p = 0.015.
The frequency of rectal over the oral route of medication administration, indicating practitioner awareness of upper gastrointestinal tract disease, increased over time: 2017 0.8%; 2018 0.0%; 2019 2.5%; 2020 6.2%; 2021 7.9%; 2022 11.1%; 2023 13.1% (complete data not shown).
Our data review established that, for DDMAPh, increased pre-aid-in-dying exposure to opiates was a risk factor for prolonged deaths (p < 0.001; Fig. 2). There were insufficient data to ascertain if DDMAPh compared favorably to DDMA in decreasing the prolonged deaths associated with increased opiate tolerance.
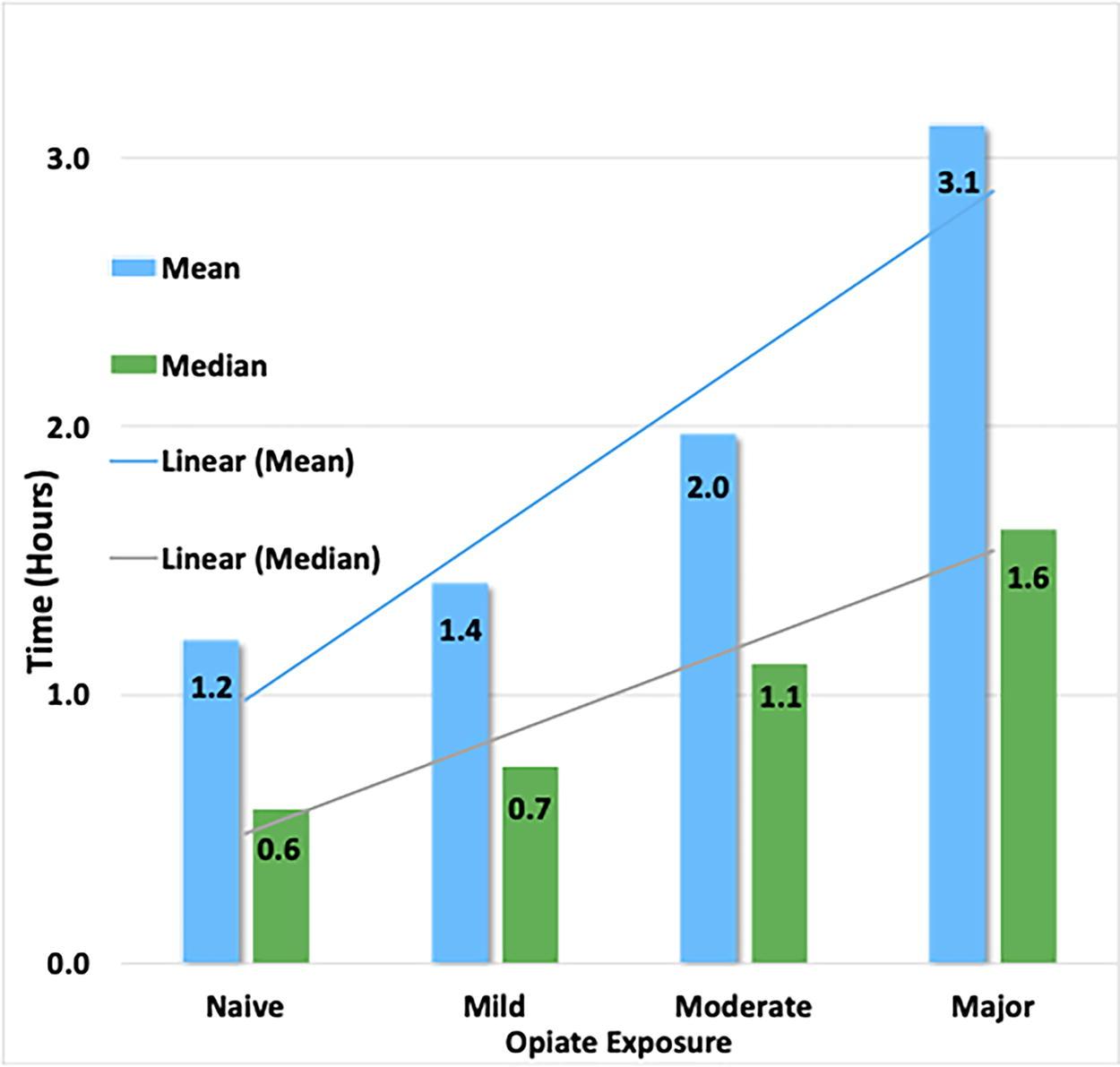
Time to death by reported prior opiate exposure. Spearman’s rank-order correlation of median is 0.26; p < 0.001.
Of note, while all the ordinal logistic regression models we calculated converged, the c-statistic that measures how well the model classifies outcomes was between 0.60 and 0.68; not adequate to use for predicting outcomes.
Discussion
In the early years of U.S. aid-in-dying pharmacology, there was no foundational knowledge or science about how to achieve a rapid, comfortable, and reliable home death. That difficulty was compounded by the legal prohibition of any injections, allowing only the self-administration of the medications by ingestion. 28 This intensified the pharmacologic challenge, since terminally ill patients rapidly approaching death commonly do not have healthy gastrointestinal tracts with intact gastric emptying, functional peristalsis, or normally absorptive intestinal mucosa.
The two most crucial variables we considered were time to sleep and time to death. A core principle of aid-in-dying pharmacology is patient comfort, so it is essential that all patients are deeply unconscious before their hearts stop. For example, it would be tragic if the cardiotoxic medications (digitalis, propranolol, and amitriptyline) caused potentially symptomatic arrhythmias in still-awake or even semi-conscious patients. The time to sleep must, with certainty, be shorter than the time to death.
Time to sleep
The mean and median times varied little across all drug protocols. Drug-induced death never preceded unconsciousness. We can inform patients with confidence that independent of the protocol used, they will be comatose before apnea or heart rhythm changes lead to death.
Time to death
Unlike times to sleep, times to death varied significantly between aid-in-dying medication protocols.
Soon after aid-in-dying legalization in 1997, the pharmaceutical focus was on briskly inducing coma by megadose oral barbiturates, assuming the brain stem would also cease driving respiration, causing hypoxia-induced cardiac arrest. 14 Secobarbital, 10,000 mg, became the most used drug. And mostly, it worked—as our pooled data and that of the Oregon Health Authority (OHA) confirmed. 16 Our data showed a median time to death of 0.38 hours, but a maximum of 1.3 days. The health authority aggregate annual data (thus not in our detailed data pool) showed a median time to death of 0.42 hours, with the range extending to 4.3 days. 10 The longer deaths indicated that coma was not consistently deep enough to reliably halt respiratory drive (apnea). These patients remained deeply unconscious until they died of complications of prolonged coma, at times days after taking the medications.
The limitations of aid in dying by secobarbital were soon intensified by exorbitant price increases and decreased availability. 29 In 2016, aid-in-dying clinicians began prescribing alternatives. By 2023, significant data had accumulated to allow for statistical comparisons of the four most common compounds.
Secobarbital ingestions resulted in the most rapid median times to death. But the range was unacceptable, indicating unreliable respiratory suppression. Additionally, secobarbital is no longer available in the United States, 30 so while the analysis of its efficacy is historically interesting, it has no practical prescribing significance. This brings our focus to the other three protocols.
The newer formulas—DDMP2, DDMA, DDMAPh—were all innovated after the limitations of secobarbital were well known. Since a different sedative taken alone seemed as likely to be an unreliable respiratory suppressant, cardiotoxic medications were added to sedatives so that cardiac arrest would occur in comatose but still-breathing patients.
DDMP2 (digitalis 50–100 mg, diazepam 1 g, morphine 15 g, propranolol 2 g)
Our data showed that DDMP2 (the first sedative/cardiotoxin combination, 2016) resulted in the longest times to death. The high-dose digitalis and propranolol were intended to drastically slow the heart rate, and post-ingestion bedside electrocardiographic rhythm monitoring showed that the intended severe bradyarrhythmias occurred reliably. 14 But many patients lived for extended periods with heart rates even in the 5–10 range—presumably because oxygen demands in the comatose patients were minimal. Deaths up to 20 hours were not unusual, with a maximum in our database of 2.6 days. Clinicians found that DDMP2 was not a satisfactory aid-in-dying formula.
DDMA (digitalis 100 mg, diazepam 1 g, morphine 15 g, amitriptyline 8 g)
DDMA employed the opposite approach from DDMP2—to induce tachyarrhythmias instead of bradyarrhythmias. Amitriptyline, a tricyclic antidepressant with a well-known toxic history from overdoses, was selected to replace propranolol. Amitriptyline causes hypotension, suppression of cardiac contractility, conduction abnormalities with QRS and QT prolongation, and ventricular arrhythmias including ventricular tachycardia followed by asystole. 31
Results with DDMA showed a marked improvement both in median and maximum times to death over DDMP2. Our data showed a maximum of 16 hours, but anecdotal reports not in our database showed occasional times to death extending beyond 24 hours. This was an improvement, but clinicians remained unsatisfied with these sporadic prolonged deaths.
DDMAPh (digitalis 100 mg, diazepam 1 g, morphine 15 g, amitriptyline 8 g, phenobarbital 5 g): All medications in DDMA require transport from the stomach to the duodenum for absorption. But gastroparesis with gastric pooling is common in patients approaching death, especially those with a history of diabetes and/or severe illness—delaying the absorption of aid-in-dying medications until they reach the duodenum. This suggested that a sedative absorbed across the gastric mucosa might improve the reliability and rapidity of sleep onset (and possibly increase respiratory suppression). We’ve found no documentation in the medical literature that such gastric absorption occurs, but the belief that it did was one reason phenobarbital was added to DDMA. More significantly, extensive aid-in-dying data had shown that patients with high levels of opiate tolerance—from their end-of-life palliative medications—experienced longer aid-in-dying deaths. Phenobarbital works at the GABA-A3 receptors, 32 bypassing tolerance at the μ opioid receptors. This augmented the rationale for prescribers to add phenobarbital to DDMA. DDMAPh use soon exceeded that of DDMA.
In our database, however, DDMAPh showed no significant time-to-death advantage over DDMA.
But while a cursory analysis of this result shows little reason to consider DDMAPh superior to DDMA, a more thorough review shows multiple reasons to conclude that using DDMAPh is advantageous. First, our DDMA versus DDMAPh data does not reflect the same time period, with DDMA used from around 2018 to 2020 versus DDMAPh 2020 through 2023. During the latter period, increasing numbers of aid-in-dying deaths were reported by Oregon, Washington, and the Academy—allowing for more patient exposures to DDMAPh (1,992) than DDMA (525), with the increased likelihood of prolonged-death outliers with DDMAPh. The data, however, do not show increased outliers with DDMAPh, indicating that the formula is bringing in those outliers more than DDMA would have done.
Additionally, in more recent years, clinicians have become accustomed to aid-in-dying care for increasingly complex patients. For example, the frequency of rectal over the oral route of medication administration — indicating practitioner awareness of upper gastrointestinal tract disease—increased over time: DDMA-predominant years, 2018 to 2020, 0% to 6.2%; DDMAPh-predominant years, 2021 to 2023, 7.9% to 13.1%. This implies that while DDMAPh seems roughly equal to DDMA in times to death, it achieved that with a more complex series of patients. Since adding phenobarbital to DDMA does not significantly increase the cost of the protocol, there seems little downside and potential benefits to adding it.
Our data confirmed that patients exposed to higher levels of opiates before aid in dying (common for patients receiving palliative care) had longer times to death (Fig. 2). But a comparison of DDMAPh to DDMA in opiate-naïve versus opiate-exposed patients was not possible due to the small number in the DDMA subset. We cannot, then, confirm or negate the hypothesis that adding phenobarbital improved outcomes for patients with higher opiate tolerance, although the reasoning appears sound, and the linear increase in time to death with level of prior opiate exposure seen in Table 2 seems to verify the hypothesis.
Similarly, sub-analyses were not performed on age, gender, route of administration, and other characteristics due to small subset sample sizes. We did observe, however, that time to death decreases steadily with increasing age (or, younger patients had longer times to death). Also, the rectal route was associated with longer times to death, likely because rectal administration is often utilized in patients with greater medical complexity. Larger sample sizes in future studies may clarify these preliminary findings.
Our overview analysis of mean versus median times to death from 2018 to 2023 (Fig. 1) confirms that accompanying the shift from DDMP2 (2016–2019) to DDMA (2018–2020) to DDMAPh (2020–2023), mean times to death correspondingly improved. But while the means showed a significant improvement, the medians indicated little change. Since improved medication efficacy would likely occur mostly in the more prolonged-death patients (those with more diseased gastrointestinal tracts and/or higher opiate tolerance), a subgroup of improvement in prolonged deaths (outliers) may be hidden in the median result. The declining means but flat medians from 2018 to 2023 confirm this explanation—indicating that prolonged-death outliers during the years with increasing use of DDMAPh were pulled down over that time period.
One motivation for improving aid-in-dying protocols was to have shorter times to death with fewer long outliers. Of note, though, is that the patients are unconscious and comfortable until death. So, the pharmacologic goal of improved times to death comes into play only if the time is excessive (closer to outliers) and problematic for family members awaiting the death. Time to sleep and time to death are, then, proxies for improved efficacy—indicating, on average, an improved experience for patients and their families. But that experience is highly individualized. We believe the decrease in prolonged death times has brought comfort to many families of aid-in-dying patients. Having said that, it is clear there is still room for improvement in reducing times to death.
A confounding variable to consider in these descending times to death includes the likelihood of increased skills of aid-in-dying clinicians in the latter years, potentially intersecting with the improved pharmacology.
We acknowledge the limitations of our data pool, reflecting information from four non-government sources. Many states with legalized aid in dying do collect data, but they report only aggregates and summaries16,23,24—so individual data points cannot be analyzed by nonstate investigators. Additionally, only Oregon includes information on specific medication protocols. 17 California’s reports, for example, cite only “a combination of cardiotonic, opioid, and sedatives” without separating out the various medication regimens. 24 The state does collect information about the specific medication protocols used but does not make that available to the public or nonstate investigators. When possible, we compared our conclusions with those of the state data summaries and found corresponding trends, although specific calculations could not be compared. For future improvements in the understanding of aid-in-dying pharmacology, we urge state health departments to provide full anonymized data to independent investigators, in addition to releasing public summaries.
Conclusions
Our analysis of pooled data regarding aid-in-dying pharmacologic protocols is the first to analyze clinical outcomes related to successive formula innovations over a 26-year period. We conclude that DDMAPh is the most effective and reliable medication protocol for aid in dying. For patients and loved ones at the bedside, clinicians can now provide specific information about the outcomes of aid-in-dying deaths with DDMAPh: 93.2% under 5 hours (successful/acceptable), with only 0.4% of deaths in the >20-hour (outlier) category. While there may be other variables at play, the data at this time is sufficient to recommend the use of DDMAPh over all preceding protocols.
Footnotes
Acknowledgments
The authors are grateful to the organizations End of Life Choices Oregon and End of Life Washington, who shared their data on aid-in-dying outcomes. We are deeply appreciative of Dr. Carol Parrot’s work toward the improvement of aid-in-dying pharmacology.
Authors’ Contributions
P.M.: Review and editing (equal) and conceptualization (co-lead). S.H.: Review and editing (equal) and statistical analysis (co-lead). A.L.: Review and editing (equal) and statistical analysis (co-lead); L.S.: Review and editing equal, conceptualization (co-lead), and original draft (lead).
Author Disclosure Statement
The authors have no conflicts of interest.
Funding Information
No funding was received for this article.