
Abstract
Dear Editor:
Palliative care should be involved in the management of patients with refractory gastroparesis, a life-limiting condition that significantly impairs quality of life and often requires multiple medical or surgical interventions.
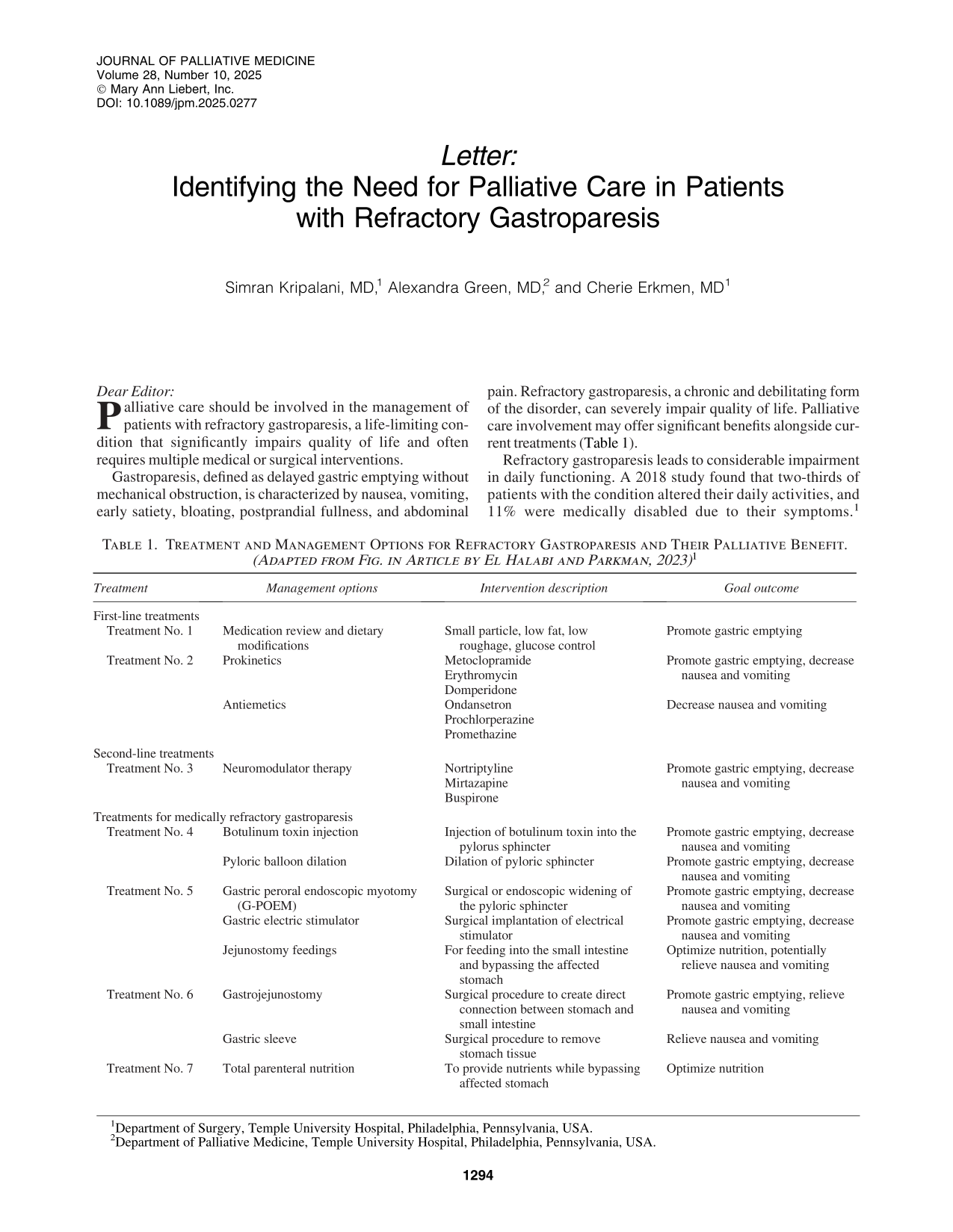
Gastroparesis, defined as delayed gastric emptying without mechanical obstruction, is characterized by nausea, vomiting, early satiety, bloating, postprandial fullness, and abdominal pain. Refractory gastroparesis, a chronic and debilitating form of the disorder, can severely impair quality of life. Palliative care involvement may offer significant benefits alongside current treatments (Table 1).
Treatment and Management Options for Refractory Gastroparesis and Their Palliative Benefit. (Adapted from Fig. in Article by El Halabi and Parkman, 2023) 1
Refractory gastroparesis leads to considerable impairment in daily functioning. A 2018 study found that two-thirds of patients with the condition altered their daily activities, and 11% were medically disabled due to their symptoms. 1 In addition to reduced quality of life, these patients frequently experience higher health care utilization and costs. Many also have comorbidities and mental health challenges, such as anxiety and depression, which further exacerbate the negative impact on their lives. 2
Palliative care providers commonly treat nausea and vomiting, which are common in gastroparesis patients. A study found that 95% of patients reported nausea. 3 These symptoms, coupled with the difficulty in tolerating or enjoying food, can lead to social isolation and emotional distress. Since food is central to many social interactions, the inability to engage in meals can cause patients to feel disconnected from normal life. Psychosocial support from palliative care providers can be vital, as many patients with refractory gastroparesis experience high rates of anxiety and depression. 4
Patients with refractory gastroparesis often require procedures to address symptoms that fail conservative management. Surgical options, such as gastric stimulator placement or gastric peroral endoscopic myotomy, can facilitate gastric emptying, potentially reducing nausea and improving oral intake. Other palliative interventions, like jejunostomy tube placement or total parenteral nutrition, may provide nutritional support but do not address the underlying gastroparesis. Before considering surgery, it’s important to have clear discussions with patients about the goals, risks, and benefits of interventions. Some patients may be unwilling to consider open surgery or face the potential for reoperation. Other patients may not be adequate surgical candidates given poor nutritional status and other comorbidities that put them at higher risk for complications. Surgical complications such as small bowel obstructions, tube dislodgement, or peritonitis must also be considered in decision-making. Inadequate nutrition due to underlying nausea and vomiting may also increase the potential for postoperative complications and infections leading to prolonged hospitalization. Understanding the patient’s values and limits is crucial in guiding treatment decisions and tailoring the management approach for gastroparesis.
Refractory gastroparesis is a complex condition that often requires more than medical therapy. Effective symptom and psychosocial support not only help patients cope with the challenges of their illness but also improve their ability to tolerate nutrition and continue treatment—much like how symptom management enables cancer patients to complete chemotherapy. Palliative care should be seen as an essential component of treatment, offering symptom control, psychosocial support, and value-based guidance to improve the patient’s quality of life and help establish goal-concordant care.