
Abstract
Human decellularized adipose matrix (hDAM) has emerged as a promising, off-the-shelf option for soft tissue augmentation, providing a biocompatible scaffold that supports angiogenesis, adipogenesis, and volume retention with minimal immunogenicity. This systematic review synthesizes preclinical and clinical evidence on hDAM’s regenerative potential, focusing on its capacity to integrate with host tissue and enhance volume retention. A comprehensive literature search was performed across multiple databases yielding 21 studies (14 preclinical, 6 clinical, and 1 combined) that met eligibility criteria. Risk of bias (RoB) was evaluated for animal and human studies using the Collaboration for the Assessment of Risks and Benefits of Anticancer Therapies (CAMARADES) and RoB In Nonrandomized Studies of Interventions (ROBINS-I) tools, respectively. Key preclinical findings indicate that hDAM supports progressive angiogenesis and adipogenesis, with significant weekly increases in vessel formation and adipocyte development. Linear mixed models were used to quantify these rates, showing an increase of 0.366% per week (p < 0.001) in the percentage of CD31+ positive area, and a 3.88% rise in perilipin-positive area per week (p < 0.001), representing angiogenesis and adipogenesis, respectively. Variability in regeneration rates underscores the influence of different hDAM preparation methods, such as enzyme-free decellularization and ultrasonication, which have been shown to improve cell compatibility and volume retention. Clinical studies demonstrate that hDAM achieves notable volume retention and patient satisfaction, particularly in facial and body contouring applications, while also improving skin texture, tone, and functionality. Compared with traditional autologous fat transfer and synthetic fillers, hDAM offers advantages in integration, resorption rates, and low complication risks, without donor site morbidity. Limitations of current studies include variability in hDAM preparation techniques, inconsistent outcome measures, and a paucity of long-term follow-up data. This review establishes hDAM as a safe and effective scaffold for soft tissue regeneration and provides a quantitative analysis of its regenerative timeline. Standardizing preparation methods and outcome measures, coupled with more randomized clinical trials, will be essential for optimizing treatment protocols. Future directions include exploring patient-specific factors and combination therapies to enhance hDAM’s applicability in reconstructive and aesthetic surgery.
Impact Statement
This systematic review highlights the potential of human decellularized adipose matrix (hDAM) as an off-the-shelf solution for soft tissue regeneration, offering advantages over traditional autologous fat transfer and synthetic fillers. By quantitatively analyzing hDAM’s angiogenic and adipogenic properties, this review provides a framework for clinicians to optimize their treatment protocols to maximize volume retention and tissue integration. Standardizing hDAM preparation and outcome measures can enhance its clinical utility, while future studies targeting patient-specific factors will foster the development of personalized reconstructive and aesthetic interventions.
Keywords
Introduction
Plastic and reconstructive surgeons continually strive to improve soft tissue augmentation techniques for addressing diverse reconstructive needs—from postmastectomy body contouring to restoring congenital defects. Autologous fat grafting and synthetic fillers are commonly used for these purposes and provide temporary to semipermanent solutions. However, while autologous fat transfer (AFT) is highly biocompatible, it presents limitations including variability in graft survival, donor site morbidity, and inconsistent aesthetic outcomes.1,2 Synthetic fillers, although accessible, may provoke immune reactions and lack the regenerative properties desired for long-term tissue integration.3–7 Autologous tissue remains the preferred method for repairing soft tissue defects from trauma, tumor removal, or congenital issues due to its high compatibility with native tissue and low complication rates.8,9
Human decellularized adipose matrix (hDAM)—also known as decellularized adipose tissue (DAT) and allograft adipose matrix (AAM)—is a promising alternative derived from donated adipose tissue. It is processed to remove cells while preserving extracellular matrix components, which supports cell proliferation, angiogenesis, and adipogenesis. These components enable hDAM to recruit host cells with minimal immunogenicity, allowing it to serve as a scaffold for soft tissue regeneration and function as a potential standalone filler.10–14
The advantages of hDAM include its integration with host tissues, minimal adverse reactions, and no donor site morbidity. hDAM can also be used alongside AFT to augment results when larger volume corrections are needed.10,15
Despite the increasing interest in hDAM as a substitute for autologous fat and synthetic fillers, there remains a significant gap in understanding its full clinical potential. The regenerative effects of hDAM in promoting adipogenesis and angiogenesis are noted in various studies; however, the literature lacks a comprehensive quantitative analysis examining how these processes progress over time in a controlled model.16,17 In addition, the paucity of randomized clinical trials contributes to uncertainties clinicians face regarding optimal injection sites, volumes, and follow-up times.
This review addresses these gaps by systematically synthesizing preclinical and clinical findings to provide a more precise, data-driven understanding of hDAM’s biological activity. By calculating the rates of adipogenesis and angiogenesis in controlled murine models, this review will quantify the regenerative potential of hDAM and establish predictive parameters to aid in clinical decision-making. In addition, a comprehensive review of findings from human studies will help translate preclinical efficacy into clinical expectations, while identifying gaps in current research to guide future investigations into hDAM modifications and combined regenerative treatments.
Ultimately, this review highlights hDAM’s potential as a dependable, off-the-shelf soft tissue filler, establishing a foundation to refine clinical applications and guide targeted research for enhancing its regenerative capabilities.
Methods
Search strategy
A systematic literature review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (registration number: CRD42024573297). 18 The search was performed on February 13, 2024, utilizing PubMed, OVID, EMBASE, and Scopus databases. The search terms focused on decellularized adipose matrices and soft tissue regeneration or aesthetic indications, and results were limited to articles published in English. To address a limitation of data, an expanded search was conducted on May 7, 2024, to include animal studies reporting histological outcomes. PubMed, Embase, Scopus, Web of Science, and Cochrane databases were queried. The full list of search terms used is available in Table 1.
(A) Original Search Terms and (B) Expanded Search Terms

Screening process
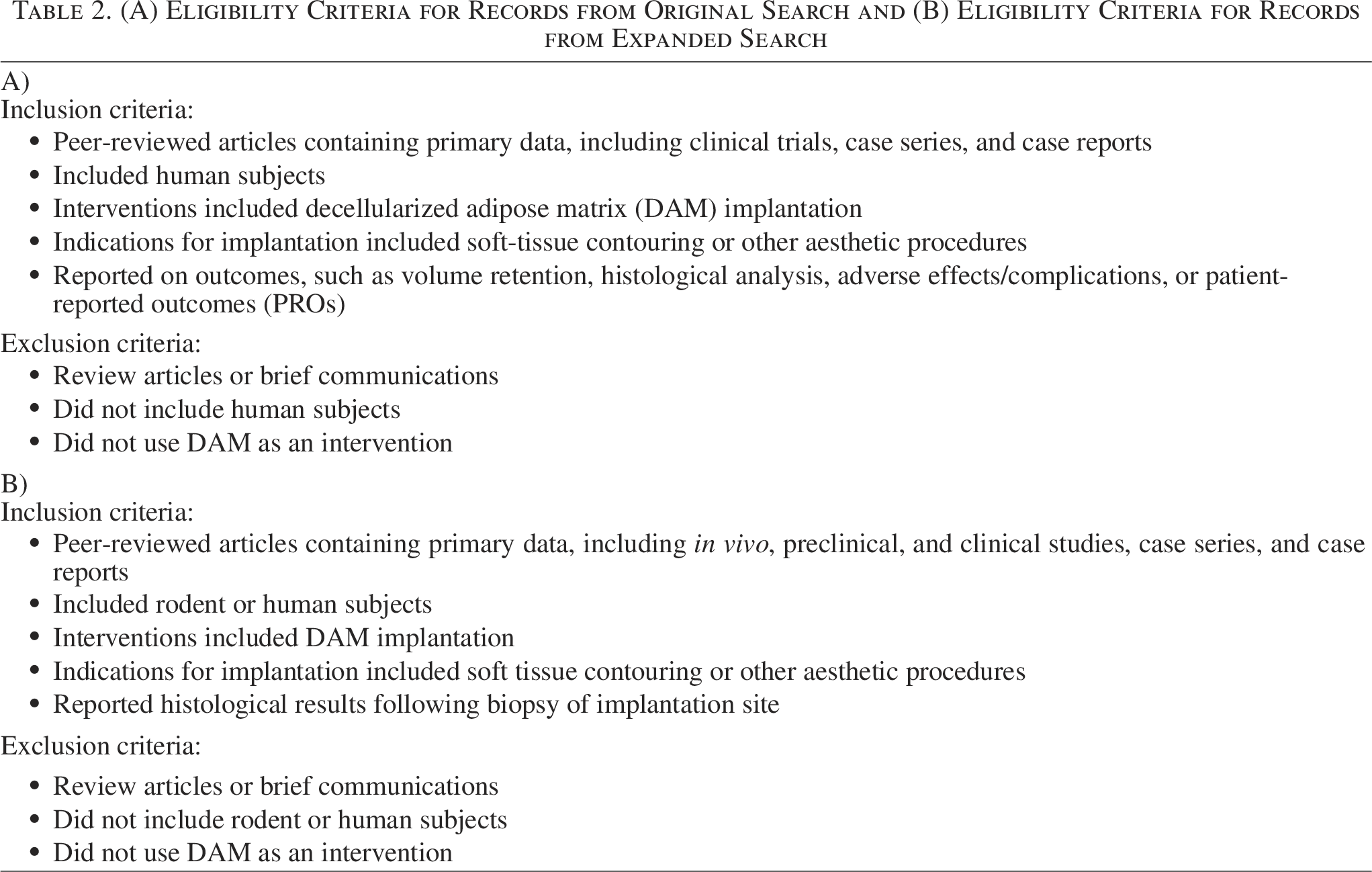
The identified records from each search were uploaded to Rayyan (Rayyan Systems Inc., Cambridge, MA, USA) and duplicates were removed. Two independent blinded reviewers screened titles and abstracts according to predefined eligibility criteria, and a third reviewer resolved conflicts. The full texts of selected articles were screened using the same process, and data were extracted from all studies. The detailed inclusion and exclusion criteria for both the original and expanded searches are outlined in Table 2.
(A) Eligibility Criteria for Records from Original Search and (B) Eligibility Criteria for Records from Expanded Search
Data collection process
The following data were extracted from clinical studies with human subjects: author, publication year, title, study type, number of subjects, gender, age, race/ethnicity, experimental groups, indications, location of injection, volume of hDAM injected, frequency of injections, assessment time points, method of assessing volume retention, average volume retention (%) per time point, method of assessing atrophy, atrophy for each time point [average ± standard deviation (SD)], weight/body mass index (BMI), study objectives, histological results, photographic results, complications, scoring systems utilized, overall findings, and limitations.
The following data were extracted from preclinical studies with rodent subjects: author, year, title, species of donated adipose, species of biopsied subjects, location of hDAM implantation/biopsy, subject groups, follow-up time points postimplantation, biopsy time points, number of subjects per group, method of assessing angiogenesis and adipogenesis, units for results, and results.
Risk of bias
In the risk of bias (RoB) assessment, two distinct tools were used by two independent reviewers who were blinded to each other’s assessments. The Collaboration for the Assessment of Risks and Benefits of Anticancer Therapies (CAMARADES) RoB tool was utilized to assess the quality of animal studies. This widely used and validated tool uses 10 questions to evaluate RoB in animal studies across five domains: randomization, blinding, incomplete outcome data, selective reporting, and other biases, which aim to identify additional potential sources of bias such as conflicts of interest or funding issues. Each animal study was classified as having a low, unclear, or high RoB based on how well the study addressed potential issues.
The RoB In Nonrandomized Studies of Interventions (ROBINS-I) tool was utilized to assess the RoB in human studies. This is tailored specifically for nonrandomized studies of interventions and ensures that the tool addresses biases that are unique to observational studies and other nonrandomized designs. For these cases, each criterion is categorized as either low, moderate, serious, or critical RoB. It also provides a detailed framework for assessing RoB across multiple domains. Upon the completion of the RoB evaluation, a third reviewer resolved discrepancies that had been identified initially.
Statistical analysis
Data collection and organization were managed using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and Google Sheets (Google LLC, Mountain View, CA, USA), while all statistical analyses were conducted using R (version 4.4.1, R Foundation for Statistical Computing, Vienna, Austria). To permit analysis, data were converted to similar units, when possible. Linear mixed models were utilized to assess the relationship between time postimplantation and the outcomes of interest (angiogenesis and adipogenesis), accounting for variability across different studies. The models included time postimplantation (in weeks) as a fixed effect to assess the rate of change in angiogenesis and adipogenesis over time and random effects were examined to understand the degree of variability across studies. The models were fit using restricted maximum likelihood estimation, and the significance of the fixed effects was assessed using t-tests. Growth curves for each outcome measure were plotted to illustrate estimated changes over time. p-Values < 0.05 were considered statistically significant.
Results
Search results
Our systematic literature search identified 14 murine/preclinical studies, 6 human/clinical studies, and 1 study reporting results from both, for a combined total of 21 studies included in the final review (Fig. 1). Upon selection, murine studies were assessed for RoB using the CAMARADES RoB tool, while the ROBINS-I tool was applied to human studies.
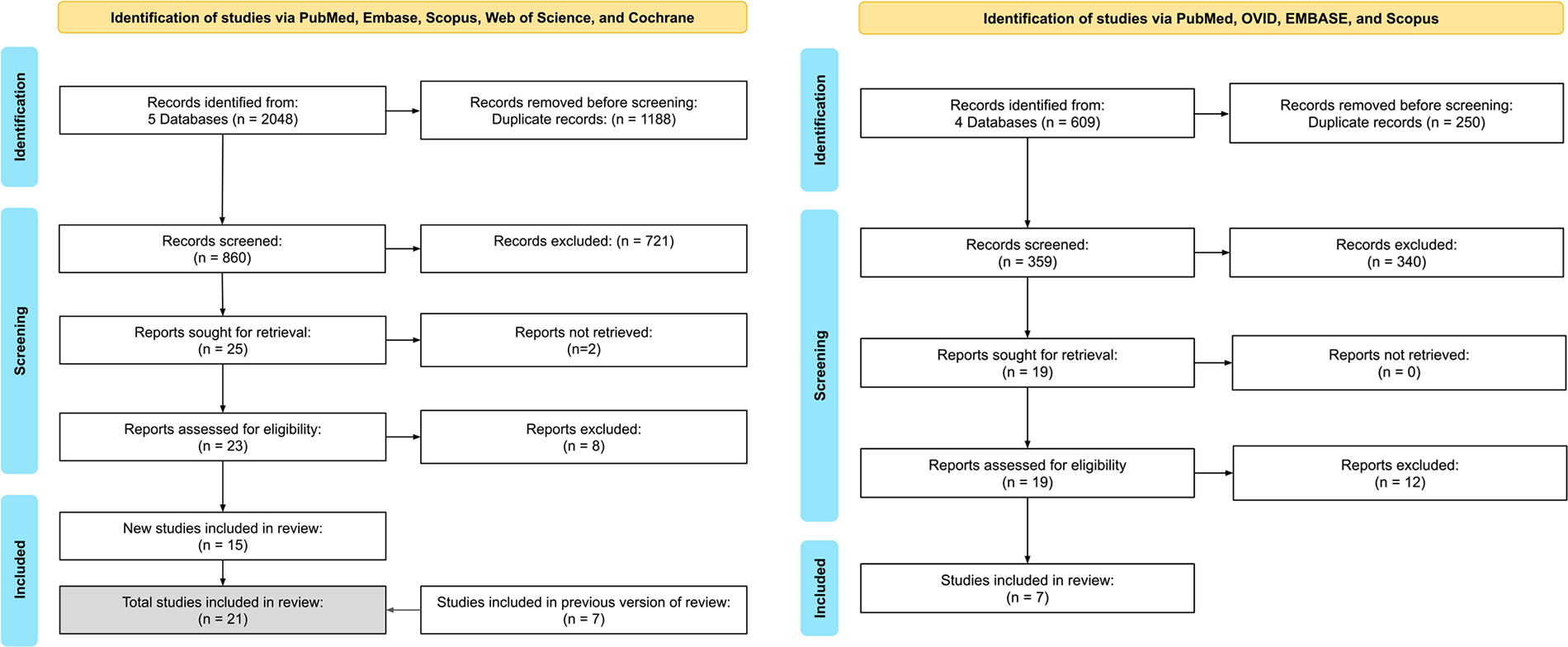
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagrams for initial search (right) and expanded search (left).
Results of RoB
Human studies were assessed for RoB using the ROBINS-I tool (Fig. 2). Most studies exhibited moderate to high RoB due to factors such as lack of randomization, inconsistent reporting of blinding, and failure to control for confounding variables such as patient demographics and preexisting conditions. Notably, Kokai (2019) demonstrated an overall low RoB, while studies such as Gold (2020), Gold (2023), and Anderson (2022) presented several potential biases, particularly in subjective outcome assessments due to a lack of blinding and randomization.13,19–21

Risk of bias (RoB) analysis of clinical human studies using the RoB In Nonrandomized Studies of Interventions (ROBINS-I) tool.
Animal studies, evaluated with the CAMARADES tool (Fig. 3), generally adhered to animal welfare regulations and used appropriate models. However, many failed to provide sample size calculations or employ methods to control for multiple tests. For example, Tang (2022) exhibited high RoB, missing several key domains such as randomization and blinding. 22 In contrast, Giatsidis (2018) and Kim (2024) demonstrated low RoB, addressing most relevant domains.12,23
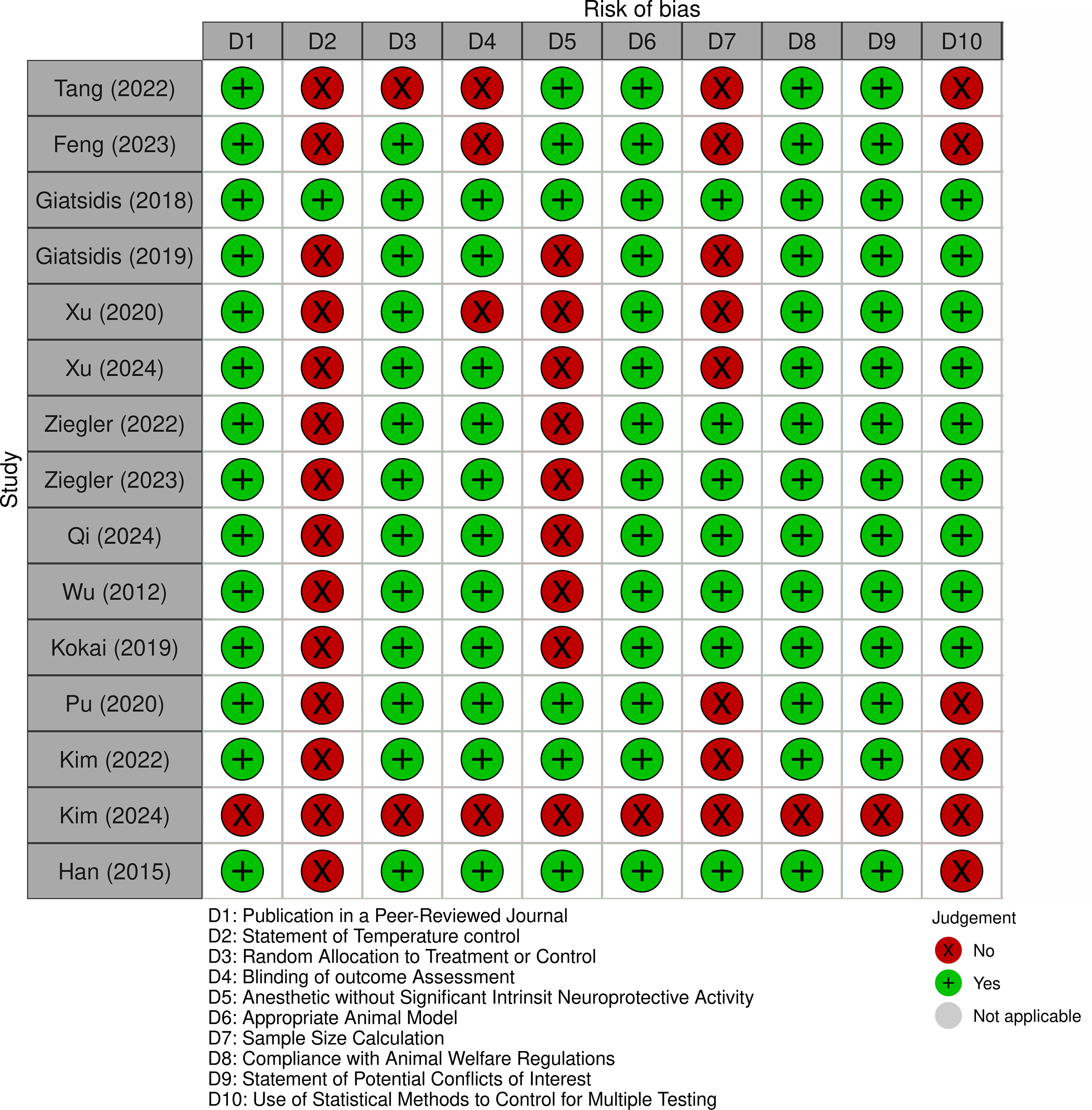
Risk of bias (RoB) analysis of preclinical murine studies using the Collaboration for the Assessment of Risks and Benefits of Anticancer Therapies (CAMARADES) tool.
Preclinical studies
The ability of isolated hDAM implantations to promote angiogenesis and adipogenesis was evaluated in several preclinical studies (Table 3). Following implantation into rodents, biopsies were collected at various time points to permit histological analysis. Samples were stained with anti-perilipin and anti-CD31 antibodies to quantitatively assess adipogenesis and angiogenesis, respectively, and results were reported as percentage of positively stained area (% positive area) or number of vessels/adipocytes per field (# per field).
Effects of hDAM on Adipogenesis and Angiogenesis in Preclinical Murine Studies
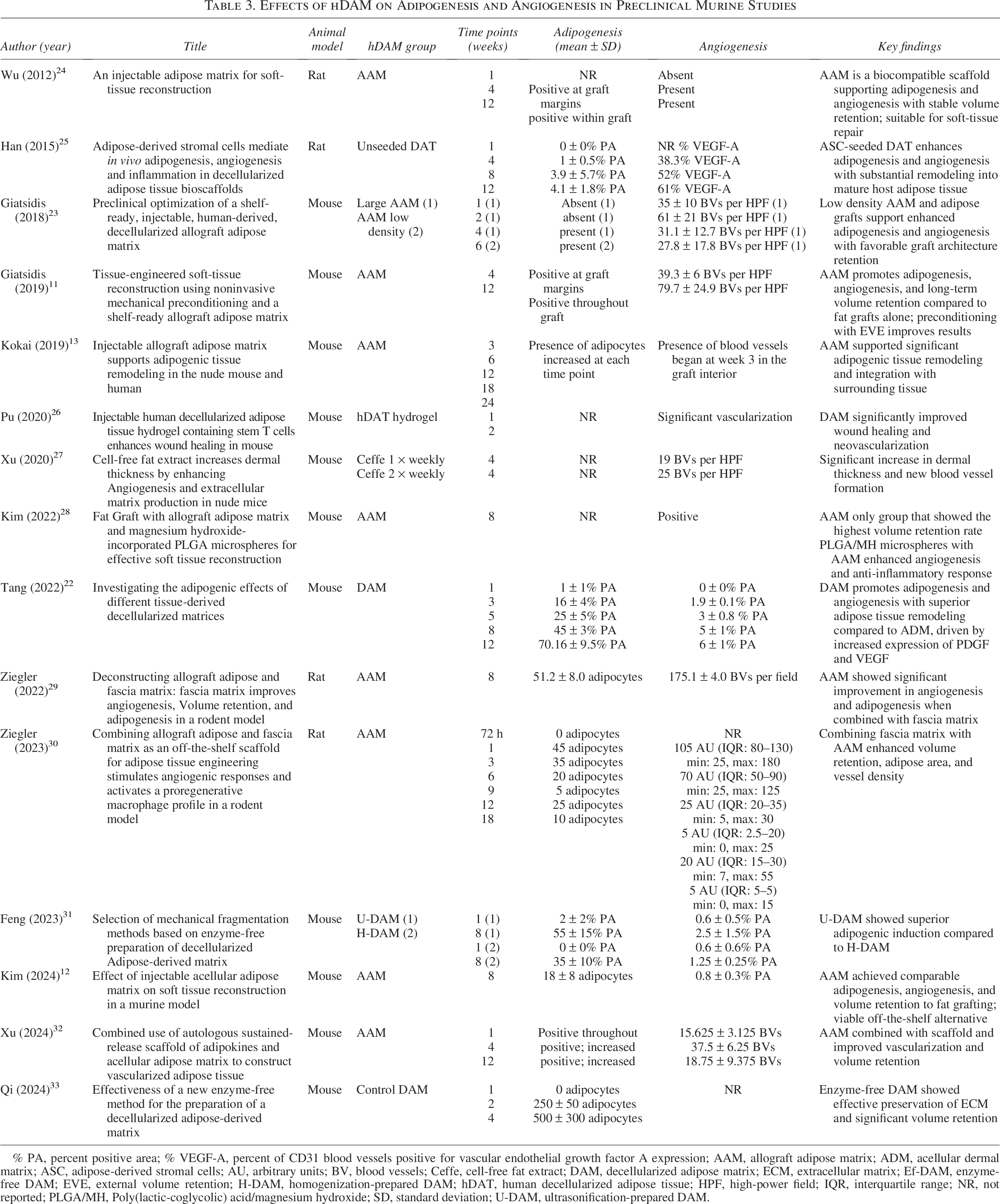
% PA, percent positive area; % VEGF-A, percent of CD31 blood vessels positive for vascular endothelial growth factor A expression; AAM, allograft adipose matrix; ADM, acellular dermal matrix; ASC, adipose-derived stromal cells; AU, arbitrary units; BV, blood vessels; Ceffe, cell-free fat extract; DAM, decellularized adipose matrix; ECM, extracellular matrix; Ef-DAM, enzyme-free DAM; EVE, external volume retention; H-DAM, homogenization-prepared DAM; hDAT, human decellularized adipose tissue; HPF, high-power field; IQR, interquartile range; NR, not reported; PLGA/MH, Poly(lactic-coglycolic) acid/magnesium hydroxide; SD, standard deviation; U-DAM, ultrasonification-prepared DAM.
To analyze the relationship between time postimplantation and outcome, we performed a linear mixed model analysis for both metrics, including time as a fixed effect and cross-study variability as a random effect. At time = 0, angiogenesis and adipogenesis were assumed to be negligible.
Results from Feng (2023), Tang (2022), and Kim (2024) reported angiogenesis as a % positive area.12,22,31 The analysis revealed a significant increase of 0.366% per week (p < 0.001), suggesting progressive angiogenesis in the weeks following hDAM implantation (Fig. 4). Variability across studies was moderate, as indicated by a random effect variance of 0.4346.
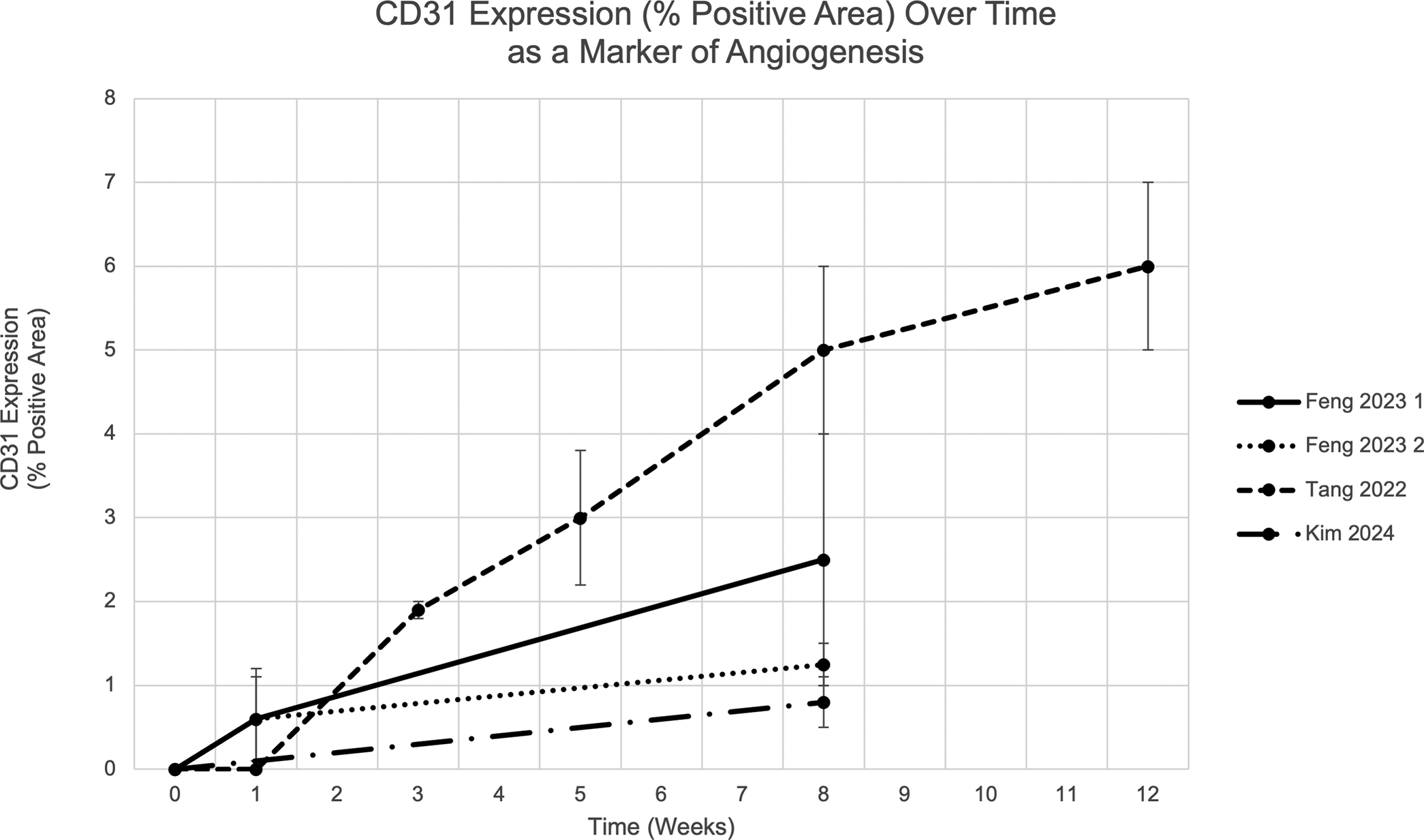
Rate of angiogenesis, measured as percent positive area of CD31 expression per field, following hDAM implantation at week = 0. hDAM, human decellularized adipose matrix.
In studies by Giatsidis (2018), Giatsidis (2019), and Xu (2024), angiogenesis was reported as # per field.11,23,32 The analysis showed a statistically significant increase of approximately 3.461 vessels per week (p < 0.05) (Fig. 5). Substantial variability in baseline angiogenesis was observed across studies, with a random effect variance of 27.63.
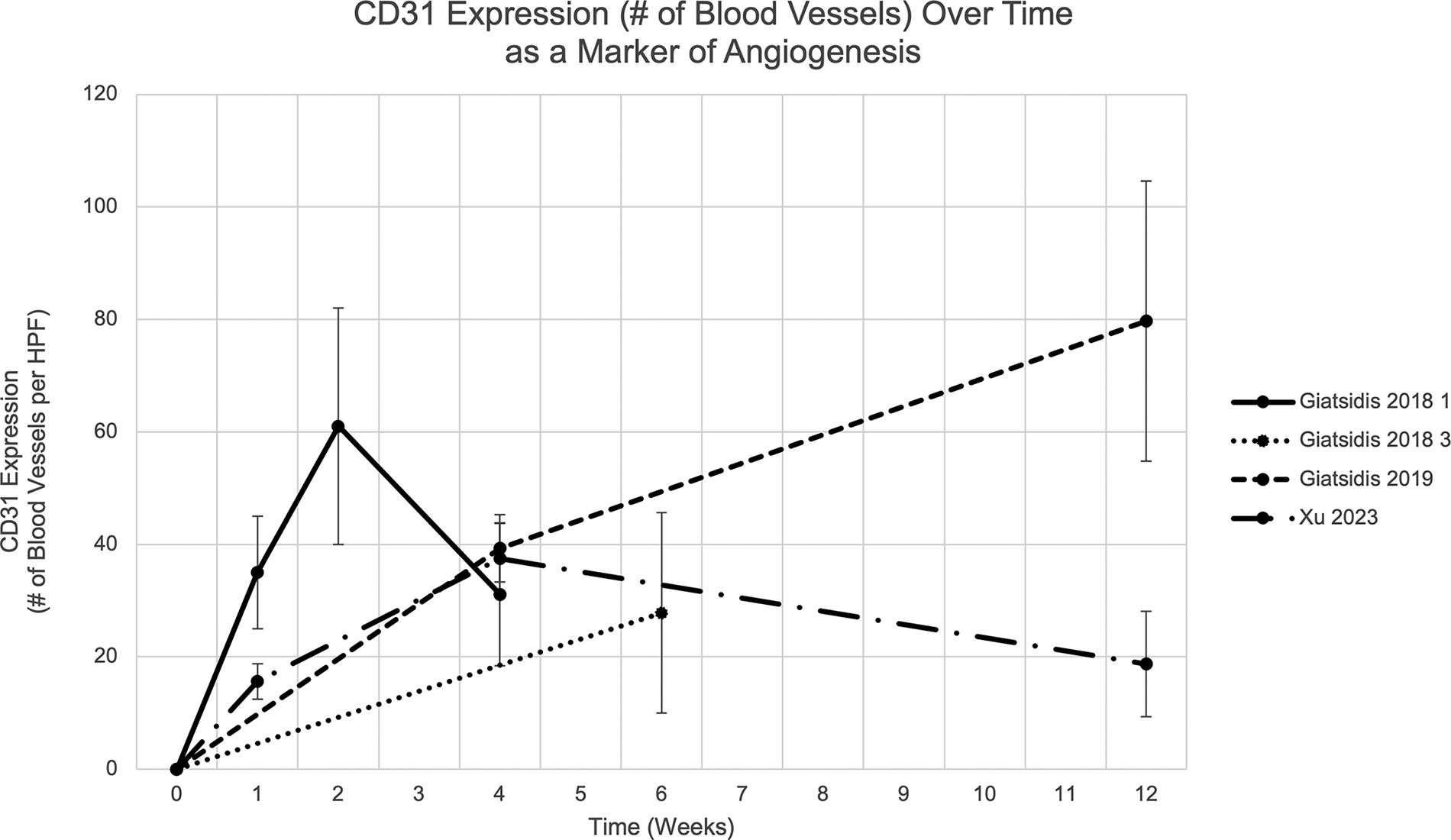
Rate of angiogenesis, measured as the number of blood vessels positive for CD31 expression per field, following hDAM implantation at week = 0.
Adipogenesis was quantified in studies by Feng (2023), Tang (2022), and Han (2015) using % positive area.22,25,31 The analysis indicated a significant increase in adipogenesis over time, with an estimated rise of 3.88% per week (p < 0.001), pointing to a steady enhancement of adipose tissue formation postimplantation (Fig. 6). Variability across studies was substantial (random effect variance = 109.5), yet the general trend of increasing adipogenesis was consistent.

Rate of adipogenesis, measured as percent positive area of perilipin expression per field, following hDAM implantation at week = 0.
hDAM modifications
In recent years, various techniques have been developed to improve the preparation and performance of hDAMs (Table 4).
hDAM Preparation Methods

An enzyme-free (EF) decellularization method has been explored by Qi et al. as an alternative to the more expensive and time-consuming enzyme-based method. This EF method effectively removes cellular components and preserves hDAM’s microstructure promoting adipose tissue regeneration. When cocultured with human adipose-derived stem cells (hADSCs), the EF prepared hDAM exhibited excellent cytocompatibility, with enhanced hADSC adhesion and proliferation rates. In addition, they demonstrated significantly increased adipocyte formation and retention with EF DAM in rodent models suggesting its superior capacity for adipogenesis and long-term volume stability. 33
Feng et al. used an EF preparation method, comparing ultrasonication DAM (U-DAM) with homogenization DAM (H-DAM). U-DAM facilitated earlier adipocyte appearance by week 1, with more vigorous regeneration by 8 weeks compared with H-DAM. Locally, immature multilocular adipocytes were observed in U-DAM at week 1, while no adipocytes were seen in H-DAM. By week 8, both groups exhibited large numbers of mature adipocytes, but regeneration was more pronounced in U-DAM. In addition, U-DAM showed superior angiogenic induction, with significant capillary formation 1 week postimplantation. Although both groups displayed comparable angiogenesis at both time points, U-DAM exhibited more efficient overall adipose tissue regeneration. Ultrasonication produced the thinnest middle layer and left most cells dead, indicating effective decellularization. 31
Han et al. demonstrated that adipose-derived stromal cells seeded onto hDAM significantly promoted adipogenesis, evidenced by increased perilipin expression over time. 25 Xu et al. further supported this, showing that a sustained-release scaffold in combination with hDAM led to enhanced adipogenesis, with volume retention varying from 100% to 44.00 ± 8.76% in the hDAM plus adipose collagen fragment (ACF) group and 47.33 ± 15.68% in the hDAM group. 27
Tang et al. compared hDAM and acellular dermal matrix (ADM) and found that hDAM implants remodeled into mature adipose tissue by week 12, with greater neovascularization and adipogenic marker expression compared with ADM. Hematoxylin and eosin (H&E) staining revealed scaffold cellularity was enhanced in the hDAM group at weeks 3, 5, and 12, with adipocytes aggregating and slowly occupying the implant over time. Infiltrating cells decreased in the ADM group, and virtually no adipocytes were observed. However, collagen retention was improved in the ADM group with 96.48 ± 4.13% and 92.48 ± 2.34% retention at weeks 3 and 8, respectively, compared with the hDAM group demonstrating 77.39 ± 4.25% and 51.50 ± 6.95% collagen retention at both time points. 22
In addition to supporting adipogenesis, several studies have highlighted the angiogenic potential of decellularized adipose matrix-based hydrogels. Wu et al. showed that AAM supported adipose tissue formation at the periphery of the implant, with vascularization observed as early as 2 weeks postimplantation. By 12 weeks, substantial adipose tissue had developed within the matrix, suggesting that AAM not only facilitated adipogenesis but also promoted long-term volume retention without significant inflammatory reactions. 24 Pu et al. investigated the efficacy of an injectable hDAT hydrogel (hDAT-gel) combined with hADSCs in promoting wound healing and angiogenesis in a full-thickness cutaneous wound mouse model. Their results demonstrated that hDAT-gel containing hASCs significantly accelerated wound healing compared with control groups, with prominent neovascularization observed within 7 days. Histological and immunofluorescence analyses confirmed increased microvessel formation in the hDAT-gel + hASCs group, particularly through CD31-positive endothelial cell staining. 26
Ziegler et al. found that combining hDAM with fascia matrix significantly increased CD31+ cells, with a 23% increase (p < 0.05) compared with hDAM alone. The 50/50 mixture of fascia matrix and hDAM also showed a 7% increase in CD31+ cells (p < 0.05). In addition, fascia matrix alone and the 50/50 mixture revealed greater volume retention (0.70 ± 0.08 and 0.60 ± 0.14, respectively; p < 0.05 for both) compared with hDAM alone (0.25 ± 0.13). 29 They also noted that combining hDAM with fascia matrix significantly improved volume retention compared with hDAM alone, with the 50/50 fascia mixture showing a 1233% greater volume retention compared with hDAM alone at 18 weeks.29,30
Giatsidis et al. observed that cyclical external volume expansion (EVE) preconditioning significantly increased the density of capillaries surrounding and invading hDAM grafts, with a 1.6-fold ± 0.2 increase at a 12-week follow-up (p < 0.05), while continuous EVE did not significantly induce angiogenesis compared with controls. They also examined the effects of scaffold configuration and mechanical preconditioning on volume retention. Small hDAM grafts, particularly when preconditioned with cyclical EVE, showed improved long-term volume retention, with a 1.4-fold ± 0.2 increase in cross-sectional area over time (week 4 vs. week 1, p < 0.05). In contrast, larger hDAM grafts triggered a more intense inflammatory reaction, though cyclical EVE still enhanced long-term perigraft angiogenesis.11,23
Kim et al. tested an injectable hDAM combined with magnesium hydroxide-incorporated poly(lactic-coglycolic) acid (PLGA) microspheres and found that this combination significantly improved volume retention compared with fat grafts alone. The hDAM + PLGA group showed a 50% retention volume whereas the fat graft group only showed a 12.5% retention volume. 28 This aligns with the findings from Giatsidis and Ziegler, highlighting the importance of scaffold composition and bioactive components in enhancing volume retention in hDAM applications.
Clinical studies
The safety and efficacy of hDAM have been investigated in various clinical settings (Table 5). In a multicenter, open-label pilot study in 2020, Gold et al. evaluated the use of hDAM (Renuva®, MTF Biologics) in 10 patients for the correction of bilateral temple atrophy. Patients showed a mean increase in fullness from baseline immediately after treatment (0.0 pretreatment to 2.8 posttreatment, on a 0–4 scale). Volume retention was maintained for up to 24 weeks with approximately 75% retention. Importantly, the study reported a notable improvement in skin tone, smoothness, and texture, with 71% of subjects expressing satisfaction with the aesthetic outcomes. Histological analysis revealed the incorporation of native adipocytes and endothelial cells into the matrix, suggesting that hDAM supports both adipogenesis and angiogenesis in vivo. Adverse events were minimal, limited to transient discomfort and mild swelling. 21
Effects of hDAM on Adipogenesis, Angiogenesis, Volume Retention, and Safety in Clinical Human Studies
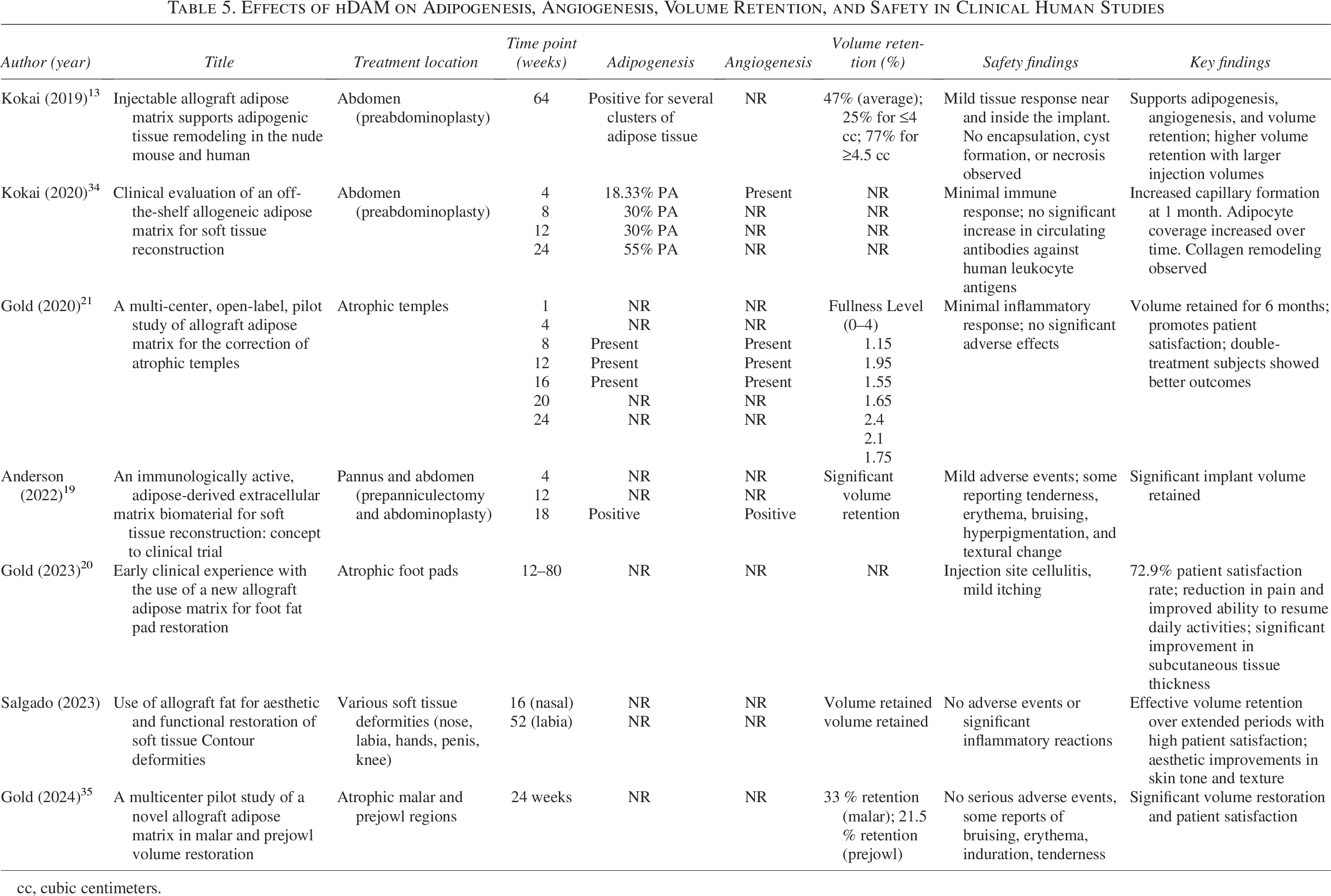
cc, cubic centimeters.
In a 2024 study by Gold et al., hDAM was found to effectively promote adipogenesis and sustained volume retention in malar and prejowl facial restoration procedures. The study observed increases in the % perilipin positive area over time, with approximately 33 ± 30% volume retained in the malar region and 21.5 ± 15.2% in the prejowl region at 24 weeks. Skin condition improved throughout the study, and at 24 weeks, the % of tone improvement was 54.3% for malar and 58.1% for prejowl; smoothness improvement was 62.1% for both; and texture improvement was 60.0% for malar and 61.9% for prejowl regions. 35
Kokai et al. (2019) assessed the impact of different hDAM configurations and preparation methods on volume retention in the dorsal wrist, finding that larger injection volumes correlated with higher retention rates. For injections of 4 cc or less, volume retention was approximately 25%, compared with 77% for injections of 4 cc or more. Average graft retention at 16 weeks was correlated as 47% relative to the initial injection volume. In addition, the prominence of veins and tendons at the dorsal wrist decreased after injection, and skin thickening quality enhanced throughout follow-up. 13 In another study, Kokai et al. injected hDAM into the pannus of 10 patients, and they reported new capillaries formed as early as 1 month post-hDAM pannus injection but then decreased in size over the remainder of the study. 34
Gold et al. (2023) evaluated the efficacy of hDAM for pedal fat pad restoration in 16 patients (21 feet) experiencing foot pain due to fat pad atrophy. The study reported a 72.9% patient satisfaction rate, with a reduction in pain and improved ability to resume daily activities. Follow-up ultrasound imaging demonstrated significant improvements in subcutaneous tissue thickness, contributing to enhanced cushioning and skin quality at the treatment sites. 20
Discussion
The systematic review reveals that hDAM significantly promotes angiogenesis and adipogenesis, key processes necessary for successful tissue regeneration and repair. Studies report increased CD31 expression after injections, suggesting hDAM effectively stimulates the formation of new blood vessels to supply nutrients and oxygen to regenerating tissues. Similarly, studies report increased perilipin expression demonstrating hDAM’s ability to support the formation of new adipose tissue.
Clinical relevance of quantitative analysis
The quantitative analysis of angiogenesis and adipogenesis rates in preclinical models offers clinicians a framework for guiding treatments. With more accurate expectations of the pace of tissue integration—such as the 0.366% weekly increase in angiogenesis and the 3.88% weekly rise in adipogenesis—clinicians can incorporate this knowledge to optimize treatment decisions, such as the volume of hDAM to inject, the frequency of repeat injections, ideal follow-up time points, and selecting which patients would be ideal hDAM candidates and which would benefit from complementary or alternative interventions. Clinicians can also better predict when satisfactory tissue integration can be expected, offering patients a better idea of when outcomes will be noticeable.
Moreover, the variability observed in the rates of angiogenesis and adipogenesis across studies indicated by random effect variances suggest hDAM preparations should be customized depending on the comorbidities and expected baseline tissue regenerative capacity of each patient. For example, patients with a history of smoking, diabetes, renal failure, or other vasculopathies, may benefit from techniques exhibiting higher angiogenic rates, such as low density AAM or precondition with EVE. Quantifying the specific rates of angiogenesis and adipogenesis also supports future research, as these rates provide benchmarks for comparing new hDAM formulations, preparation techniques, and adjunctive therapies.
Translating preclinical findings into clinical practice
By systematically reviewing and analyzing preclinical and clinical data, this review helps clinicians translate the regenerative potential of hDAM into practical therapeutic strategies. Angiogenic and adipogenic trends were consistent across murine studies, which reinforces their clinical relevance. In addition to regenerative ability, clinical studies demonstrate hDAM is effective in achieving desirable patient-reported outcomes and volume retention. Studies report sustained volume retention in both facial and body contouring applications, as well as functional improvements, enhanced tissue quality, and improved skin tone, texture, and overall appearance.
Advantages over traditional volume replacement techniques
Traditional methods for soft tissue augmentation include AFTs and synthetic fillers. While widely used due to its natural results and biocompatibility, AFT is associated with several limitations, including donor site morbidity, unpredictable survival, and the potential for complications such as infection and fat necrosis.36–38 hDAMs have lower resorption rates, thus it is more effective in maintaining their structure and bioactivity over time. In addition, given the preparation technique and cell removal, there is a lower infection risk associated with hDAM. 39
Synthetic fillers have become increasingly popular for soft tissue augmentation in recent years, but some have been shown to cause chronic inflammation-induced fibrosis and contour irregularities. 40 They are also associated with nodule formation, hypersensitivity reactions, migration, and granulomas. 41 Due to the low immunogenicity of hDAM, there is a lower risk of allergic reactions and chronic inflammation. Furthermore, hDAM may integrate better with surrounding tissues and minimize long-term complications associated with synthetic fillers.
Standardizing hDAM preparation
A key finding of this review is the variability in hDAM preparation methods, which complicates direct comparisons between studies. Techniques such as EF decellularization, ultrasonication, and mechanical preconditioning have been shown to differentially affect the rate of adipogenesis and angiogenesis. For example, ultrasonicated hDAM (U-DAM) demonstrated faster and more robust tissue regeneration than homogenized hDAM (H-DAM), with earlier appearance of adipocytes and capillary formation. These findings underscore the need to standardize preparation techniques to ensure consistent clinical outcomes.
Gaps in current research and future directions
Despite promising findings, several gaps remain in the current literature. First, the small number of human studies limits the generalizability of preclinical findings to clinical practice. Long-term data on volume retention, vascularization, and tissue integration are sparse, leaving questions about hDAM’s efficacy over extended periods. Future studies should focus on long-term follow-up to better understand the durability of hDAM in human applications.
Second, variability in outcome measures across studies hinders the ability to perform a comprehensive meta-analysis, limiting the generalization of findings. Standardized outcome measures, particularly for angiogenesis and adipogenesis, should be adopted to facilitate more reliable comparisons between studies. In addition, more randomized clinical trials are needed to provide high-level evidence for hDAM’s efficacy compared with traditional fat grafting and synthetic fillers.
Third, while several studies highlight hDAM’s potential to enhance tissue regeneration, little is known about the impact of specific patient factors, such as age, comorbidities, or genetic background, on hDAM outcomes. Future research should investigate how these variables affect angiogenesis, adipogenesis, and volume retention to better tailor hDAM treatments to individual patient needs. As technology advances, further hDAM modifications, such as injection site preparation, the addition of growth factors, or combination treatments with stem cell or gene therapy, may help patients with specific tissue requirements achieve better outcomes.
Conclusions
This systematic review demonstrates that hDAM is a potent biomaterial for soft tissue reconstruction, significantly promoting angiogenesis and adipogenesis. Clinical studies support its effectiveness in achieving sustained volume retention and patient satisfaction, suggesting hDAM is a viable alternative to traditional volume replacement techniques while offering off-the-shelf availability and high biocompatibility. By providing a quantitative analysis of regenerative rates, this review establishes a data-driven foundation for optimizing clinical protocols and guiding future research on hDAM modifications. As hDAM technology advances, the potential for personalized medicine through customized hDAM preparation and combination therapies will further enhance its utility in reconstructive and aesthetic surgery.
Authors’ Contributions
B.A.M.: Conceptualization, methodology, software, formal analysis, investigation, resources, data curation, writing—original draft, and project administration. A.A.-R.: Conceptualization, methodology, investigation, writing—original draft, and visualization. K.S.F.: Methodology, software, validation, formal analysis, writing—original draft, writing—review and editing, and visualization. N.M.B.-C.: Validation, investigation, resources, writing—original draft, writing—review and editing, and visualization. E.D.D.: Investigation and writing—original draft. E.C.: Conceptualization and methodology. M.L.: Conceptualization and methodology. M.D.R.: Conceptualization and validation. M.J.O.C.: Investigation. K.C.H.: Investigation. A.T.N.: Investigation, writing—original draft, writing—review and editing, and visualization. G.A.O.C.: Investigation. A.U.: Investigation. B.M.C.: Writing—review and editing and visualization. R.D.G.: Conceptualization, methodology, validation, and supervision.
Footnotes
Funding Information
The authors would like to acknowledge the financial support from Northwestern Medicine and Northwestern University-Feinberg School of Medicine, Department of Surgery, Division of Plastic and Reconstructive Surgery. The content is solely the responsibility of the authors and does not necessarily represent the official views of Northwestern Medicine or Northwestern University.
Disclosure Statement
E.C. and M.L. are employees of Musculoskeletal Transplant Foundation (MTF) Biologics. R.D.G. serves as a consultant and member of the Medical Board of Directors for MTF. All other authors have no competing interests to report.