
Abstract
In this study, the authors examined the contributions of physical functioning, acculturation, the Latino cultural value of familismo, and ethnic identity in predicting depressive symptoms in a community sample of Latino older adults. The participants were 98 Latino older adults, age 65 and older, from a moderately sized Midwestern city. Multiple regression analyses indicated that physical functioning, acculturation, familismo, and ethnic identity were significantly related to depressive symptoms. Due to the limited empirical research focused on ethnic identity among older adults, the construct of ethnic identity was closely examined in an effort to extend ethnic identity theory and research specific to Latino older adults. The findings are discussed within the context of ethnic identity theory and implications for research and practice.
The U.S. population of older adults, those aged 65 and older, will account for roughly 20% of the total population by the year 2030 (U.S. Census Bureau, 2010). This rapid population growth is largely due to longer life spans and aging baby boomers. Simultaneously, both the U.S. population and the older adult population are becoming more racially and ethnically diverse. By the year 2050, the U.S. Latino population is expected to double. U.S. Latino older adults, who currently make up the fastest-growing segment of the older adult population and account for 7% of older adults, are projected to become 20% of the older adult population by the year 2050 (U.S. Census Bureau, 2010).
Alarmingly, paired with these unprecedented demographic trends, national reports also indicate an increasing prevalence of physical and mental health disparities among U.S. Latinos (e.g., National Council of La Raza, 2005; Surgeon General, 2001). It is estimated that 85% of Latino older adults have at least one chronic health condition that drastically impairs their quality of life (Applewhite, Garcia Biggs, & Herrera, 2009). There is some evidence that physical illness for Latino adults is strongly associated with depression (e.g., Black, Goodwin, & Markides, 1998; Liang, Xu, Quinones, Bennett, & Ye, 2011), and that there is a higher prevalence of depression among both U.S.-born and immigrant Latino older adults in comparison with African American and White older adults (Areán et al., 2005; González, Haan, & Hinton, 2001; Liang et al., 2011).
Further exacerbating health disparities for Latino older adults is the undertreatment for physical and mental health problems, and the less-than-optimal overall quality of care received when they do seek treatment (Barrio et al., 2008; Sorkin, Pham, & Ngo-Metzger, 2009; U.S. Department of Health and Human Services, 2001). Health services based on Western approaches often lack cultural relevance for Latino older adults seeking treatment, which may be compounded by treatment access issues, language barriers, and low levels of acculturation (Barrio et al., 2008; Chavez-Korell et al., 2012; González et al., 2001; Santiago-Rivera, Arredondo, & Gallardo-Cooper, 2002). In an effort to develop preventive and therapeutic interventions for Latino older adults, scholars have increasingly stressed the importance of incorporating Latino older adults’ social resources (e.g., family, extended kinship networks, and religious/spiritual communities) and cultural resources (e.g., ethnic identity, cultural values, spirituality, and language) into mental health treatment (Beyene, Becker, & Mayen, 2002; Chavez-Korell et al., 2012; Cruza-Guet, Spokane, Caskie, Brown, & Szapocznik, 2008; Santiago-Rivera et al., 2002); however, empirical research examining such resources remains scant. Little research exists about the nature of the relationships between physical health, psychosocial–cultural factors, and mental health for Latino older adults. Therefore, the purpose of the present study was to examine potential psychosocial–cultural resources (i.e., familismo, ethnic identity, and acculturation) in relation to physical health and depressive symptoms for a community sample of Latino older adults.
Latino Older Adults and Depression
Depression is the most frequently diagnosed mental health concern for older adults in the United States, where an estimated 5.7% of older adults suffer from major depression and an additional 15% to 20% suffers from less severe minor depressive disorders (Cahoon, 2012; Substance Abuse and Mental Health Services Administration [SAMSHA], 2007). The prevalence of depression is higher for both U.S.-born and immigrant Latino older adults, in comparison with other racial and ethnic older adults, with prevalence estimates of 20% to 30% (Areán et al., 2005; Chavez-Korell et al., 2012; Falcon & Tucker, 2000; González et al., 2001). There are strong links between all forms of depression with comorbid psychiatric and medical conditions for older adults (Badger, 2001; Cahoon, 2012; Nyunt, Lim, Yap, & Ng, 2012). Specific to Latino older adults, there is some evidence that depression is strongly associated with poor physical health (Black et al., 1998; Kemp, Staples, & Lopez-Aqueres, 1987; Liang et al., 2011; Sorkin et al., 2009). In a study involving Latino older adults in Los Angeles, Kemp et al. (1987) discovered that 26% had a depressive disorder and that the depression was related to medical conditions in 94.5% of these cases.
Acculturation and Latino Mental Health
In a review of the empirical literature focused on Latino mental health and acculturation, Lara, Gamboa, Kahramanian, Morales, and Bautista (2005) concluded that more negative than positive mental health outcomes were associated with acculturation for Latinos. However, inconsistent findings exist within the empirical literature. Studies examining the association between acculturation and the risk of depression in Latinos have utilized differing definitions and measures of acculturation and have had conflicting results. Black et al. (1998) reported that immigrant women were at significantly greater risk for depression in comparison with U.S.-born Latinos, whereas being an immigrant male imparted a protective effect. Krause and Goldenhar (1992) examined English language use as a measure of acculturation and found that Latino older adults who used more English were at lower risk for depression. Results from the Hispanic Health and Nutrition Examination Survey (Moscicki, Locke, Rae, & Boyd, 1989) reported opposite findings, in which less-acculturated, immigrant Mexican Americans were at a reduced risk of depression (this was a combined sample of younger and older adults). In addition, changes in lifestyle associated with acculturation have been related to increases in the risk of obesity (Arandia, Nalty, Sharkey, & Dean, 2012), diabetes (Barrera, Toobert, Strycker, & Osuna, 2012), and cardiovascular disease (Gallagher et al., 2012), and as mentioned in the previous section on depression, physical health problems have been found to have strong associations with depressive symptoms for Latino older adults.
Acculturation to mainstream U.S. culture is an important aspect of the psychosocial experience of many Latinos. The demands to adjust to different customs and social norms, learn a new language, and become familiar with new laws and rules can create considerable stress and strain (Organista, Organista, & Kurasaki, 2003). The sociopolitical environment along with the context of the reception by the host country influences the acculturation experience. Other factors that may influence the acculturation experience include socioeconomic status, family and social supports, employment, gender, age, and time in the United States and country of origin. Although inconsistencies remain in the risk estimates of depression for acculturation among Latino older adults, it is evident that the process of acculturation influences the mental health of Latinos; therefore, this complex relationship requires further investigation specific to Latino older adults considering the prevalence of depression and low-acculturation rates for this population.
Familismo
The Latino cultural value of familismo (family orientation and connectedness) has been found to have a positive impact on the psychological and physical health of Latinos (Austin & Smith, 2008; Castillo, Conoley, & Brossart, 2004; Coohey, 2001; Gil, Wagner, & Vega, 2000). Familismo refers to having strong feelings of reciprocity, loyalty, and solidarity among family members (Santiago-Rivera et al., 2002). This Latino value originates from a collectivistic worldview in which there is willingness to sacrifice for the well-being of the group (Marín & Triandis, 1985). Studies have confirmed that familismo contributes to positive mental health for Latinos (e.g., Ayón, Marsiglia, & Bermudez-Parsai, 2010; Gil et al., 2000; Harker, 2001; Unger et al., 2002) by providing a natural support system that promotes growth and protects family members from emotional stressors (Cruza-Guet et al., 2008). The perceived support from family members has been found to be an important aspect of familismo that is not affected by acculturation levels in Latino adults (Comeau, 2012; Sabogal, Marín, Otero-Sabogal, Marín, & Perez-Stable, 1987). Latino adults endorse higher values of family support and obligations to family members in comparison with individuals of European American descent (Comeau, 2012). Furthermore, Latinos are more likely than non-Latino Whites to live near their families, where family serves as the primary social unit, and attribute additional importance to more personal types of communication such as face-to-face contact interactions, especially with family members (Santiago-Rivera et al., 2002). In addition, familismo has been linked to help-seeking behaviors; specifically, familismo tends to promote seeking help from within the family rather than from outsiders and may influence whether Latinos seek psychotherapy services provided within a Eurocentric context (Alegría et al., 2007; Areán et al., 2005).
Although there is relatively strong evidence for the positive effects of familismo on younger Latinos, there is little research that has examined these effects among Latino older adults. Descriptively, we know that Latino older adults are more likely to live with and be financially dependent on their adult children, and less likely to rely on hospices and nursing homes in comparison with non-Latino White older adults (Colon & Lyke, 2003; Hispanics in Philanthropy, 2011). Cruza-Guet and colleagues (2008) examined the relationship between social supports and psychological distress among Latino older adults (predominately Cuban) in Miami, Florida, and found that satisfaction with received social support was associated with lower psychological distress. Guided by the existing literature, in the current study, we examined the relationship between the Latino cultural value of familismo and depressive symptoms for Latino older adults.
Latino Older Adults and Ethnic Identity
Little is known about ethnic identity and the role it serves in the day-to-day lives of older adults, and even less is known about ethnic identity specific to Latino older adults. Theoretical conceptualizations of ethnic identity (Phinney, 1989; Umaña-Taylor, Yazedjian, & Bámaca-Gómez, 2004), the degree to which individuals perceive themselves as being a part of and aligned with an ethnic group, include tenets of social identity theory (Tajfel & Turner, 1986) and the ego identity development literature (Erikson, 1968; Marcia, 1980). Identity theorists have emphasized the idea that individuals’ attitudes regarding their ethnicity unfold systematically as part of a normative lifelong process of psychological development (Cross & Fhagen-Smith, 2001; Erikson, 1968; Marcia, 2002).
Recent work has indicated that ethnic identity can be conceptualized as involving exploration, resolution/commitment, and affirmation (Phinney & Ong, 2007; Umaña-Taylor et al., 2004). Exploration refers to the process by which an individual searches and increases his or her knowledge about his or her ethnic group. Resolution entails making a commitment or developing a sense of understanding regarding the role ethnic group membership plays in the individual’s life. Affirmation is defined as positive or negative feelings about one’s ethnic group membership and is considered an affective component of ethnic identity. Umaña-Taylor and colleagues (2004) developed a typology that integrates these three aspects of ethnic identity with the identity statuses developed by Marcia (1980) of diffusion, foreclosure, moratorium, and achievement. Diffusion describes individuals who have neither explored nor resolved their identity. Foreclosure involves low exploration but high resolution or commitment while moratorium entails high exploration but low commitment. Achievement includes individuals who have explored and resolved their identity.
Although identity development was originally conceptualized to occur during adolescence (Marcia, 1966), a growing number of identity researchers have expanded the model to include adulthood (Marcia, 2002; Meeus, Iedemaa, Helsen, & Vollebergh, 1999; Yip, Seaton, & Sellers, 2006). Yip and colleagues (2006) found evidence for the existence of four ethnic identity statuses (i.e., achieved, foreclosed, moratorium, and diffused) across three different age groups of African Americans (i.e., adolescents, college students, and adults), with older participants disproportionately occupying the achieved status but older adults were also represented in the other statuses (e.g., diffused).
The process of ethnic identity has extended into adulthood with theorists indicating that individuals reexamine their ethnic identity throughout their lives particularly when faced with new and changing contexts (Parham, 1989; Phinney, 2006). Given the developmental conceptualization of ethnic identity, a bulk of empirical literature has focused on adolescent samples with less work examining adults and older adults let alone Latino older adults. Guided by ethnic identity theory, one can make predictions about ethnic identity across the life span. Given the fact that adults who have not committed to an identity in adolescence can choose to explore what their ethnic group identity means to them and that adults may reevaluate their ethnic identity as triggered by life events, we expect that the three components of ethnic identity development (i.e., affirmation, resolution, and exploration) are likely to be represented throughout the life cycle.
In a meta-analysis conducted by Smith and Silva (2011), a modest relationship between ethnic identity and personal well-being was found, with stronger relationships found among adolescents and young adults, than adults above 40. However, relatively few studies have examined ethnic identity among adults above 40 years of age, and specifically with older adults age 65 and older (Smith & Silva, 2011; Yip et al., 2006). No studies, to our knowledge, have examined ethnic identity among Latino older adults or its relationship to psychological well-being for Latino older adults.
The Present Study
The goals of this study were threefold: (a) to examine the relationship between physical and mental health for Latino older adults, (b) to examine ethnic identity among Latino older adults, and (c) to examine the relationships between psychosocial–cultural factors (i.e., acculturation, familismo, and ethnic identity) and the depressive symptoms of Latino older adults. In this study, we examined four hypotheses. First, in keeping with previous research, we expected that physical functioning would be negatively associated with depressive symptoms among Latino older adults. Second, we hypothesized that acculturation would be positively and significantly associated with depressive symptoms. Third, we expected familismo to be negatively associated with depressive symptoms. Finally, we hypothesized that ethnic identity would significantly contribute to the variance in depressive symptoms for Latino older adults. Specifically, in keeping with the limited findings from previous research examining ethnic identity among African American older adults (Yip et al., 2006), we hypothesized that affirmation, exploration, and resolution would be significantly and negatively associated with depressive symptoms for Latino older adults.
Method
Participants and Procedures
Participants were 98 older adults living in a metropolitan area in the Midwest region of the United States, who self-identified as being Latino or Hispanic (32 men and 66 women). Participants ranged in age from 65 to 97 years (M = 71.04 years, SD = 7.80). Participants identified their ethnic background as Mexican (n = 39; 39.8%), Puerto Rican (n = 28; 28.6%), Cuban (n = 4), South American (n = 10), Hispanic/Latino (n = 9), Other (n = 5), and 3 participants did not respond. In addition, 61.4% (n = 59) of participants were not born in the United States, with years in the United States ranging from 1 to 81 years (M = 37.03 years, SD = 21.52). In regard to participants’ education, 11.2% (n = 11) reported they did not attend school, 22.4% (n = 22) had an elementary school education, 26.5% (n = 26) completed middle school, 21.4% (n = 21) graduated from high school, 14.3% (n = 14) attended college, and 4 participants did not respond.
These data represent a community sample of participants. Approximately half of the participants (55.10%; n = 54) were recruited at a large Latino community center where there are older adult day programs, housing for older adults, and social events for the extended Latino community. The other 44 participants were recruited through face-to-face recruiting at local community festivals and churches. All measures were made available to participants in English and Spanish. Given the choice, the large majority of participants (91.84%) chose to respond in Spanish to the study measures. Bilingual Latino research team members read aloud each of the measures to participants in one-on-one interviews.
Measures
In addition to demographic items, participants completed five measures: the Ethnic Identity Scale (EIS; Umaña-Taylor et al., 2004), the Short Acculturation Scale for Hispanics (SASH; Marín, Sabogal, Marín, Otero-Sabogal, & Perez-Stable, 1987), the Pan-Hispanic Familism Scale (Villarreal, Blozis, & Widaman, 2005), the 9-Item Patient Health Questionnaire (PHQ-9; Kroenke & Spitzer, 2002), and the Short Form-12 Health Survey (SF-12; Ware, Kosinski, & Keller, 1996). Measurement selection was based on the brevity and ease of administration in an effort to place minimal burden on the older adult population, as well as the established reliability and validity of the measure for use with Latinos, Spanish-speakers, and/or older adults. All measures were counterbalanced to control for order effects.
Ethnic Identity
Participants’ ethnic identity was assessed by the EIS (Umaña-Taylor et al., 2004), a 17-item instrument that measures three distinct components of ethnic identity formation. The three EIS subscales are Exploration (7 items), Resolution (4 items), and Affirmation (6 items). Responses to EIS items are made on a 4-point Likert-type scale, ranging from 1 (does not describe me at all) to 4 (describes me very well). Sample items are “I have participated in activities that have exposed me to my ethnicity” (Exploration item), “I am clear about what my ethnicity means to me” (Resolution item), and “My feelings about my ethnicity are mostly negative” (Affirmation item; reverse coded). Subscale scores are obtained by reverse coding indicated items and summing items that make up each subscale. High subscale scores indicate high levels of exploration, resolution, and affirmation. Subscale reliability estimates for the EIS scores have ranged from .84 to .89 with ethnically diverse samples (Umaña-Taylor et al., 2004), and from .80 to .88 in a sample of Latino adults (Chavez-Korell & Torres, 2014). In the current study, the Cronbach’s alpha coefficients for the subscale scores were .80 (Affirmation), .81 (Exploration), and .82 (Resolution).
Acculturation
The SASH (Marín et al., 1987), a 12-item unidimensional measure of acculturation, was used to assess the degree of endorsement of mainstream U.S. American culture. Responses to SASH items are made on a 5-point scale, ranging from 1 (only Spanish; all Hispanics/Latinos) to 5 (only English; all Americans). Sample items are “What language do you usually speak with your friends?” and “Your close friends are . . . ” Total scores range from 12 to 60, with low scores indicating low preference for mainstream U.S. American culture and high scores indicating high preference for mainstream U.S. American culture. The SASH has been found to have strong validity and reliability indexes in previous studies (Marín et al., 1987). In this study, the coefficient alpha was .96.
Familismo
Participants’ attitudes about the value and importance of family were assessed with the Pan-Hispanic Familism Scale (Villarreal et al., 2005), a 5-item instrument. Responses to items are made on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (strongly agree). A sample item is “My family is always there for me in times of need.” Scale scores are obtained by summing and averaging responses across the 5 items with higher scores indicating a greater endorsement of familismo. A one-factor confirmatory factor analysis demonstrated scale validity (Villarreal et al., 2005). Previous studies resulted in Cronbach’s coefficient alphas of .95 with Latino male college students (Ojeda, Navarro, & Morales, 2011) and .82 with Latino adults (Villarreal et al., 2005). The Cronbach’s alpha for the current study was .90.
Depressive Symptoms
The PHQ-9 (Kroenke & Spitzer, 2002) was used to measure participants’ depressive symptoms, with each item corresponding to one of the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for depression. A sample item is “Over the last 2 weeks, how often have you been bothered by poor appetite or overeating?” Items are rated on a 4-point Likert-type scale, ranging from 0 (not at all) to 3 (nearly every day). Total scores range from 0 to 27, with lower scores representing lower severity, a score of 10 to 14 representing minor depressive symptoms, 15 to 19 moderately severe, and greater than 20 indicating severe major depressive symptoms.
The PHQ-9 has been well-validated for older adults and for Spanish-speaking communities (e.g., Gilbody, Richards, Brealey, & Hewitt, 2006). Kroenke and Spitzer (2002) found strong support for criterion validity against independent structured interviews by mental health professionals. The validity of the PHQ-9 is sufficiently well established, and it is now being used in published studies as a criterion against which other measures of depression are examined (Ani et al., 2008). The PHQ-9 has been used successfully in studies of older adults, including older adults with comorbid medical conditions who are receiving treatment for depression, Latino older adults with comorbid medical conditions, community-based samples of older adults, and community-based samples of Latino older adults (Chavez-Korell et al., 2012). The Cronbach’s alpha for the current study was .90.
Physical Functioning
Physical functioning was measured by the Physical Component Summary Score of the SF-12 (Ware et al., 1996). SF-12 scores range from 30 (worst physical functioning) to 70 (best physical functioning), with a score of 50 being the U.S. average score normed for older adult populations.
The SF-12 is a shortened form of the SF-36, which measures eight domains of health. According to Ware et al. (1996), the SF-12 was developed after it was discovered that 85% of the variance measured by the SF-36 was attributable to two of the eight scales, the Physical Component Summary and the Mental Component Summary. It was further found that 12 items accounted for more than 90% of the variance captured by these two scales. The SF-12 asks respondents to rate the extent to which their physical and emotional health has, over the past 4 weeks, limited them globally and with regard to specific activities. Studies comparing the SF-12 with the well-validated SF-36 have supported its internal consistency (Luo et al., 2003), test–retest reliability (Ware et al., 1996), construct and criterion validity (Gandek et al., 1998; Jenkinson & Layte, 1997; Ware et al., 1996), and discriminant validity (Sugar et al., 1998; Ware et al., 1996). In addition, support for the psychometric properties of the Spanish version of the SF-12 has also been found (e.g., Jordan-Marsh, Cody, Silverstein, Chin, & Garcia, 2008; Peek, Ray, Patel, Stoebner-May, & Ottenbacher, 2004). In addition, the Spanish version of the SF-12 has been used successfully in studies of populations similar to the current study’s population of focus, including studies with Latino older adults (e.g., Chavez-Korell et al., 2012), Latinos seeking treatment for depression, and community-based samples of Latinos (Guerra & Shea, 2007). In the current study, the coefficient alpha was .94.
Results
A power analysis was conducted to calculate the sample size using G*Power 3.0 (Erdfelder, Faul, & Buchner, 1996). Power was set at f2 = 0.80, and the alpha level was set at .05. Results of the analysis, accounting for six predictor variables, suggested that a sample size of 97 participants was needed to detect a medium effect (i.e., 0.15) and a sample of 46 participants was needed to detect a large effect (i.e., 0.35). Therefore, according to the power analysis, the present study (N = 98) had a high likelihood of detecting medium and large main effects.
Preliminary Analyses
Means, standard deviations, and correlation coefficients were calculated for the scores on the SF-12 Physical Component Summary Score, the SASH, Familismo scale, the three EIS subscales, and the PHQ-9 and are presented in Table 1. The results indicated that physical functioning was significantly associated with ethnic identity exploration (r = .34; p < .01) and negatively associated with depressive symptoms (r = –.45; p < .01). Acculturation, preference for mainstream U.S. American culture, was significantly correlated with depressive symptoms (r = .29; p < .01). Familismo was negatively associated with depressive symptoms (r = –.24; p < .05). Two of the EIS subscales, Resolution (r = –.20; p < .05) and Affirmation (r = –.20; p < .05), were negatively associated with depressive symptoms.
Means, Standard Deviations, and Correlations Among Variables (N = 98).
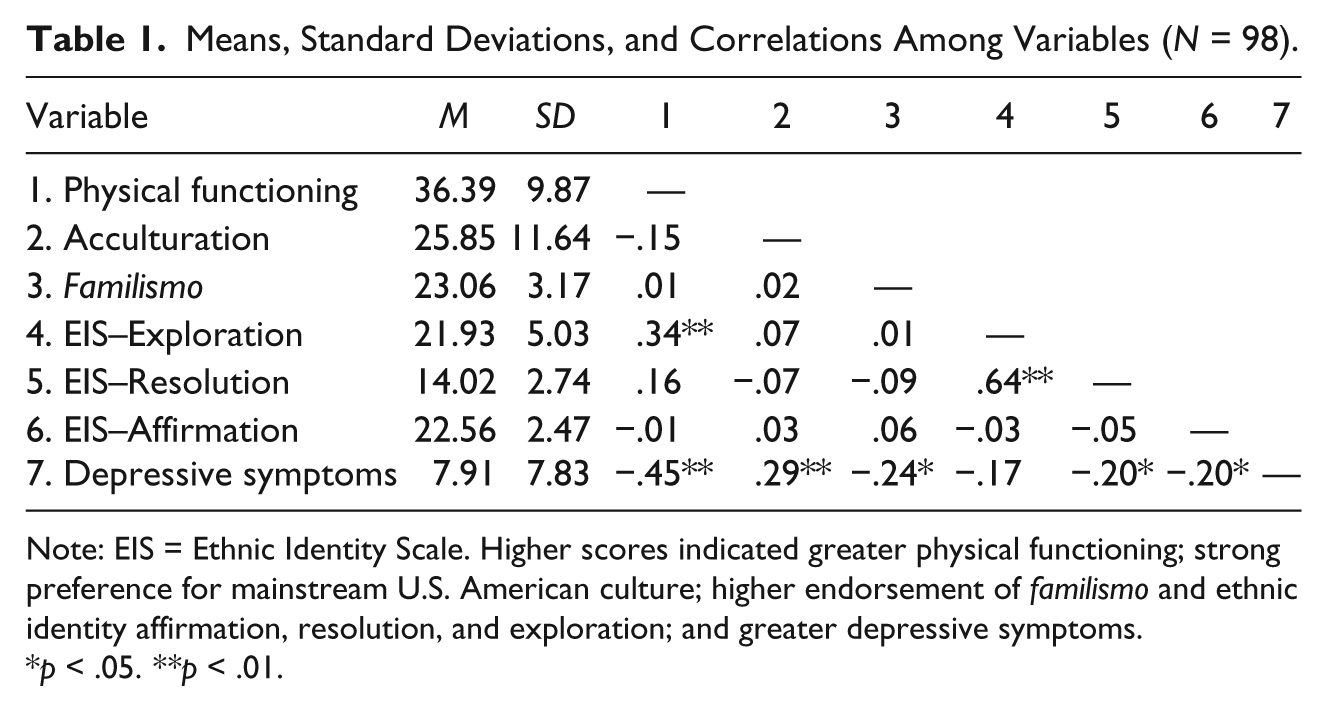
Note: EIS = Ethnic Identity Scale. Higher scores indicated greater physical functioning; strong preference for mainstream U.S. American culture; higher endorsement of familismo and ethnic identity affirmation, resolution, and exploration; and greater depressive symptoms.
p < .05. **p < .01.
Five analyses of variance between groups (ANOVAs) were conducted to test whether depressive symptoms varied as a function of participants’ sex, ethnic identification, education, whether they were born in the United States, and years in the United States. The results indicated that there were no significant main effects for any of these demographic factors; thus, none were used as covariates in the subsequent regression analysis.
Primary Analyses
To investigate the relationship between psychosocial–cultural factors (i.e., acculturation, familismo, and ethnic identity) and depressive symptoms for Latino older adults, a forced entry multiple regression was conducted. This methodology was chosen to determine whether the psychosocial–cultural variables were significantly related to depressive symptoms after controlling for the effects of physical functioning, which was found to be significantly related to depressive symptoms for Latino older adults. This multiple regression method relies on good theoretical reasoning for including the selected predictors; however, there are no decisions about the order in which variables are entered. This was also an appropriate analysis for the sample size (N = 98).
With PHQ-9 scores as the dependent variable, the multiple regression indicated that after the first step, physical functioning generated R2 = .20, F(1, 96) = 24.56, p = .000 (adjusted R2 = .20). At the second step of the regression, with the addition of the psychosocial–cultural variables, acculturation, familismo, ethnic identity exploration, ethnic identity resolution, and ethnic identity affirmation, R2 = .37, F(5, 91) = 8.92, p = .001 (adjusted R2 = .33; ΔR2 = .17).
Analysis of the specific predictor variables revealed significant patterns. In support of our hypotheses, physical functioning (β = –.41, p = .000), familismo (β = –.24, p = .005), ethnic identity resolution (β = –.19, p = .05), and ethnic identity affirmation (β = –.20, p = .01) were significantly related to lower levels of depressive symptoms. Also in support of our hypothesis, acculturation (preference for mainstream U.S. American culture) was significantly and positively related (β = .22, p = .01) to depressive symptoms. Contrary to our hypothesis, ethnic identity exploration (β = .06, p = .60) was not significantly related to depressive symptom levels. Table 2 provides information on predictors of depressive symptoms.
Multiple Regression of Predictors of Depressive Symptoms Among Latino Older Adults (N = 98).
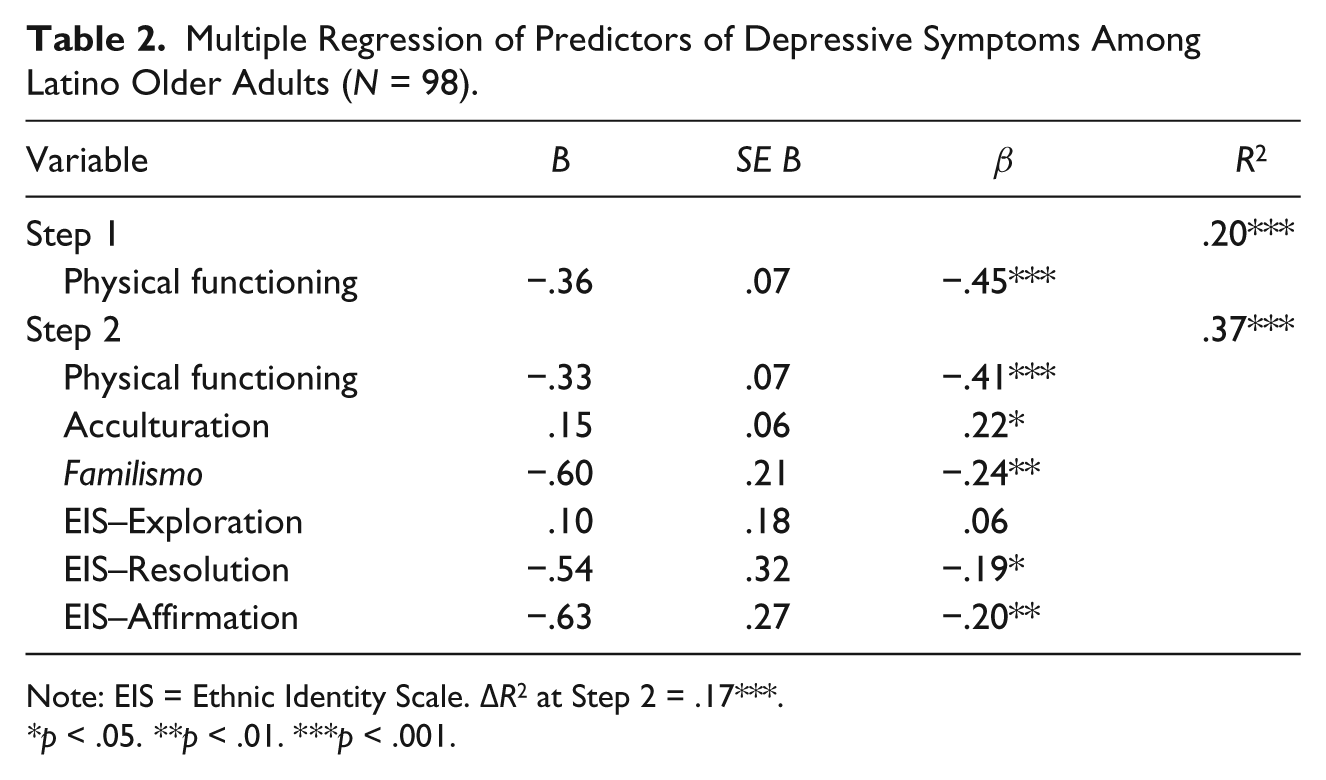
Note: EIS = Ethnic Identity Scale. ΔR2 at Step 2 = .17***.
p < .05. **p < .01. ***p < .001.
Discussion
The purpose of this study was threefold: (a) to examine the relationship between physical and mental health for Latino older adults, (b) to examine ethnic identity among Latino older adults, and (c) to examine the relationships between psychosocial–cultural factors (i.e., acculturation, familismo, and ethnic identity) on the depressive symptoms of Latino older adults.
Latino Older Adults and Ethnic Identity
To our knowledge, there is no empirical literature that explicitly examines ethnic identity among Latino older adults. Using descriptive statistics and multiple regression analyses to examine levels of ethnic identity affirmation, exploration, and resolution, this study provides evidence that the three components of ethnic identity development are represented in the lives of Latino older adults. Through the examination of mean scores, range of scores, and standard deviations, it is clear that Latino older adults endorse the three components of ethnic identity to varying degrees. The mean scores across the three ethnic identity subscales were high in this sample of Latino older adults, indicating that older adults tend to strongly endorse ethnic group affirmation, exploration, and resolution. However, the range of scores for each subscale and the standard deviations also offer evidence that ethnic identity is in fact experienced differently across individuals, with some older adults holding negative feelings about their Latino ethnic group membership, having limited ethnic group exploration, and feeling uncertain about what their ethnic group membership means for them. These findings provide support for ethnic identity development theory, which emphasizes that individuals’ attitudes regarding their ethnicity unfolds systematically as part of a normative lifelong process of psychological development (Cross & Fhagen-Smith, 2001; Erikson, 1968; Marcia, 2002; Phinney, 2006) and suggests that identity development is not necessarily completed or resolved during adolescents but instead may continue to develop or be revisited into adulthood and older adulthood (Cross & Fhagen-Smith, 2001; Parham, 1989; Phinney, 2006; Yip et al., 2006).
In addition, the results of multiple regression analyses provide preliminary evidence that the three components of ethnic identity development are not only present among Latino older adults, but ethnic identity also relates to the psychological well-being of older adults. In this study, ethnic identity affirmation and ethnic identity resolution were significantly related to lower depressive symptoms. Because there has been limited focus on the ethnic identity of older adults, ethnic identity researchers and theorists have questioned whether ethnic identity serves any significant role in the lives of older adults (Cross & Cross, 2008; Yip et al., 2006). This study begins to establish that not only is ethnic identity salient in the lives of older adults but that it may serve an important role in the day-to-day functioning and quality of life for Latino older adults.
Psychosocial–Cultural Predictors of Depressive Symptoms
The current study suggests that physical functioning and the psychosocial–cultural variables of acculturation, familismo, and ethnic identity, are related to depressive symptoms among Latino older adults. Latino older adults who reported lower levels of physical functioning had significantly higher levels of depressive symptoms. This relationship between physical functioning and depression has been well established in previous research with older adults (e.g., Badger, 2001; Cahoon, 2012; Nyunt et al., 2012); the present study affirmed these same phenomena for Latino older adults.
After controlling for the effects of physical functioning, the psychosocial–cultural variables of acculturation, familismo, and ethnic identity independently emerged as significantly contributing to the variance in depressive symptoms. Consistent with our hypothesis, acculturation (preference for mainstream U.S. American culture) significantly contributed to depressive symptoms. This finding provides further support for the literature suggesting that more negative than positive mental health outcomes were associated with acculturation for Latinos (Alegría et al., 2007; Lara et al., 2005). One possible explanation for this finding may be due to context. All of the data for this study were collected within an area of the city known by many as the “Latino south side,” in a racially segregated Midwestern city. Previous research by Kwag, Jang, and Chiriboga (2012) found that the impact of acculturation on depressive symptoms for Latino older adults was moderated by the perceived density of Latinos in neighborhoods. Latino older adults in this study reported low levels of acculturation and live in an ethnically dense Latino area where businesses are largely Latino-owned and oriented toward Latino consumers; Spanish is spoken everywhere; and the residents of the zip code area are more than 85% Latino; therefore, context may be influencing the relationship between acculturation and depression.
The Latino cultural value of familismo was found to be negatively related to depressive symptoms for Latino older adults. This finding has been well established in the literature (e.g., Ayón et al., 2010; Cruza-Guet et al., 2008; Gil et al., 2000; Harker, 2001; Unger et al., 2002). The present study affirmed the same phenomenon that family social support can serve as a buffer for psychological distress for Latino older adults.
In addition, ethnic identity affirmation and resolution were significantly related to depressive symptoms for Latino older adults. Affirmation is the affective component of ethnic identity and refers to feelings about one’s ethnic group membership. Resolution entails making a commitment or developing a sense of understanding regarding the role ethnic group membership plays in the individual’s life. Latino older adults with strong positive feelings about being Latino (affirmation) had lower levels of depressive symptoms. Similarly, Latino older adults who knew what their Latino ethnic identity meant to them and who were committed to their Latino ethnic identity (resolution) also had significantly lower levels of depressive symptoms. These findings are consistent with the hypotheses and research indicating a modest relationship between ethnic identity and psychological well-being (Smith & Silva, 2011).
Ethnic identity exploration was the only component of ethnic identity that did not significantly contribute to the variance in depressive symptoms. Interestingly, bivariate correlations identified a statistically significant positive relationship between ethnic identity exploration and physical functioning for Latino older adults, possibly due to the need for mobility and physical activity in exploring one’s ethnic cultural heritage and engaging in cultural events; however, exploration was not related to depressive symptoms.
Limitations
There are important factors that limit the conclusions that can be drawn from this study. The generalizability of the findings is limited, as the sample of participants were not randomly selected and was composed of a community sample of Latino older adults from a Midwestern city in the United States. This sample may not be reflective of Latino older adults living in rural settings or other geographic regions of the United States. In addition, this sample had more women than men, and the participants’ Latino heritage was predominately Mexican and Puerto Rican. This sample may not be reflective of other Latino heritage groups (e.g., Cuban, South American, and Dominican). Sample size is another limitation, as the small sample size inhibited the use of more robust statistical designs (i.e., cluster analyses of ethnic identity subscales to examine ethnic identity statuses).
Clinical Implications and Future Directions
The findings obtained in this study are a first step in examining ethnic identity among Latino older adults, and the role physical functioning, ethnic identity, familismo, and acculturation may play in the psychological well-being of Latino older adults. These results have potentially important clinical implications for counseling psychologists and other mental health professionals. Knowing that a Latino older adults’ ethnic identity may be salient in his or her life, and that ethnic identity also has the potential to influence depressive symptoms, clinicians should consider ways to intentionally and meaningfully adapt mental health interventions to the clients’ culture, worldview, and value system when this is important for the client (e.g., indicated by ethnic identity salience, low acculturation, etc.). Considering that culture plays an important role in the treatment process and is associated with the effectiveness of treatment (Bernal & Scharrón-Del-Río, 2001; Sue, Zane, Nagayama Hall, & Berger, 2009), mental health professionals must provide effective interventions by intentionally accounting for the cultural contexts and cultural values relevant to clients’ well-being (Trimble & Fisher, 2006). In this study, the Latino cultural value of familismo was found to be significantly related to lower depressive symptoms for Latino older adults; therefore, clinicians should consider ways to welcome Latino families into mental health centers, where they can comfortably wait and be of support to their loved one. Counseling psychologists should consider whether family counseling may be more appropriate for the client’s presenting concerns, and also consider how family could be incorporated into the treatment intervention (e.g., behavioral activation activities may involve doing enjoyable activities with family members). A meta-analysis by Griner and Smith (2006) suggested that clients with the greatest need for treatment accommodations (i.e., non-English speakers, older adults, Latinos) received the greatest benefit from culturally adapted mental health interventions.
Alternatively, this study also found that negative feelings about one’s Latino ethnic group (low affirmation), and limited understanding and commitment to one’s Latino ethnic identity (low resolution), were significantly related to higher depressive symptoms for Latino older adults. Counseling psychologists, guided by ethnic identity development theory and research, could use information about a client’s ethnic identity salience (the degree of importance) and valence (whether affect is positive or negative) to inform clinical practice. For example, a depressed Latino older adult client with low affirmation and low resolution may benefit from exploring his or her negative feelings about his or her Latino ethnicity, as there may be psychological benefits to a change in affect as suggested in this study and in ethnic identity development theory (Cross & Cross, 2008; Umaña-Taylor et al., 2004).
Finally, the underutilization of mental health services by Latino older adults is well documented (e.g., Barrio et al., 2008; Sorkin et al., 2009; U.S. Department of Health and Human Services, 2001), and as found in the current study, there is growing support for the relationship between poor physical health and depression for Latino older adults (Black et al., 1998; Kemp et al., 1987; Liang et al., 2011; Sorkin et al., 2009). In an effort to reduce barriers and improve access to mental health care, mental health professionals should consider providing mental health services in alternative settings beyond mental health clinics such as primary care clinics and community centers that have the potential to integrate physical health care with mental health care and mitigate stigma and mistrust (Areán et al., 2005; Karel, Gatz, & Smyer, 2012).
The results of this study contribute to the growing body of research on ethnic identity among Latinos and its relation to psychological aspects of functioning. However, future replication of this study is necessary to provide support for the existence of ethnic identity salience among Latino older adults, and its influence on psychological functioning. Future research should incorporate developmental designs that continue into older adulthood, with larger sample sizes to allow for more robust analyses, so that ethnic identity development and statuses can be examined from early adulthood to older adulthood. In addition, research should also begin to examine how clinicians’ intentional incorporation of cultural adaptations to treatment based on clients’ ethnic identity influence case conceptualization, intervention, and treatment outcomes for older adult Latino clients.
Footnotes
Acknowledgements
The authors extend their gratitude to the participants, the United Community Center, and the first author’s research team for their involvement and generous support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Institute on Race and Ethnicity, University of Wisconsin System.