
Abstract
This article reports on a program of research that examined the background, planning, implementation, and evaluation of an after-school preventive intervention program within an ongoing urban alternative education program targeting African American students referred to the school because of their problematic behavior in regular schools. The research undertaken involved the examination of three separate, but interrelated, investigative components: (a) the relationship of risk and protective factors to the sexual activity of individuals in the targeted population; (b) the problems associated with the implementation of an after-school preventive intervention found to be effective within a regular school setting; and (c) determination of the effectiveness of the after-school preventive intervention, the results of which were largely compromised by the problems encountered during the implementation of the intervention.
While advances have been made in the development of effective school-based prevention strategies for adolescents, further research is needed to provide effective prevention programming for urban minority youth who have already exhibited problem behaviors. Adolescents attending alternative education programs have multiple unmet needs and are at especially high risk for school failure, school dropout, drug use and trafficking, risky sexual activity, and other serious problematic behaviors (Grunbaum et al., 2002; Lehr, Moreau, Lange, & Lanners, 2004). Limited empirical research is available regarding the behavioral characteristics of youth who attend these types of schools, as well as on the risk and protective factors that impact on their involvement in health-compromising behaviors. Initially prompted by these circumstances, the following is a report on a program of research that examined the implementation and evaluation of an after-school preventive intervention program within an ongoing urban alternative education program targeting African American students referred to the school because of their problematic behavior within the regular school system. The research undertaken involved the examination of three separate, but related, investigative components: (a) the relationship of risk and protective factors to the sexual activity of individuals in the targeted population; (b) the implementation process of an after-school preventative intervention found to be effective within a regular school setting; and (c) the effectiveness of the after-school preventive intervention in terms of risk and protection in four behavioral domains of influence.
Background
Alternative Education Programs (AEPs)
Emerging in the United States in the 1960s, AEPs initially grew out of a desire to meet the needs of poor and minority students underserved in traditional public school systems and to create innovative educational programming for suburban students (Meyers, 2001; Raywid, 1999). Recently, however, AEPs have become a frequently used resource for the education and socialization of at-risk youth experiencing academic, behavioral, social, and/or emotional problems. According to Raywid’s (1999) commonly cited typology, AEPs can generally be classified as one of the following three types and/or as containing elements of all three: Type I programs are attended by individual choice and offer innovative, nonstandard curricula; Type II programs mandate attendance in an attempt to segregate and reform disruptive students; and Type III programs may be either attended by choice or mandated and provide therapeutic and remedial educational services to students with social and emotional problems. Although AEPs continue to grow in scope and size throughout the United States, with approximately 11,000 currently in existence serving over 600,000 students, limited empirical findings are available regarding the effectiveness of these programs on the types of students who attend them (Aron, 2006; Barr & Parrett, 2001; Foley & Pang, 2006; Hosley, 2003; Powell, 2003; Wraight, 2010; Zweig, 2003).
Although limited research has been conducted on students who attend AEPs, available information indicates that the majority of these youth are poor, bilingual, and/or a member of a minority population (Carswell, Hanlon, O’Grady, Watts, & Pothong, 2009; Foley & Pang, 2006; Lehr et al., 2004; Powell, 2003). Nationwide data obtained from the Youth Risk Behavior Surveillance (Grunbaum, Lowry, & Kann, 2001) revealed that, compared to regular high school students, AEP high school students were older, on average; likely to be disproportionately Hispanic and/or African American; and more likely to have smoked cigarettes, drunk alcohol, and/or used marijuana or cocaine. They were also more likely to have engaged in sexual intercourse and be sexually active. Specifically designed to address such characteristics in an African American youth population, the present application of a prevention-focused after-school program in an urban Type II alternative education program provided an opportunity not only to obtain treatment-relevant information on youth who are likely to be included in such programs, but also to highlight programmatic issues having a direct bearing on the planning and evaluation of future prevention efforts undertaken in similar settings.
The Overall Research Undertaken
African American students entering a single alternative education program conducted at two urban middle-school sites within the same metropolitan area were recruited for participation in a research program conducted at the AEP over consecutive years of a 4-year project intake period. In implementing recruitment procedures, research staff made contact with those parents/guardians and AEP students who, in reply to a notice of the availability of the investigative program, demonstrated an interest in participating. All aspects of the proposed research, including a description of the after-school preventive intervention component, were fully explained to caregivers and to the child. Once all questions had been satisfactorily answered and research program recruitment and processes had been agreed upon, parents/guardians and students signed informed consent and assent forms, respectively.
Assessment battery
The research program’s baseline assessment battery included self-report data and school information to assess characteristics, circumstances, and experiences that had been previously found to be related to the involvement of youth in health compromising behaviors (Hanlon, Bateman, O’Grady, Simon, & Carswell, 2004 ). In addition to demographic characteristics, the principal areas of self-reported information provided by the youth included the extent of participation in risky behaviors, family stability and functioning, the deviance of peer associates, and school interest and performance.
Administered in a private location and involving responses to structured interview schedules, the assessment instruments used in the program had been uniformly shown to be reliable and valid in previous research (Carswell, 2007; Carswell, Hanlon, O’Grady, & Watts, in press; Hanlon, et al., 2004; Hanlon, Bateman, Simon, O’Grady, & Carswell, 2002; Hanlon, Simon, O’Grady, Carswell, & Callaman, 2009). Brief descriptions of these instruments, in terms of their use in deriving the risk and protective measures examined are presented below.
Center for Substance Abuse Prevention (CSAP) Questionnaire. The CSAP survey (2002) was used to measure the degree of student involvement in the family. It was also used to measure Parental Monitoring, as well as the Educational Aspirations and School Connectedness of the students. Youth Self-Report Questionnaire (YSRQ). Developed and utilized in previous research with urban, African American youth (Carswell, 2007; Carswell et al., in press Hanlon et al., 2002, 2004, 2009), the YSRQ provided demographic information, along with information on the extent of youth involvement in delinquent behavior. This latter information included measures of Youth Deviance in terms of the extent of the variety of deviant behavior involved, ranging from minor property damage to various types of theft, drug distribution, and violence-related behavior. Youth Risk Behavior Surveillance (YRBS). Items from the YRBS (Eaton et al., 2006) were used to measure Substance Use included ever having tried cigarette smoking, had a drink of alcohol (more than a few sips), and/or used marijuana. The YRBS was also used to derive a Risky Sexual Behavior dimension in terms of the age at first initiation and extent of sexual intercourse involvement, which served as an outcome measure in the analysis of the relationships between risk and sexual behavior. Our designation of the intercourse experiences that the students reported as “risky” is based on an assumption of an increased possibility of inconsistency in condom use among our adolescent students over time, as well as the greater exposure of many of these youth to sexually transmitted infections associated with the disinhibiting effects of alcohol, marijuana, and other mind-altering substances and the likelihood of indiscretion associated with their involvement with multiple sexual partners on multiple occasions. FACES II. The FACES II (Olson, Portner, & Lavee, 1988) was used to derive an overall measure of family functioning in terms of Family Cohesion and Adaptability. Family cohesion items of the combined scale reflect the degree to which bonding exists between and among family members; adaptability items indicate the extent interactions within the family are equitable among family members. Friends’ Delinquent Behavior-Denver Youth Survey (FDB-DYS). A measure of Peer Delinquency, the FDB-DYS (Institute of Behavioral Science, 1990) consists of a participant’s perception of the extent to which his (her) friends violated rules or laws at home, school, or in the community.
Descriptive statistics and internal consistency reliabilities for the risk factors derived from the above instruments are presented in Table 1.
Baseline Descriptive Statistics for Risk/Protection Measures (N = 222).
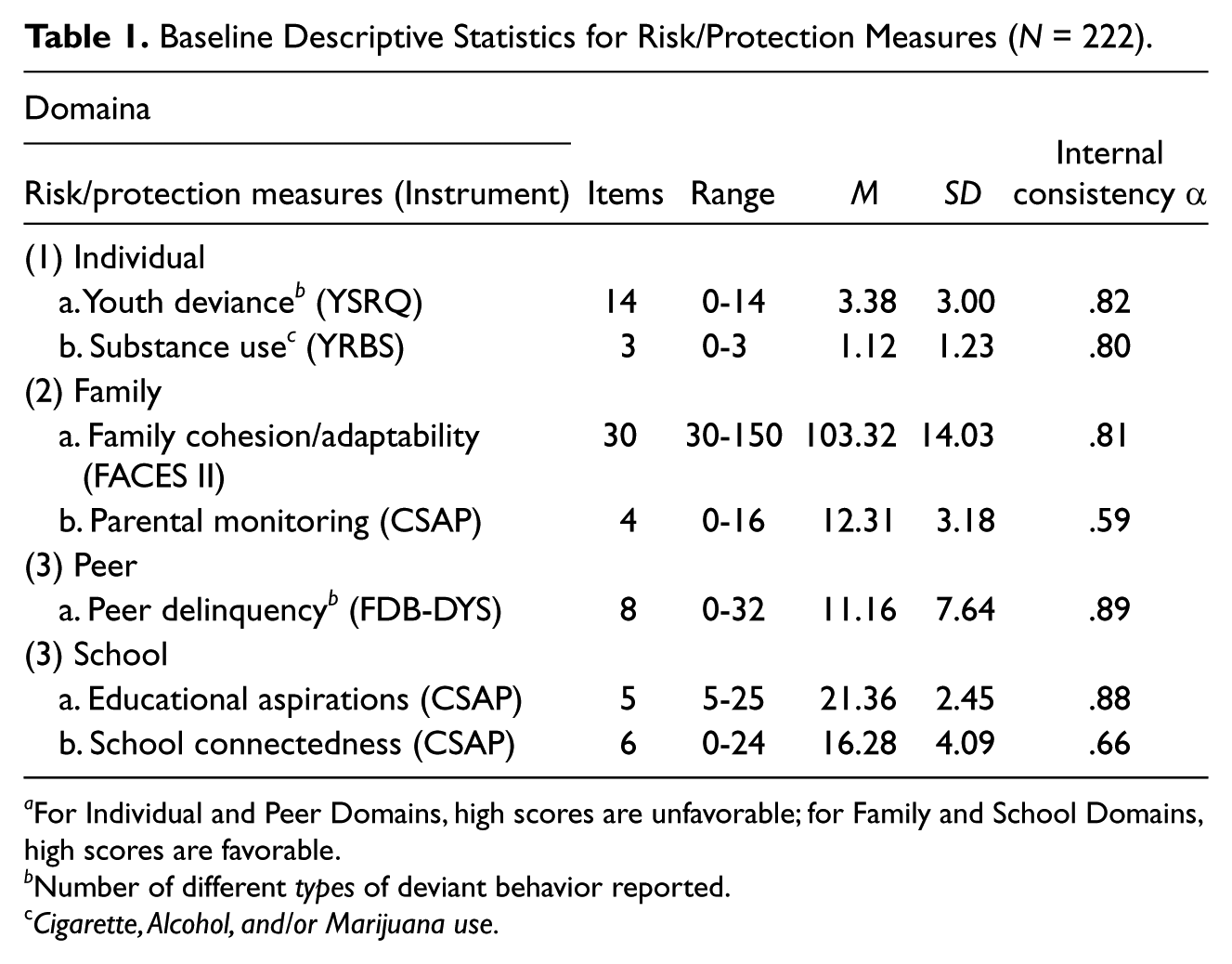
For Individual and Peer Domains, high scores are unfavorable; for Family and School Domains, high scores are favorable.
Number of different types of deviant behavior reported.
Cigarette, Alcohol, and/or Marijuana use.
Examination of the Relationship of Risk Factors to Sexual Activity
Little is known about the sexual practices of urban African American youth referred to AEPs. However, the limited information that is available indicates that, compared to regular urban school students, this group of African American youth is particularly vulnerable to the eventual development of an STI because of their exceptionally high rates of involvement in multiple risk-taking behaviors, including early engagement in sexual intercourse (Carswell et al., 2009; Grunbaum et al., 2001; Shrier & Crosby, 2003). Addressing the lack of information in this regard, this initial phase of our research examined developmental, social, and environmental aspects having a bearing on the sexual practices of these youth, focusing particularly on the impact of selected risk and protective factors associated with involvement in such practices.
Over a 4-year study recruitment period, 222 (155 male and 67 female) African American students who volunteered to participate in our research program were administered a comprehensive behavioral assessment designed to determine the behavioral characteristics and risk-related personal predispositions of the students in our sample. Obtained prior to an examination of the process and effectiveness of the proposed preventive intervention, the self-report information obtained from this baseline assessment was used to determine the relationship between specific risk and protective factors and risky sexual behavior. Findings from this first phase revealed that for the characteristics and factors examined, there was a significant relationship between developmental risk and protective measures and lifetime engagement in risky sexual behavior. Overall, these findings illustrated the relatively high rate of risky sexual activity among our sample of urban African American AEP students; the relevance of HIV prevention programming for such youth; the positive relationship between alcohol, tobacco, and drug use and involvement in risky sex; the feasibility of the identification of characteristics and risk factors that underlie vulnerability to long-term health-compromising behavior; and the important role that parental monitoring plays in preventing risky sexual behavior. A detailed description of the rationale and findings of this phase of our research is contained in a separate report (Carswell et al., in press).
Examination of the After-School Implementation Process
The second phase of our research involved an examination of the background, implementation, and feasibility findings associated with conducting an after-school intervention program in an alternative education setting designed to prevent the initiation and escalation of problematic behavior among at-risk urban African American youth. Evolving from an earlier preventive intervention strategy implemented in clinic and school settings that targeted at-risk middle school youth, the after-school program examined, entitled The Village Model of Care (VMC), consisted of the provision of academic assistance along with group mentoring, parental support, and community outreach services during the school year (Carswell et al., 2009).
Over the initial 2 years of the 4-year intake period of the overall program, 109 AEP youth had volunteered to participate in an after-school preventive intervention research program that included an intervention and no intervention condition. In this second phase, process evaluation findings from the implementation of the intervention not only provided relevant demographic and assessment information on the characteristics of youth likely to be included in urban alternative education programs, but also had a direct bearing on the planning and execution of future prevention efforts conducted in similar settings aimed at reducing problem behaviors among minority high-risk urban youth.
Besides revealing a general lack of participation of parents in the school-based rehabilitation program and the complications associated with the multiple needs of the families involved, our intervention process findings illustrated the importance of providing sufficient school administrative system support and resources essential to ensure the viability of sustained alternative education program efforts. Specifically related findings in this regard included the importance of the provision of strict monitoring and enforcement of student attendance within the school administrative system; the availability of appropriately trained AEP staff to deal with frequently occurring problematic student behavior; and the allocation of adequate physical space and resources for supplemental program activities; and the advisability of conducting prevention efforts as an integrated component, rather than an extension, of the overall AEP program. Process findings also highlighted the need to establish student assessment and triage procedures that would allow the provision of a relevant vocational education supplement to a basic remedial education approach. A detailed presentation of these and related findings in this process evaluation phase of research is contained in an earlier publication (Carswell et al., 2009).
The Evaluation of the After-School Intervention
Besides offering remedial academic support, the after-school preventive intervention program conducted with our AEP youth involved three major components: (a) group mentoring that primarily involved remedial education and emphasized positive peer relationships and character development; (b) parental support services that involved the participation of parents in bimonthly family gatherings held at the AEP; and (c) community outreach services that involved the provision of case management services to families and student educational activities in the community. The prevention program approach utilized a strategy that focused on promoting positive change in characteristics and dispositions that influence youth during their adolescent years.
Intervention study procedures
Using a counterbalanced design, one of two participating alternative education school sites was determined on a chance basis to serve as the after-school intervention site in years one and two of the trial and to serve as a no intervention comparison site in years three and four, while the second school served as a comparison school in years one and two and as the after-school experimental site in years three and four. In terms of the characteristics of the geographic areas and general populations served, the two sites were located in neighborhoods equally representative of high-risk urban settings based on census tract public health information.
Reflecting the racial composition of the urban communities in which the school sites were located, all study participants were African American, and as indicated, were also considered to be at high-risk for academic failure and escalating behavioral problems. Administered throughout the school year, the VMC intervention routine involved a combination of after-school 2- to 3-hour mentoring sessions administered 5 days per week; bimonthly scheduled gatherings of students with their families at the AEP; case management services to families; and organized educational field trips.
Prior to entry into the intervention phase of the overall research program, all participants had been administered the above described comprehensive battery of assessments that included structured interview and standard behavior inventory information provided by the students. As indicated, this battery, along with school record information relating to school achievement, present functioning, and adjustment, served as the pre- and post-assessments (conducted at the end of the school year) for the after-school intervention trial. For each of the 4 years of the intervention process, research program volunteers who entered the intervention were assigned by AEP site to either the intervention or no intervention condition. In addition to the standard AEP curriculum, those administered the intervention condition were enrolled in the VMC after-school prevention program, which was conducted an average of 4 days a week during the school year. Participants admitted to the designated comparison site received no research-related preventive intervention other than that associated with the standard AEP curriculum, which primarily involved remedial instruction and crisis/behavioral counseling. Assessments involving the same instruments administered at baseline were conducted at both sites at the end of each school year.
Intervention sample characteristics
Over a 4-year period, 205 of the 222 AEP youth who volunteered for the research program subsequently entered the after-school intervention phase of the program, 154 of whom received both a baseline and post intervention assessment (see Table 2). Seventy-five of these 154 participants had been assigned the prescribed VMC after-school program, and 79 to the no after-school programming condition. This completer intervention sample of 154 AEP students consisted of 111 males (72%) and 43 females (28%), ranging from 11 to 16 years of age (M = 13.86; SD = 1.17). With respect to demographic, academic, and school behavioral information, slightly less than one third of the students were in the 15- to 16-year-old category, just over one-half were enrolled in the 8th grade and approximately 80% participated in the free or cost-reduced breakfast and lunch programs. Almost all (96%) had at one time or another been suspended from school; 78% had been expelled; and 51% had failed at least one grade. With regard to family structure, almost three fourths of the youth were living in single parent homes, most of them living with their mothers (in only 34% of the cases was there a father figure currently in the home); and 16% of the students were being raised by their grandparents.
Demographic Characteristics of the Intervention Phase Completers (N = 154).
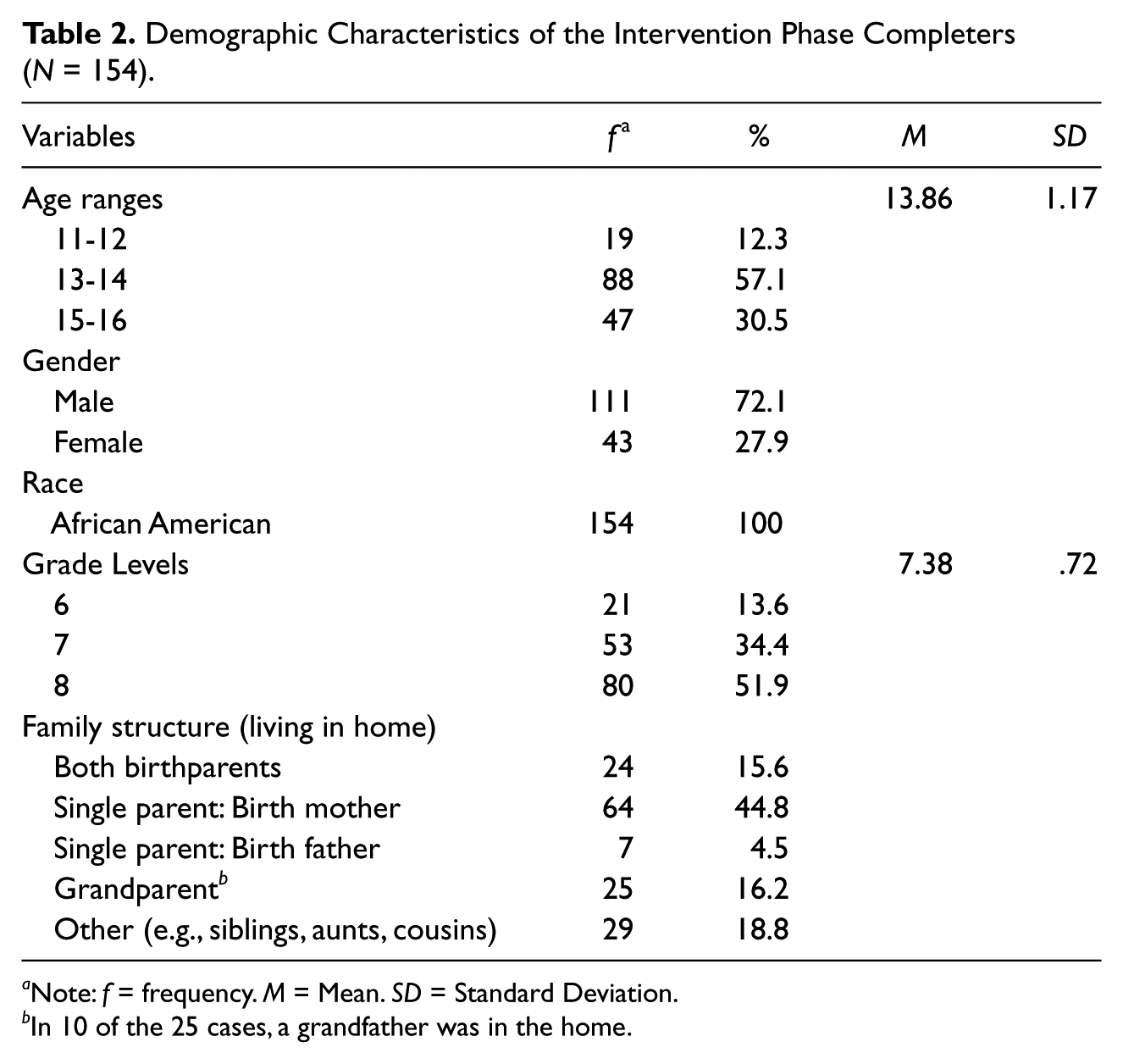
Note: f = frequency. M = Mean. SD = Standard Deviation.
In 10 of the 25 cases, a grandfather was in the home.
Self-reported information provided by the students at AEP school intake indicated that almost half (48%) had engaged in substance use, defined as ever having used cigarettes, alcohol, and/or marijuana. Seventeen percent of the sample reported having used all three substances. Although there were no significant gender differences with respect to ever having used any one of these substances (respective male/female percentages were 48% vs. 56% for use of either cigarettes, alcohol, or marijuana), almost twice as many females as males reported the use of all three substances (25.6% vs. 13.8%).
With respect to reported lifetime involvement of the 154 students in risky sexual behaviors at baseline, 92 (60%) reported having engaged in sexual intercourse at one time or another over their lifetime. Respective percentages of engagement for the male and female students were 66% and 44%. For those reporting that they had engaged in sexual activity, the average age at first intercourse for males was significantly younger than for females, and the percentage of males having engaged in intercourse with a lifetime total of 4 or more individuals was significantly greater than that for females.
Intervention evaluation findings
The general linear mixed model (GLMM; Breslow & Clayton, 1993; McCulloch & Searle, 2001; Wolfinger & O’Connell, 1993) was the principal method for examining treatment effects. Although this model can be seen as an extension of the “traditional” mixed-model ANOVA, log-linear, and logistic regression models, GLMM requires fewer distributional assumptions, is more robust to violation of the restrictive assumptions of these latter models, allows for the appropriate estimation of random effects and their standard errors, and is considerably more flexible in dealing with missing data.
For the sample involving those 154 students completing both baseline and post assessments, the latter conducted at the end of the school year, GLMM analyses were conducted that in all cases included the following independent measures: Gender; Age; Study Condition (Intervention and No Intervention); and Cohort (1st 2 years vs. 2nd 2 years). Covering four contexts, or domains, of interest (Individual, Family, Peers, and School), the dependent measures that were separately examined in these analyses included the following variables as outcome measures, each of which was representative of a key prevention target area: CSAP Family Involvement, Parental Monitoring, Educational Aspirations, and School Connectedness; YRBS Risky Sex; YRBS Substance Abuse; YSRQ Youth Deviance; FACES II Family Cohesion/Adaptability; and FBD-DYS Peer Deviance. For all of these analyses, we found no significant outcome differences favoring the intervention over the no intervention condition.
To determine the extent to which after-school program attendance was related to outcomes, we then conducted GLMM analyses of the same dependent measures, as above, using the following independent measures: Gender; Age; Cohort, Program Attendance (high vs. low, i.e., 50% or more vs. less than 50% attendance of scheduled after-school program days). In these analyses, which included the intervention group only, no significant differences in treatment outcome results were found for the 1st and 2nd vs. 3rd and 4th years of intervention implementation nor were they found for high vs. low program attendance.
In addition to the above GLMM results, the findings of supplemental analyses of AEP school records, including promotional status, disciplining infractions, grade point average, and attendance covering the school year period, also revealed no significant, nor otherwise noteworthy, differential outcome effects between the intervention and no intervention conditions.
Research Outcome Findings and Suggested Future Direction
Evidence of differential effects favoring the intervention condition in our evaluation research, which focused primarily on risk reduction, were negligible to nonexistent. The lack of differential effects favoring the intervention condition in this evaluation phase of our research is disappointing, but not surprising, considering unfavorable process findings with respect to implementation of the intervention. These included: site-related difficulties associated with an unanticipated relocation of the AEP school serving as the intervention site during the third year of the study; school staff shortages, which contributed to the instability of the alternative education program at this site; a pervasive inaccessibility of parents and their lack of participation in program activities; chronic student participant recruitment problems in a prevention program requiring an extension of the school day; student behavioral problems and/or disruptive acts during program implementation; and high AEP school absenteeism, which obviated participation in after-school programming. (At the post evaluation, one third of our sample reported having been absent from school over 50% of the time in the preceding four weeks.) Besides prompting changes in our preventive intervention strategy, these experiences highlighted the need for substantially more city-wide school system oversight, support, and commitment to AEP programming targeting at-risk, urban minority youth.
Many of the difficulties we encountered in the intervention phase of our research were associated with the implementation of an after-school preventive intervention that required extension of the school-day for participants whose prior school experiences had generally been negative and who were often absent from school. The following are program implementation recommendations based on both of these circumstances and on the process and outcome findings of our overall research program: (a) preventive interventions should be integrated within the AEP curriculum during regular school hours, with students viewing program activities as part of the remedial education process; (b) implementation should be undertaken by on-site AEP teachers familiar with, and specifically trained in, working with problematic AEP students; (c) the active involvement of parents in the prevention process should be aggressively pursued throughout the implementation of the program (ideally, a description of the prevention program should be included during the orientation of parents regarding available AEP resources); and, as noted above, (d) school system administrative support, including sufficient initial and continuous funding, particularly with regard to the allocation of necessary physical resources; monetary incentives to attract and retain qualified teachers to undertake the educational and disciplinary responsibilities of such a program; and the maintenance of student attendance requirements.
In implementing our preventive intervention, it was apparent that many of our adolescent participants were difficult to engage in a generally applied, academically oriented rehabilitative approach. There were, however, no available technical and other occupationally-related training alternatives available for these students and no routinely administered assessments of interests and aptitude testing to students in terms of the selection and pursuit of suitable career pathways. Ongoing school partnership arrangements with external resources, such as technical skills programs, offered by community colleges and local businesses were also lacking.
Research suggests that AEPs that have well-designed community partnerships with occupational programs, local employers, and/or community colleges are able to offer AEP students additional support services that may assist in meeting their needs, giving them a clear advantage over those alternative programs that lack such connections (de Velasco et al., 2008). Given the currently depressed state of the nation’s economy and its inevitable negative impact on urban minority youth, there is an obvious need for the wider availability of technical and other occupationally-related training and opportunities at AEPs, which may require not only local, but national sponsorship to establish. (Interestingly, a citywide restructuring of the local school system has since been proposed that includes the creation of new job training and career development initiatives targeting students within the system.)
With regard to our overall intervention findings, particularly the pervasiveness of school absences and dropout, it is clear that there remains an urgent need to develop effective evidence-based prevention programming to youth who are referred to urban alternative education programs, given their unique characteristics and needs, the magnitude of the life hazards and obstacles they face, and the ever-expanding population of high-risk students served by these programs.
In summary, our prevention implementation and outcome experiences indicate that to be successful, approaches undertaken within an urban AEP require that prevention efforts be an integral part of the AEP framework and that they do not extend the school day beyond regular school hours. With regard to the AEP approach itself, urban AEP’s targeting at-risk minority students require substantial system-level support and commitment, particularly with respect to the maintenance of student discipline and school attendance (a recently emphasized goal of the local school system). They also require the involvement of an exceptionally dedicated and trained AEP staff, an aggressive pursuit of the participation of parents in the remedial education process, and the broadening of student career-training options within the urban AEP network that are more immediately relevant to the interests of urban minority students and to the viable job opportunities that are available nationally and, even more importantly, locally in urban communities with limited opportunities for upward social mobility.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Award Number 5R00MD002271 from the National Institute On Minority Health and Health Disparities. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute On Minority Health and Health Disparities or the National Institutes of Health.
Author Biographies
![]()
![]()
![]()