
Abstract
Objectives:
Text message–based interventions may provide sexual health information to young people through a number of service types, from sending information on a regularly scheduled timeline, to providing an automated menu, to allowing young people to connect directly with health educators. While such service types exist, it is not clear which features young adults feel are most effective at allowing them to engage with sexual health information.
Design:
This study used a mixed-methods design (survey and focus groups) to assess perceptions of three types of sexual health text message services with young adults, a population particularly at risk of negative sexual health outcomes.
Setting:
College students from the US Pacific Northwest participated in the project.
Method:
Participants heard about three sexual health text message services, completed questionnaires and discussed each type. Focus groups were gender-separated.
Results:
Participants reported that services that allowed them to connect with a health educator would be highly useful, but automated services would be beneficial in bringing new topics to their attention. Participants perceived the purpose of the service types as different and felt each could be a useful resource, depending on the situation. Regardless of service type, participants wanted to personalise their experience. Participants wanted messages tailored to them and options to interact with the systems, from influencing topic selection to message timing.
Conclusion:
Each of the service types can be useful for young adults. Young adults perceive services that provide the opportunity to tailor information and interact with the system as beneficial.
According to the US Centers for Disease Control and Prevention (CDC, 2014), 15- to 24-year-olds make up just more than 25% of the sexually active population but account for approximately 50% of new sexually transmitted infections (STIs) in the USA each year. While approximately 16% of young people have engaged in sexual activity by the age of 15 years, this number rapidly increases from almost half for the last year of high school to nearly three out of four (71%) by the second year of college (Guttmacher Institute, 2014; Kann et al., 2014). With such prevalence of sexual behaviour, it is important to make sure young adults have access to comprehensive and accurate medical information related to sexual health.
New digital media, defined as user-driven interactive communication (Guse et al., 2012), are popular among young adults, as evidenced by their use of social networking sites, the Internet and cell phones. In all, 98% of young adults (aged 18–29) in the USA own a cellular phone, and 86% of 18- to 29-year-olds own smartphones (Anderson, 2015). Text messaging or short message service (SMS) is a popular feature used by adolescents and young adults, with 90% of 13- to 17-year-olds with cell phones or smartphones sending text messages (Lenhart, 2015). Additionally, college students have been shown to use text messaging as a primary form of communication (Skierkowski and Wood, 2012). Because of the popularity of such technology, health educators have developed text message–based interventions in an attempt to bring sexual health information to young people where they are at – on their mobile phones.
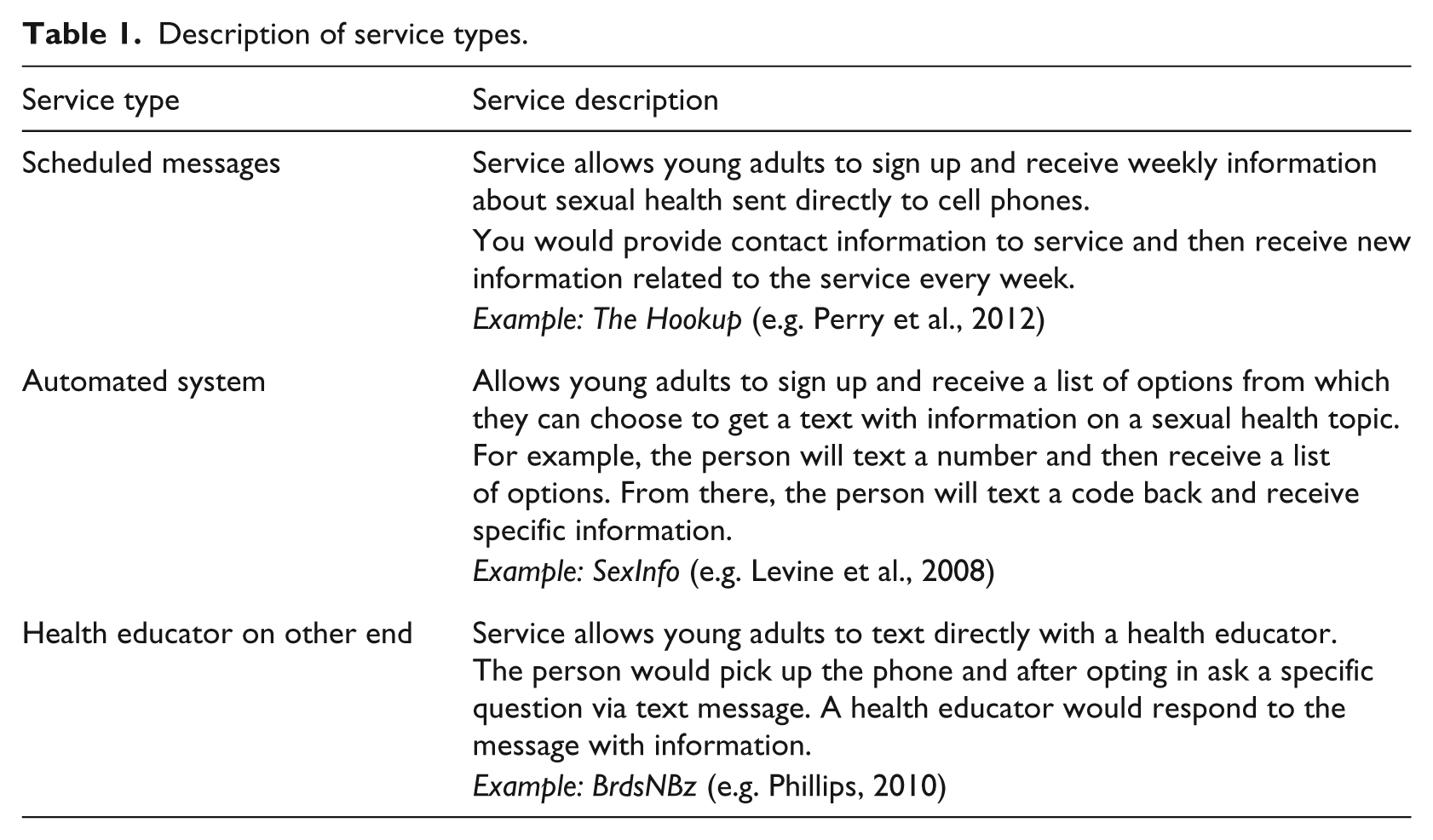
Generally, three types of SMS interventions for sexual health exist. The first allows for messages to be sent on a specific timeline to provide young people with health information (e.g. the Hookup, Perry et al., 2012; Sheoran et al., 2014). A second approach allows for the use of an automated system for users to select topics from a list of options in which they are interested to obtain health information (e.g. SexInfo, Levine et al., 2008). A third method allows for the back-and-forth between youth and a trained individual such as a health educator (e.g. BrdsNBz, Phillips, 2010; Willoughby, 2015). These service types are not necessarily mutually exclusive, as regularly scheduled messaging may also include an automated function to receive information on nearby clinics.
It is unclear which aspects of these different types of services young adults may find most useful. Such information could help practitioners and researchers develop more effective interventions aimed at increasing education about sexual health and improving sexual health–related outcomes. Researchers have encouraged scholars to investigate which approaches may be most effective for promoting healthier sexual behaviours among young people (Allison et al., 2012; Gilliam et al., 2014; Jones et al., 2014). This project uses a mixed-methods study to assess three different sexual health text message service types to determine what elements young adults see as most useful and how such services are perceived.
New media for health promotion
Mobile health, or mHealth, is the use of mobile devices for health information and health services (Noar and Harrington, 2012). Mobile phones are appealing for health promotion for a number of reasons, including the opportunity that mobile phones afford for the exchange of health information with a user ‘anytime or anywhere’ (Abroms et al., 2012: 151). Additionally, mobile phones offer the opportunity to tailor health information. Tailoring refers to using pre-assessed individual information to determine the specific content that will reach an individual (Kreuter and Wray, 2003). Evidence shows that in comparison with non-tailored messages, tailored messages can be more efficacious for a variety of health issues (Noar et al., 2007). In a recent review of text message–based interventions, researchers found that tailored interventions were associated with increased intervention efficacy, regardless of the health topic (Head et al., 2013).
Text messaging for sexual health promotion
Young people have indicated they are interested in receiving health information on mobile devices, such as through text messaging (e.g. Sheoran et al., 2014; Willoughby, 2013). In one study, researchers found that text messages were seen as a personal means of health promotion among young adults, and that messages may be seen as memorable and worthy of sharing, in some cases (Gold et al., 2010). In another study, researchers found that participants who received regularly scheduled messaging found the content to be informative, convenient and private (Perry et al., 2012). Similarly, in formative research that asked about participants’ perspectives of a two-way text message service for sexual health information, participants reported liking the convenience and anonymity afforded by the system (Willoughby, 2013).
In addition to being liked by young people, text message interventions for sexual health have been shown to be efficacious. Research has found that text message interventions may influence knowledge (Gold et al., 2011; Lim et al., 2012) and behaviours, such as getting tested for STIs and HIV (Sheoran et al., 2014). In a review that examined the impact of digital media on adolescent sexual health including digital technology beyond text messaging, researchers found that interventions impacted sexual health knowledge, attitudes and behaviours (Guse et al., 2012). Similarly, in a meta-analysis that examined the effects of new media interventions on sexual health–related outcomes, researchers found that new media interventions may impact behaviour change, with interventions that include an interactive component leading to increased success (Swanton et al., 2015). While these reviews may assess research that encompasses digital media beyond text messaging, they showcase the potential of using user-generated interactive channels to reach young people with sexual health information.
Interactivity is one aspect that may be influential in the possible success of mobile interventions. Interactivity is a ‘set of system affordances that allows users to manipulate the source, message, channel, and receiver combinations’ (Chung, 2012: 39). Interactivity may allow audience members to be a more active agent in the communication process (Chung, 2012). In research related to sexual health, researchers found that perceptions of interactivity (e.g. whether users felt the system was responsive, regardless of system functionality) were associated with increased positive attitudes towards the service, likelihood to recommend the service to a friend and repeat use (Willoughby and L’Engle, 2015). While both interactivity and tailoring may be a benefit of the use of mobile, it is unclear how target audience members (e.g. young adults) may perceive the different types of available services. This study attempts to provide some insight into which features of sexual health text message services young adults find beneficial.
Methods
We conducted five focus groups in February 2015. Three of the focus groups were conducted with women and two of the focus groups were conducted with men. Focus groups allow for individuals to build off of the information provided from one another in a relaxed setting (Leung and Savithiri, 2009). Participants were recruited from a participant pool in the authors’ college. Through the participant pool, students sign up to participate in research studies for course credit or extra credit, depending on the practice of their instructors. Participants signed up via an online management system and attended one of the five focus groups. We conducted focus groups until new information was not emerging during the focus groups.
During the focus groups, an experienced moderator (the first author) led the discussion. Results were recorded and transcribed. Focus groups were, on average, 45 minutes long. The Washington State University Institutional Review Board determined the study exempt from review.
Procedure
All participants were provided with information about the study and read and signed consent forms agreeing to participate. A protocol was followed during the focus groups. Focus groups began with a general discussion of participants’ resources for health information. The moderator then described one of three types of sexual health text message services (see Table 1 for a description) and provided an example. Participants were next asked to complete a short survey regarding their perceptions of the service. Once participants had completed the questionnaire, the moderator led a discussion on perceptions related to the described service. Questions covered topics related to participant attitudes towards such a service (e.g. what do you think of this type of service? Why might someone not want to use a service like this?), what participants felt users could learn (e.g. what do you think someone could learn from a service like this?), engagement with the service (e.g. how would a service like this help you get information about sexual health?) and potential negatives to using the service (e.g. are there any drawbacks to such a service?). The process was repeated two more times to get questionnaires and perspectives on all three types of services. After discussion of all three service types, questions were asked about overall opinions including which service was preferred or least preferred and why. We varied the order of the service descriptions to prevent order effects.
Description of service types.
Participants
In all, 31 college students participated. More women participated than men (women: n = 21, men: n = 10). Participants ranged in age from 18 to 26 years (M = 19.7, SD = 1.7). More than half (58%) of the participants were first year or second year students. A total of 16 participants identified as White/Caucasian, 6 identified as Black, 6 identified as Asian/Asian American/Pacific Islander and 3 identified as Hispanic. Approximately half (n = 16) reported receiving some form of financial aid.
Measures
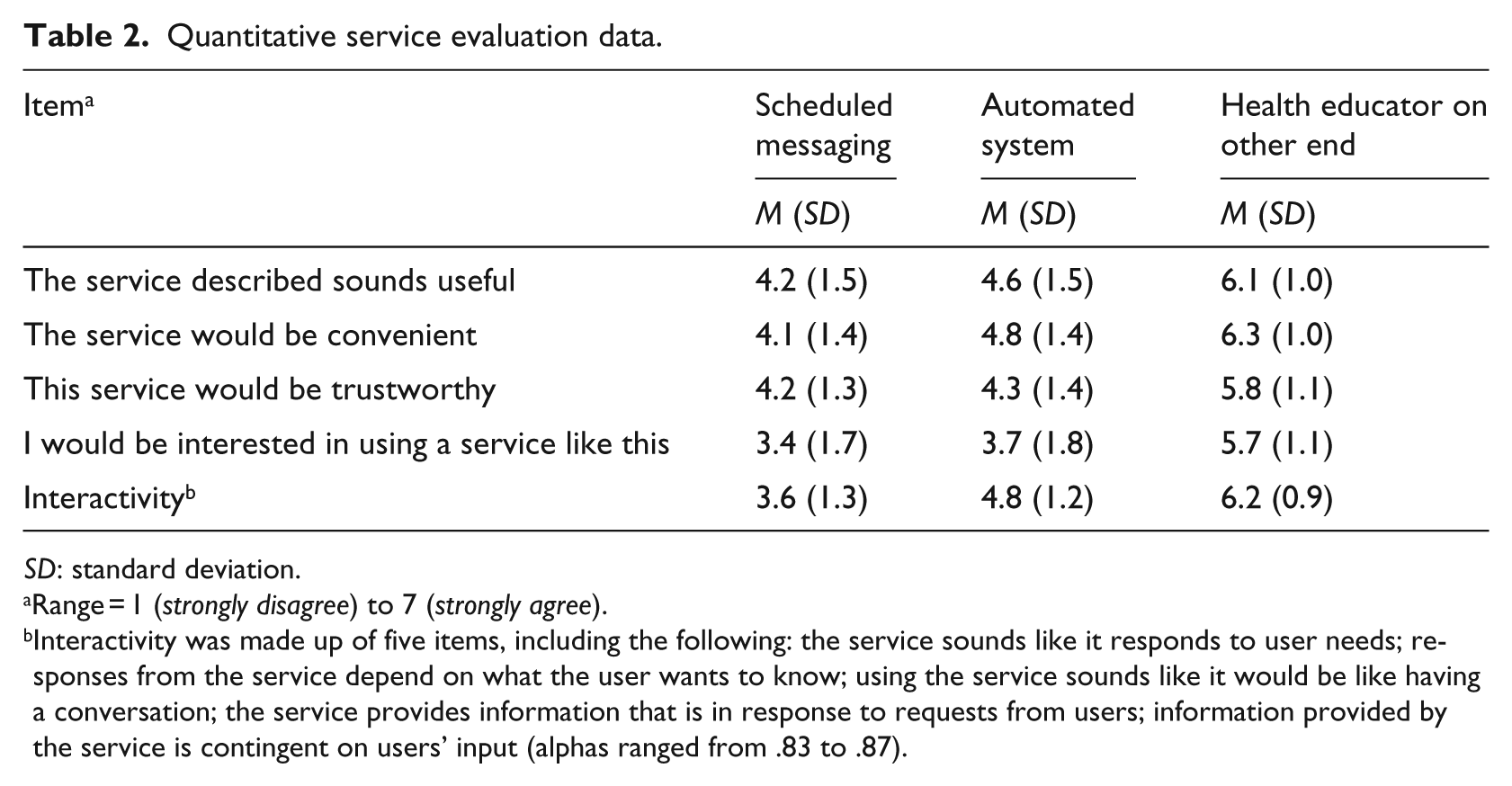
Single items were used to measure most constructs except for perceived interactivity. The item that assessed perceived service usefulness was adapted from previous research on attitudes towards a sexual health text message service (Willoughby and L’Engle, 2015). The perceived interactivity items were developed based on previous research in interactivity via text messaging (Willoughby and L’Engle, 2015) and previous work done on interactivity in advertising (Wu, 2006). The Cronbach’s alphas for perceived interactivity were above .80. All items used a Likert-type scale with 1 representing strongly disagree and 7 representing strongly agree. See Table 2 for all items, means and standard deviations.
Quantitative service evaluation data.
SD: standard deviation.
Range = 1 (strongly disagree) to 7 (strongly agree).
Interactivity was made up of five items, including the following: the service sounds like it responds to user needs; responses from the service depend on what the user wants to know; using the service sounds like it would be like having a conversation; the service provides information that is in response to requests from users; information provided by the service is contingent on users’ input (alphas ranged from .83 to .87).
Analysis
Quantitative data were collected and entered into the data analysis software programme SPSS 21.0. One-way repeated-measures analyses of variance (ANOVAs) were used to determine whether there were significant differences between service types on the outcome variables.
Qualitative data were transcribed and analysed using the constant comparative method, which allows researchers to look for trends and relationships based on information presented by participants (Charmaz, 2007; Corbin and Strauss, 1990). Both authors analysed the transcripts independently by hand, coding for themes that emerged. The authors then met to discuss the themes and create categories that represented higher level representations of concepts identified during the focus groups (e.g. Corbin and Strauss, 1990). Any discrepancies in coding were discussed and final codes were agreed upon by both authors.
Results
Quantitative results
There was a significant effect for service type on perceptions that the system was useful: Wilks’ Lambda = .41, F(2, 29) = 20.96, p < .001, multivariate partial eta squared = .591. Means and SDs are presented in Table 2. Services that connect participants directly with a health educator were seen as significantly more useful than either of the other systems – automated or those that send regularly scheduled messages (p < .001). However, all systems were rated as somewhat useful.
Convenience also significantly differed based on service type: Wilks’ Lambda = .37, F(2, 29) = 24.73, p < .001, multivariate partial eta squared = .630. There were no significant differences between the automated and scheduled systems, but both differed significantly from the systems that allow for a back-and-forth with a health educator (p < .001).
Perceptions of trust also differed based on service type: Wilks’ Lambda = .50, F(2, 29) = 14.78, p < .001, multivariate partial eta squared = .645. Again, there were no significant differences between the automated and scheduled systems, but both differed from the systems that allow for a back-and-forth with a health educator (p < .001). Once again, while there were significant differences, all services scored above the mid-point on trustworthiness.
Interest also differed based on the service types: Wilks’ Lambda = .35, F(2, 29) = 26.82, p < .001, multivariate partial eta squared = .649. Again, there were no significant differences between the automated and scheduled systems, but both differed from systems that allowed for back-and-forth with a health educator (p < .001).
Interactivity perceptions differed based on the service types: Wilks’ Lambda = .29, F(2, 29) = 35.88, p < .001, multivariate partial eta squared = .712. For interactivity perceptions, all services types differed significantly from each other (p < .001), with the back-and-forth system seen as most interactive, followed by the automated system and then the scheduled messaging.
Qualitative results
A number of themes emerged from the focus group discussions. Themes did not differ by participants’ gender. Participants expressed interest in all the service types, but felt text message services in general might be more appropriate for a slightly younger audience. However, participants still saw value in what the services could offer. Participants also had recommendations on how to improve such services. They appreciated the control that was offered by some services, as well as the potential to personalise information and messages. Credibility, trustworthiness and timing also came up across multiple focus groups. All names used in the manuscript are pseudonyms, used to protect participant confidentiality.
Service types
Participants felt that each service type offered valuable features. When comparing the three services, participants indicated that the different types of services met different needs. When talking about services that allow participants to receive regularly scheduled automated information, Kate said,
… it wouldn’t help your particular situation if you had one … it just gives you random knowledge every week, which could be useful, but at the same time you probably wouldn’t know something about what is happening to you right now if there is something.
Another woman found the automated service to be a good way to receive beneficial reminders. Tiffany said,
It’s good to get the information when you aren’t pressured … if you are in a controlling relationship you might not see the signs, but if before the controlling relationship you got the signs, you might be like, hey, I remember something about this.
Participants also felt that services that send regularly scheduled messages could help provide new information that could spark interest:
Whatever is given to them in that text … that’s what these people could learn. If they aren’t interested, they don’t have to dig any deeper, and if they are, they could spend hours digging into the topic … I think it’s really good and could be useful, especially for someone who is busy and doesn’t have time to dive in to all this information and it is just sent to them and they are like, ah, sweet, I got my information for the week. (Meg)
Overall, when talking about services that provided automated responses to select topics, participants said that the services could be useful, maybe as an introduction to a topic. As Eli said, ‘I feel like this would lead to more though. This is just opening the door’.
Personalisation
The topic of control over information came up when discussing various service types. One concern participants had with messages that were sent on a regularly scheduled basis was the possible lack of control over the topics. As Meg said, ‘… If you aren’t interested in the topic of the week, then you are like, well, I wish they had sent me a better one, because everyone’s interests are different …’. When discussing regularly scheduled messages, participants felt that having an option to personalise the messages would be beneficial. According to Kyle, ‘Maybe like if it texted, hey, are you this, this, and this, and you say I’m a male and I’ve got this kind of stuff …’.
In one of the female focus groups, participants highlighted the importance of preference by recommending that such services allow participants to select information that is relevant to them before receiving messages:
… if it’s something you sign up for, and you do a quick survey, and they’re like, really broad topics, like click all that apply … then they send you more specifics on the broad topics in order of what was your most interested versus least. I think that would be really cool. I’m down. (Meg)
In making the point about the ability to have a choice in topic selection, participants referenced popular music applications that allow them to set preferences and then receive songs relevant to their liking. As Tiffany said,
… you tell them what you like and then every once in awhile they try something new and are like ‘hey, based on your previous answers I think you would like this’, and that could be good … and every once in awhile there is a random song on there where you are like ‘how did that get on my station’, and you either hate it and get rid of it or you like it and are like, actually that was kind of interesting.
Participants also wanted to have control over how and when they received information. One participant asked whether there were options to tell text message systems how many messages to send to you and when they would be sent, talking about how this would be useful. This was especially important in terms of timing, which was brought up in all of the focus groups. Participants felt having control was not just important to their liking of such services but also to their understanding of information. As Hannah said, ‘… sometimes it gets annoying the amount of information that’s thrown at us. So if we feel more in control of something, we respond to it better than something that’s forced on us’.
Timing
Timing came up as an important aspect for the various services. For services that connect a user directly with a trained individual, participants said that timing was important because such services might often be used in timely situations. As Sara said, ‘Let’s say the condom does break and they’re freaking out and they’re panicking. They could text this number … And it can snap into the mindset of that’s something I can do’. Participants also felt that automated systems had the benefit of being quick. As Haley said, ‘It saves a lot of time … you don’t have to go through all of the topics. I mean, it’s text to use. Okay, I just have to text back 5 or something …’.
Participants were also concerned about timing with regularly scheduled information, however, as they feared messages might appear at inopportune times or be too frequent and thus a source of annoyance. As Jackie said, ‘If it were weekly, it would probably drive me crazy’. Participants also felt that if messages were too frequent, users would tune out the information.
Credibility
When discussing the different service types, trust and credibility were brought up multiple times. Participants wanted to trust the information provided and have access to information from credible sources. The use of ‘text lingo’ (e.g. the use of ‘u’ as opposed to ‘you’) was something several participants expressed disliking and thought of as unprofessional, although a few said they did not see it as an issue. Aside from the appearance of the message, participants said they also felt that systems where you generally knew who was on the other end (e.g. a health educator) were more credible. When asked why, Hannah said, ‘Just because it’s not an automatic machine texting you back … They’re [health professional is] actually reading the question and giving you an actually informed answer’. However, some participants still had concerns about the credibility of an anonymous health educator, in comparison with a trained and certified health professional such as a nurse or doctor, citing a lack of a certification in personal consultation with someone as a potential barrier to using such systems.
Purpose
Participants identified the different service types as having different purposes. As Callie said, ‘I think it just depends on what you are trying to get out of the service …’. Participants highlighted that a regularly scheduled service could provide information they were not aware of that could be helpful in the future, but that a service that lets you communicate with a trained professional would be beneficial if an individual was in a specific situation and wanted an answer to a question. When discussing services that let you text with a health educator, Amy said, ‘I thought it was nice because it was direct. It seems like you could ask follow up questions …’. Jake stated that he did not really see the reason one might use a text message to communicate about sexual health, but that services that let you text with a health educator: ‘you could actually use a text because it feels like you’re talking to someone’. However, the drawback to such services was pointed out well by Mike, who said,
But the learning ability of it [services that connect with a health educator] will be dictated by the part of the user. So, you would not be able to learn stuff that you might not have thought about learning, whereas the other options give you things that you find useful, but didn’t think of in the first place.
Consequently, the manner of facilitating information was seen as a double-edged sword. Although some participants would enjoy complete personalisation and control over their selection of topics, others appreciated the ability to have some amount of control, but wanted flexibility to learn about sexual health topics of which they might not have had an initial interest.
Concerns
Privacy
Participants had a few concerns related to text messages and to specific system types. In general, there was a concern over embarrassment that could come from having someone else view the text messages, as participants felt that information about sexual health should be private. A discussion in a male group highlighted this after Jake said, ‘You might hand someone your phone, and they [accidentally] get the message’. To participants, some messages were more embarrassing among peers than other messages. As Craig said, ‘Especially the birth control one!’ (laughter from the group) ‘Like whoops!’ ‘So it might not even be relevant so then it’s just awkward’. Participants felt having control over the timing of when the messages were sent would help avoid potential embarrassment and help with concerns over privacy.
Over-reliance and disparities
An additional concern was too much reliance on such systems. While participants felt discussing sexual health questions with a health educator could be useful, especially in an anonymous setting, there was a fear that people might try to use such services as a replacement to seeking appropriate medical assistance, which participants saw as irresponsible. As Amy said,
Some people, since it seems pretty accurate, some people might use it as a replacement to going to an actual doctor. But you should not use anything as a replacement to going to a doctor. I still think you should use this as like, a before thing, and then going to the doctor.
Participants also expressed concerns that such a service might be relied upon more heavily by people of lower socioeconomic status who have fewer resources available to them, which could lead to lack of adequate professional care and the supplement of text message systems as opposed to obtaining appropriate treatment. However, other participants said that while such a situation could occur, they saw text message systems as a way to get around barriers related to location, status and class because everyone could use them. They still emphasised the need for appropriate medical care when applicable.
Discussion
This study looked at how young adults perceived a selection of text message services to determine their perceived usefulness and the elements young adults thought would be most effective. Participants felt that all the service types were useful and that each type offered something different to the user that could be needed. For example, an automated system that allowed for the pull of information was seen as a good starting point on specific topics, whereas a system that sent regularly scheduled messaging was thought of as a valuable way to gain new and unsolicited information that could be useful to users in the future. Services that allowed for young people to connect directly with a health educator were seen as a possible option when a specific situation was the issue.
The different purposes participants identified are particularly important to note, as certain health organisations and programmes may have different goals. If a goal is to bring young people new but relevant information, perhaps regularly scheduled messaging on a variety of topics is most appropriate. If the goal is to allow young people to learn specific information they may not have been able to receive from other sources, perhaps the back-and-forth with a health professional in an anonymous setting or an automated system would be more beneficial. Results from this study highlight the need for a variety of different types of services, depending on the goals of the service, service creators and target audience members.
One of the main findings from the focus groups was the importance young adults placed on personalisation. They wanted to control content and timing of messages. In a meta-analysis that examined the efficacy of text message–based health interventions, tailoring and personalisation were associated with intervention efficacy (Head et al., 2013). This research supports the need for mobile interventions for sexual health that can be tailored based on participant input. Participants wanted to have personally relevant information (e.g. tailored to relationship status, interests). A related concept, interactivity, also came up as a topic in the focus groups. Interactivity involves the control and flow of information related to the technological features of a system (Chung, 2012). Text message services that allowed for additional interactivity seemed preferential to young adults, as they again could engage in greater personalisation. Future research should examine mobile interventions beyond text messaging as a possible way to reach young adults, as there may be additional opportunities for tailoring and interactivity.
This study also echoed findings from previous research. For example, young adults did not like the use of abbreviations in text messages. Previous research found text message acronyms (e.g. LOL, meaning laugh out loud) too informal to be used in a healthcare text message programme (Woolford et al., 2011). In our study, not only did participants see such messages as inappropriate when they came directly from a health educator, participants wanted all service types to avoid the use of such abbreviations.
Interestingly, participants brought up embarrassment as a potential privacy concern with such services. While this is not completely novel, other studies have found that young people view text messages as a convenient and private form of gaining sexual health information (Perry et al., 2012; Willoughby, 2013). This finding may in part be related to the specific population used in this study. This project examined young adults, specifically college students, when previous research has often focused on adolescents (e.g. Perry et al., 2012; Willoughby, 2013). Perhaps there are differences in how these populations use and share content on their mobile devices that make embarrassment a more pressing concern for young adults. Future research should examine how adolescents and young adults use their mobile devices to determine whether there are differences in use and perception based on age.
Participants were also concerned disparities could cause problems by limiting the people who could access a service or limiting the care people might seek if a text service was available. Research to date shows some promising results. For example, a study that examined the feasibility of using cell-based communication with young people in an economically depressed area found that the majority of participants had cell phones, sent text messages and used other technology features (Sawni et al., 2016). Additionally, many were open to receiving health-related messages via mobile. In regard to whether text message service users will seek appropriate medical care, one study found that of users of a text service, 90% said they had made some behaviour change since they started using the service, and for 15%, that included getting tested for HIV or other sexually transmitted diseases (STDs) (Sheoran et al., 2014). While it appears that service use can be associated with healthcare use, more research could be done to continue to assess the issue.
Limitations
While this study provides interesting insights, it has limitations that must be considered. First, the sample limits the generalisability of the findings. Participants were from one university in the US Pacific Northwest. Opinions of young adults may differ based on a number of factors, including relevant sexual education training, which can vary by region. Second, participants in this study were young adults. Often, services are developed for adolescents as well as young adults, and attitudes and opinions about what may be useful may shift over time as experiences and knowledge change. However, young adults and college students in particular are a population for which sexual health information is highly relevant. Third, this study used focus groups and short questionnaires that consisted of mostly single-item measures. While focus groups can be beneficial because they allow for the building of information across participants, they also include barriers, such as the potential for group-think. The moderator tried to avoid group-think by inviting participants who had not spoken to engage in conversation and by acknowledging all viewpoints as valid. However, a different method might yield different results.
Recommendations
Based on the findings from this study, we offer the following three suggestions to service providers or creators of sexual health SMS interventions. First, determine specifically which purpose you intend your text message service to serve. If a specific county lacks access to accurate sexual health information and resources, or young people seem to have a number of questions they would like answered, a service that lets young people directly access a health educator or health professional may be useful. However, if a service is intended to spur new insights and knowledge, a system that sends messaging or allows for users to select from a list of information may be an appropriate option, as it does not require the user to solicit specific knowledge. Second, for services that provide regularly scheduled messaging, it may be useful to incorporate additional back-and-forth elements that allow for participants to follow-up. For example, some services that send regularly scheduled messages often include a link to additional information or an option to find local service providers. Such services can be useful as they provide opportunities for young people to not only gain new knowledge but also reach out and access additional resources as needed. Such engagement may also lead to increased perceptions of interactivity, which can influence service attitudes and use (Willoughby and L’Engle, 2015). Third, when possible, allow for the personalisation of messaging. Young people want to have some control over decisions such as general topic and timing. While it might not be feasible to tailor an intervention based on a number of specific criteria in all situations, just providing a feeling of personalisation may be useful. For example, research has found a placebo effect of tailoring (Webb et al., 2005), where participants may experience the benefits of tailored messages if they believe messages are tailored to them, although the messages were not tailored.
Conclusion
Text message services may differ in their design. Young adults recognise that such systems may also differ in the affordances they offer target audience members. Texting with a health educator may be useful when you have a specific question, but receiving regularly scheduled messaging can help individuals learn about new and relevant topics on which they might not have otherwise sought information. Personalisation and tailoring were brought up as something important to every service type. From selecting the timing of messages to the content conveyed, young adults wanted to have access to information directly related to them. They also were interested in systems that allow for interactivity, providing them with options to control system features. Text message services can be a useful way to convey sexual health information to young adults, as they readily have access to their cell phones, but allowing them to make choices, such as when the texts will occur or what content will be included, will help users engage with the information presented.
Footnotes
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.