
Abstract
Background:
In the UK, African communities are a focus of public health efforts to increase uptake of HIV testing. Mobile phone interventions may be an innovative way of reaching migrant groups who are known to face multiple obstacles in accessing mainstream health services. This paper presents findings from a feasibility study that used participatory approaches to investigate the use of a text messaging intervention to encourage HIV testing among migrant African communities.
Methods:
Participants were recruited in the city of Nottingham by a team of community researchers. They were sent two text messages per week (one on HIV and one on general health) for 12 weeks. Baseline and follow-up questionnaires were completed to measure HIV testing behaviour, HIV-related knowledge and attitudes and general health. Participants’ views on the intervention were solicited.
Results:
One hundred and sixty-nine participants were enrolled in the study. Follow-up data on HIV testing were obtained for 76 participants (45%) and complete follow-up measures were available from 60 participants (36%). Eight reported seeking an HIV test during the study period. There were statistically significant positive changes in attitudes about HIV and a trend towards increased knowledge about HIV. One-third of participants reported improvements in physical activity levels, diet and stress management following the intervention. The intervention messages and structure were positively evaluated.
Conclusion:
Well-designed mobile phone messaging proved to be a feasible and acceptable intervention to promote both HIV testing and lifestyle behaviours among African migrant communities in the UK. When co-constructed with communities, they hold considerable promise for overcoming some of the health-related barriers faced by migrant populations in new countries. Future research and service development should focus on exploiting and evaluating this potential in relation to other key health priorities.
Introduction
An important health issue facing African migrant communities in the UK is HIV (Public Health England, 2016). Between 30% and 50% of African migrants who are HIV positive are unaware of their diagnosis; risk perception is low and over 60% of those diagnosed are identified ‘late’ with a concomitant poorer prognosis (Public Health England, 2016). Low levels of testing occur despite a long history of community-based HIV prevention initiatives in these communities (National AIDS Trust, 2014). It is imperative to identify successful communication strategies to support HIV prevention among these groups (NICE, 2011).
Health education for migrant populations in the UK now takes place in a context of ‘super-diversity’ whereby migrants come from all over the world, are highly mobile, transnationally connected and represent widely varying languages and cultural identities (Phillimore, 2011; Vertovec, 2007). Such populations face many individual, health system and structural barriers to accessing health services (Ochieng, 2013; Rechel et al., 2013). These difficulties are compounded for HIV due to its stigmatised nature and fears of how a positive diagnosis may influence immigration processes (Blondell et al., 2015).
Globally, there is great interest in exploring how mobile phone–based interventions could address health education for migrant populations, with a particular focus on how they might enable access to information, peer support and resources (Liamputtong et al., 2016; Morley, 2017; Walker et al., 2015). With respect to HIV, short messaging service (SMS) interventions have been shown to be effective in supporting aspects of care (e.g. treatment adherence or retention), but there is less evidence on their utility in promoting HIV testing. Some studies have yielded promising results (Njuguna et al., 2016; Odeny et al., 2014), but these have been conducted in Africa. It is not known whether similar approaches would be effective among migrant African groups in high-income settings. African migrants in the UK have the highest level of household mobile phone ownership of all other population groups – at 97% (Ofcom, 2013), but there is a lack of research on patterns of use and ownership according to different socio-demographic features (O’Connor and O’Donoghue, 2015).
Study aim
The aim of this study was to test the feasibility of using a mobile phone SMS intervention to increase uptake of HIV testing among African communities in the UK. The intervention design and structure was guided by formative research to identify the challenges faced by communities around HIV testing, using the Health Belief Model (HBM) as a theoretical framework (see Evans et al., 2016, for a full description).
Methods
Research design
The feasibility study adopted a community-based participatory research (CBPR) approach, working in partnership with a pan-African community organisation, the African Institute for Social Development (AISD). CBPR is ‘collaborative, action orientated research … that involves the development of long term, equitable research partnerships between academic researchers, community based organisations and community members’ (Unertl et al., 2015: 1). This methodology was adopted for three reasons: (1) to address potential power imbalances within the research process so that all stakeholders had a voice and their contribution was recognised (Minkler and Wallerstein, 2008), (2) to ensure the intervention would genuinely reflect the needs and experiences of a diverse target group and (3) to build capacity within communities for ongoing advocacy around health (Trostle, 1992).
The study utilised a longitudinal one-group comparison design with data collected at two time points: baseline and post-intervention.
Ethics
The University of Nottingham Faculty of Medicine and Health Sciences Ethics Committee provided ethical scrutiny and approval (D09052013 SNMP). All participants provided written informed consent.
Setting
The study setting was Nottingham, a city of approximately 314,000 people in the East Midlands, UK. Its African migrant community is ‘super-diverse’ with an estimated population of 5,000 representing 31 different countries (African Initiative Support, 2010). Nottingham has a relatively high HIV prevalence of 2.78 per 1,000 population and high levels of late diagnosis (65.8% compared with the England average of 48.3%) (Nottingham City Council, 2015). HIV testing is free to all, regardless of migration status, and is available through public sector health facilities and voluntary agencies.
Sampling and recruitment
Participants were eligible to participate if they were African, over 18 years and could complete the surveys in English. A convenience and snowballing sampling strategy was used as is common in research on sensitive topics (Pitts and Smith, 2007). Recruitment took place over a 10-week period between March and May 2014. Individuals were invited to participate by a team of 12 AISD community researchers that represented diverse African communities and genders (Elliott et al., 2002). Recruitment occurred through direct referral within the community researchers’ social networks (Penrod et al., 2003) and visits to voluntary sector groups (e.g. refugee charities) and community venues (e.g. library or church). Participants were offered a GBP 5 shopping voucher to thank them for their time.
Text message intervention
The intervention was called ‘Health4U’. To avoid participants feeling stigmatised, the intervention embedded HIV text messages alongside general health messages, providing a consistent message that knowing your HIV status was an important part of overall health and well-being. It included 24 messages: 12 on HIV and 12 on other health aspects (see Evans et al., 2016, for a fuller description).
Participants started receiving text messages within 7 days of completing the baseline survey. Two messages per week were delivered for 12 weeks: one HIV message and one on general health (e.g. diet, physical activity, stress management, seeking appropriate medical help). Messages were limited to 160 characters and were personalised and tailored on religion (Christian, Muslim, neither), language (English, Arabic, French) and gender.
Outcome measures
Pre–post surveys were used to collect demographic, baseline and follow-up data (see Tables 1 and 2). The surveys were piloted with the community research team and 12 community participants. Where necessary, amendments were subsequently made to the items the team had developed (but not to the wording of standardised measures).
Behavioural and attitudinal measures.

Socio-demographic profile of study participants.

Behavioural and attitudinal outcomes were based on HBM constructs and recent research evidence. They included whether participants sought an HIV test during or immediately following the intervention and HIV-testing determinants, including previous testing history, intentions to get tested, changes in confidence to get an HIV test, HIV-related knowledge and attitudes to HIV testing (Evangeli et al., 2016a, 2016b).
Other outcomes included changes in perceived health status, perceived quality of life, diet, physical activity, stress management and confidence to seek appropriate medical help. Participants’ views on the acceptability of the intervention (content, frequency, duration) were also collected.
Data collection
At enrolment, participants were given the option of completing the baseline survey in paper format or online. At the end of the intervention, participants were sent an SMS requesting them to text a reply reporting whether or not they had sought an HIV test during the study period. They were also sent an SMS and email containing a link to the follow-up survey. Participants who did not complete the online follow-up survey were contacted via their mobile phone by a researcher who had not previously been involved in the study. If there was no reply after three attempts to contact the participant, they were considered lost to follow-up.
Data analysis
A researcher who had not previously been involved with the study entered the data and a 10% data check was undertaken. Statistical analyses were performed using IBM SPSS, version 21.0, while exact tests of symmetry were carried out using Stata IC, version 12.0. In order to control for Type I error due to multiple statistical tests being performed, a Bonferroni-corrected α of .003 was used to determine statistical significance. Descriptive statistics for ordinal data and continuous data that did not meet the assumptions of normality were reported using the median (Mdn) and range, which represented the lowest and highest scores reported by participants.
Results
Recruitment and retention
Of the 281 individuals invited to participate in the study, 172 agreed to take part (61.2%). Of those who agreed, three were excluded due to invalid telephone numbers. Hence, the intervention involved 169 individuals, who provided baseline data and were sent an SMS. Of the 109 who declined to take part, 46 provided a reason: 19 (41.3%) were not interested, 15 (32.6%) were ineligible due to nationality and 11 (23.9%) did not have time. Twenty-seven participants (15.9%) texted a reply to the final SMS reporting on their HIV testing behaviour. No participants completed the online follow-up survey. All participants were then contacted by phone and 60 (35.5%) completed the survey verbally. Combining the text replies and the survey, data on HIV testing uptake were obtained for 76 participants (45%).
Socio-demographic characteristics
Of the 169 participants, 85 were men (50.3%), 67 were women (39.6%) and 17 did not report their gender (10.1%). Ages ranged from 18 to 55 years, the majority were under 45 years (86.9%, n = 147). The majority of participants were Christian (60.4%, n = 102) or Muslim (26.6%, n = 45). Over three-quarters (78.7%, n = 133) were university educated. The majority of participants were either working (39.1%, n = 66) or studying (33.1%, n = 56). The participants represented all regions of Africa, yet the majority (89.3%, n = 151) selected English as their preferred language for the intervention.
Demographic characteristics of responders to the follow-up surveys were compared with non-responders. A 2 × 2 χ2 test of independence showed that fewer men (z = –2.1) than women (z = 2.1) completed the follow-up questionnaire, χ2(1, n = 152) = 4.38, p = .036. Fisher’s exact test showed that higher educational level (minimum of secondary school education compared with lower educational level) was associated with completion of follow-up measures (z = 2.4; p = .027). No other associations were found.
HIV testing
At baseline, almost two-thirds of participants (62.1%, n = 105) reported having ‘ever had’ an HIV test. There were no statistically significant differences in reports of ever having had an HIV test prior to the intervention between follow-up responders (64.8%, n = 35) and non-responders (68%, n = 70), χ2(1, n = 157) = 0.158, p = .691. Within the sample, 24.2% (n = 41) had tested more than 1 year ago and 30.8% (n = 52) had never tested. A relatively large proportion of the sample had tested less than a year ago (28.4%, n = 48).
Eight participants (10.5%) responded that they had sought an HIV test after receiving Health4U messages.
Confidence to seek a HIV test
Both before and after the intervention, participants were ‘very confident’ that they would be able to take an HIV test in the next 3 months (Mdn = 9 [1–10], n = 44, z = –0.527, p = .299). There was no statistically significant change in self-efficacy post intervention.
HIV-related knowledge
Changes in HIV-related knowledge were analysed using an exact test of symmetry for 3 × 3 contingency tables. Response categories for one item (‘If I have HIV, early testing will improve my chances of living a healthy life’) were collapsed into a 2 × 2 contingency table (correct vs incorrect response) in order to run McNemar’s test. Univariate analysis showed that after receiving the intervention, significantly more participants identified that early testing would improve their chances of living a healthy life (p = .006), that HIV testing is free to anyone in the UK (p = .007) and that they would know where to get a test (p = .006), compared with baseline. However, after statistical correction for multiple testing (Bonferroni-corrected α of .003), these relationships became non-significant (see Table 3).
HIV-related knowledge.
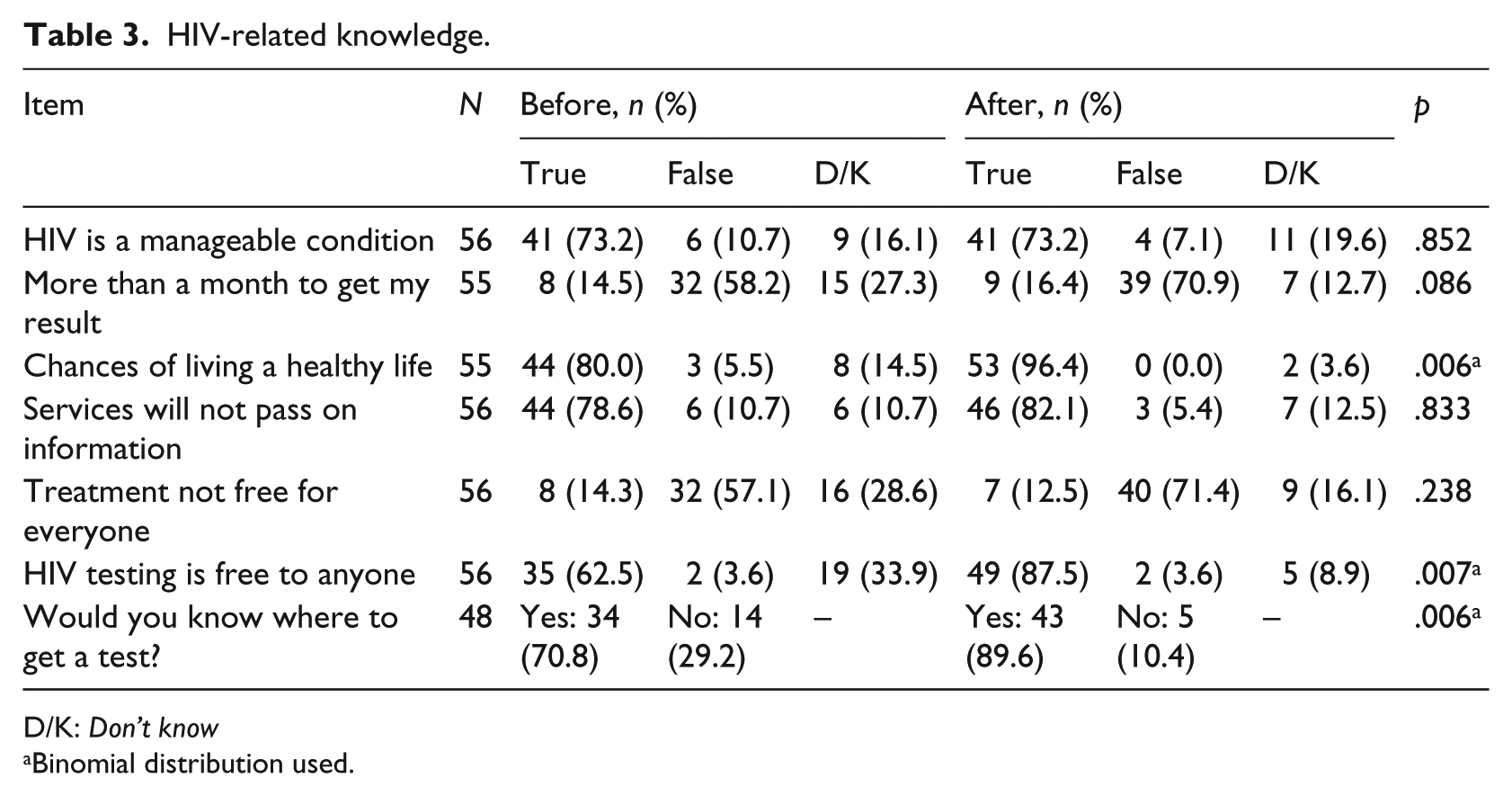
D/K: Don’t know
Binomial distribution used.
HIV-related attitudes
Some changes in HIV-related attitudes were observed. Participants were significantly more likely to strongly agree with the statement ‘If I had HIV, I know I would get the support I need’ at follow-up compared with baseline (Mdn score (range): before = 6 [1–7]; after = 7 [1–7]). Participants were significantly more likely to agree with the statement ‘Early testing will help me protect others from infection’ at follow-up compared with baseline (Mdn score (range): before = 7 [1–7]; after = 7 [5–7]). Both significant changes had medium-sized effects (r = –.44; see Table 4).
HIV-related attitudes.
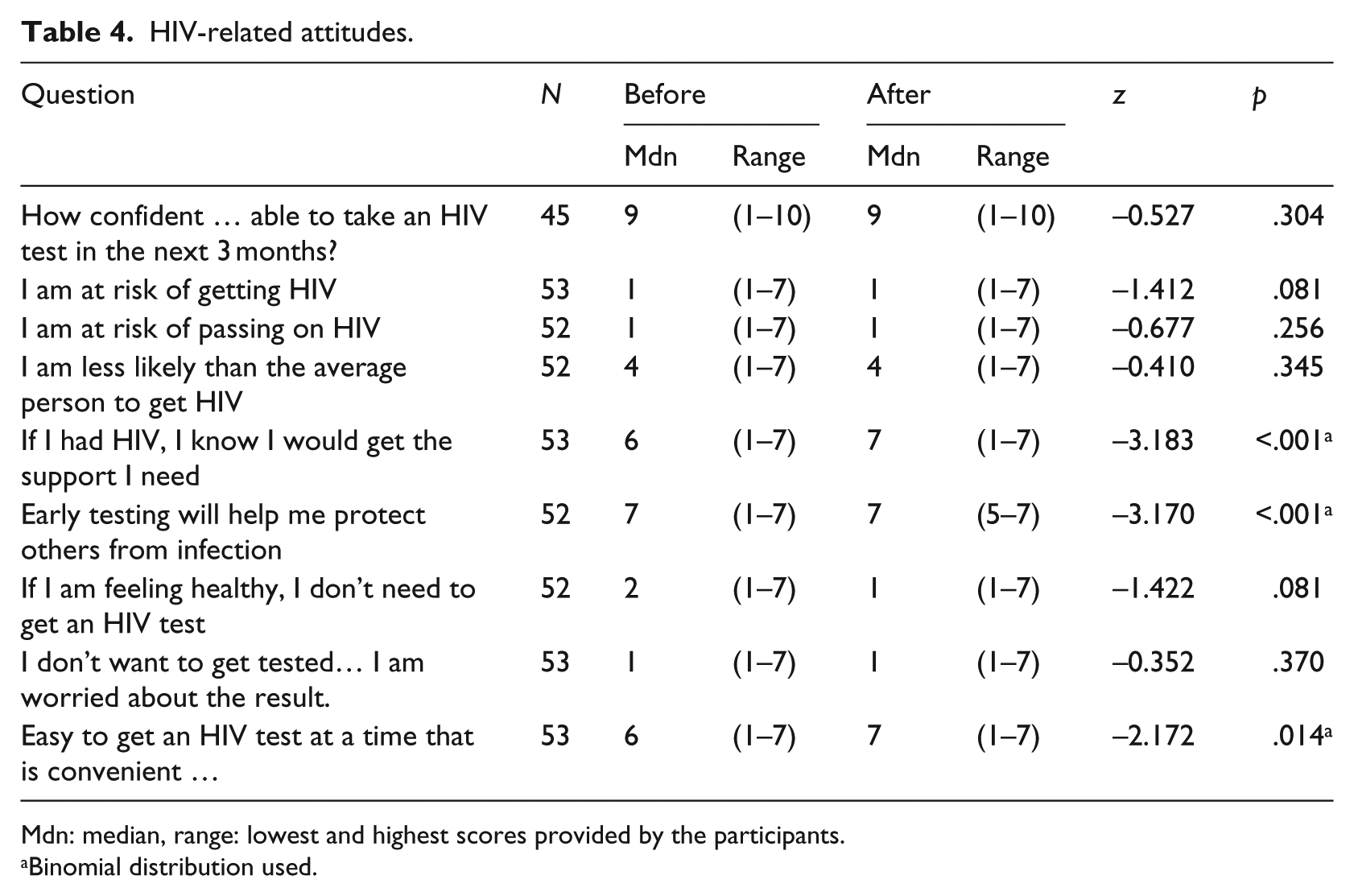
Mdn: median, range: lowest and highest scores provided by the participants.
Binomial distribution used.
Intentions to get an HIV test
Using an exact test of symmetry, a significant difference was found in participants’ intentions to get tested before and after the intervention (p = .0015). More than half of the participants who responded to the post-test question reported a change in their intentions to test following the intervention (31/55; 56.4%). Post hoc analysis showed that this significant difference applied to participants who said that they had been tested for HIV at baseline (n = 35); after the intervention, a significant proportion of this previously tested subgroup indicated that they ‘have actively looked into getting tested’ (22.9%, n = 8), ‘have thought about it’ (20%, n = 7) or ‘don’t have any plans to get tested’ (20%, n = 7).
Perceived health status, quality of life and other health behaviours
Changes in perceived general health and quality of life were analysed using the Wilcoxon signed-rank test. All rated their general health status as 2 = Very good (range = 1–5) both before and after the intervention, and hence, no statistically significant change was found (n = 60, z = –0.182, p = .434). There was a significant improvement in quality of life at follow-up compared with baseline (p = .013, n = 53), although when a Bonferroni-corrected α level was applied this change no longer reached statistical significance (Table 5).
Pre–post comparisons for general health status and quality of life.
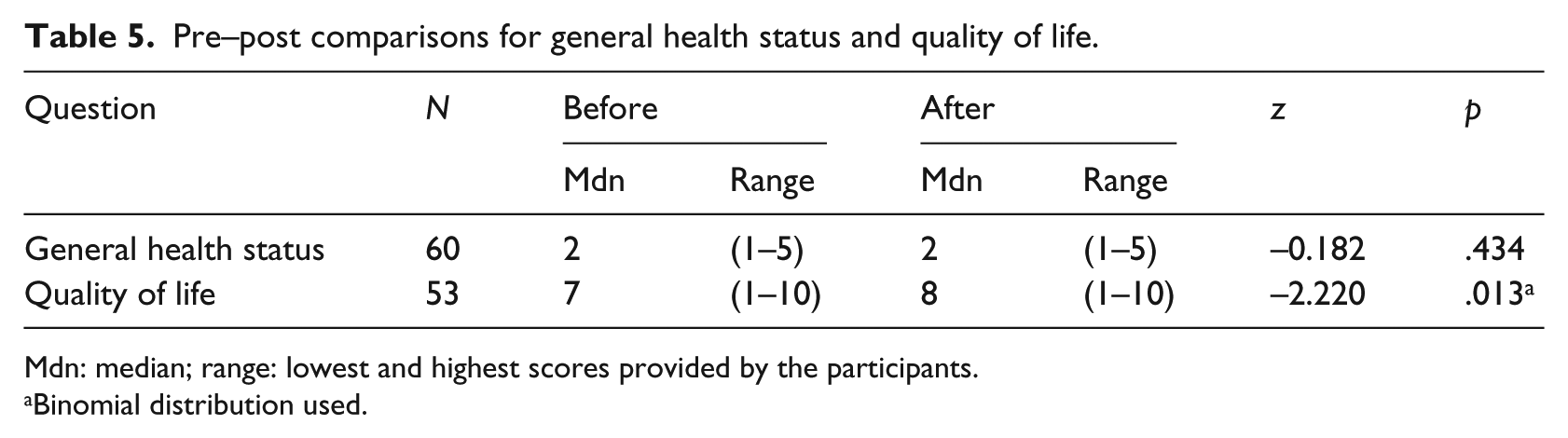
Mdn: median; range: lowest and highest scores provided by the participants.
Binomial distribution used.
With regard to other health behaviours following the intervention, 35.4% of participants self-reported an increase in their physical activity; 29.8% said that they eat healthier and 27.2% said that they were better able to manage their stress. At follow-up, respondents generally felt ‘very confident’ that they would seek out medical help (Mdn = 10 [5–10], n = 47).
Evaluation of the intervention
Fifty-two participants (30.8% of the total sample) provided feedback about the frequency and duration of the intervention. Of these, 59.6% (n = 32) were satisfied with the frequency of the messages. Five wanted more messages (9.6%) and 15 said there were too many (28.8%). Regarding intervention duration, 59.6% (n = 31) stated it was just about right, with 7.7% (n = 4) wanting a longer intervention and 32.7% (n = 17) a shorter one.
On Likert-type scales of 1–7, participants tended to agree with positive statements about the intervention and the personal relevance of messages and reported to have discussed the message content with others (see Table 6).
Participant evaluation of the intervention.
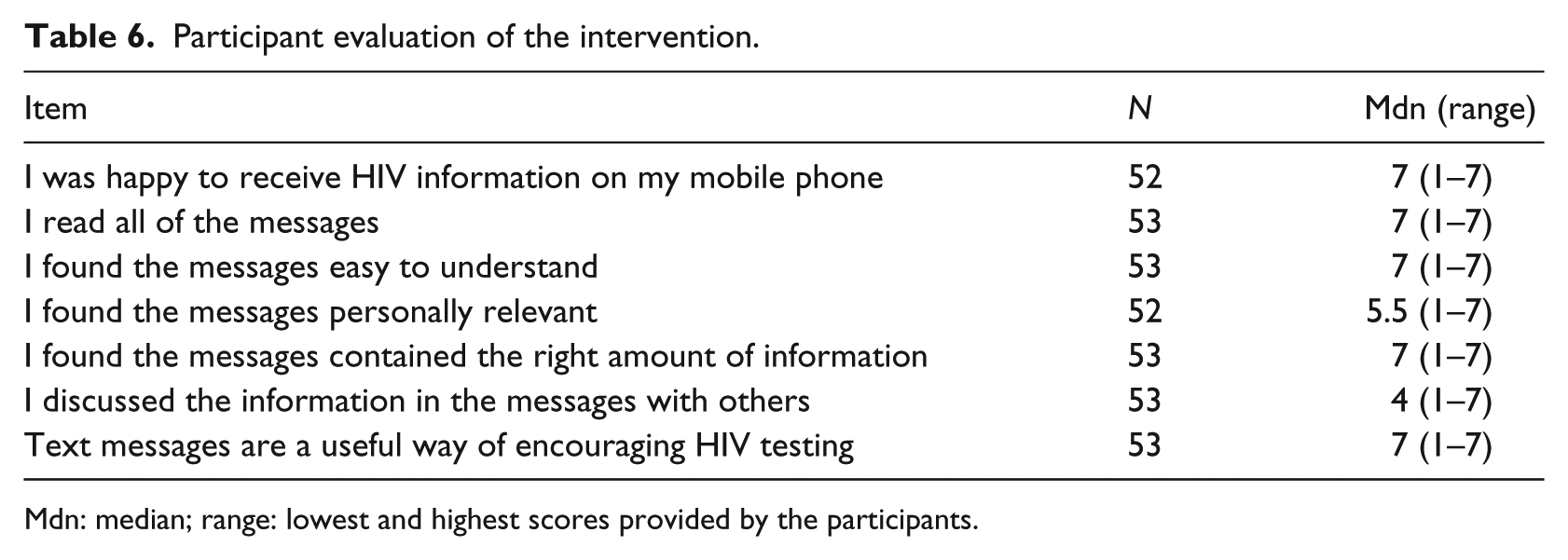
Mdn: median; range: lowest and highest scores provided by the participants.
Discussion
Effectiveness of recruitment strategies
Recruitment was successful in terms of participant numbers. A total of 172 participants were recruited, which exceeded the original recruitment target of 120. Community researchers provided a feasible and appropriate means of supporting recruitment into HIV-related SMS interventions. Given the low refusal rate, the intervention was acceptable to the target communities, confirming our hypothesis that mobile phones are an appropriate channel for reaching this population with health messaging.
Acceptability of data collection methods
Data collection using online, text and email methods was not feasible in this population group. Face-to-face interactions or telephone follow-up were more successful. Recent UK national surveys of HIV in African communities that attempted to use online methods of data collection have reported similar challenges (Bourne et al., 2014; Public Health England, 2015).
Influence on HIV testing and response rate
Follow-up data were obtained for only 76 out of 169 individuals (45%). Of these, eight (10.5%) reported having an HIV test during or after the intervention. This relatively low response rate and the small numbers in the follow-up sample make these findings difficult to interpret. However, mobile phone interventions are low cost. The cost saving for any new HIV case detected in the UK has been estimated at £380,000 (US$493,582) (Nakagawa et al., 2015), suggesting that even marginally increasing the potential for identification of new cases through increasing access to testing has potential for significant economic benefit.
There is relatively little outcome data available for SMS-based interventions against which to compare our study findings. In South Africa, a multi-arm SMS intervention study recruited from a mobile phone company’s database (n = 2,533) achieved a 54.1% response rate for the primary outcome. Of these, 30.2% reported having an HIV test and 22.3% reported that they did not (De Tolly et al., 2012). This relatively higher response rate may have been influenced by the fact that participants who responded received a 10-Rand mobile phone top-up.
With respect to other (non-SMS) community-based HIV testing interventions among African migrants in the UK, we are aware of only one initiative (offering outreach ‘point of care’ tests) that has published process and outcome data (Rayment et al., 2012). In total, 3,789 African individuals were approached, of whom only 459 (12.1%) agreed to be tested – a relatively low proportion, as found in our study.
Intervention targeting and reach
With respect to HIV, the proportion of our sample who reported ever having had a test (62%) is comparable with national surveys conducted in 2008 and 2014 in the UK which reported figures of 61.9% and 65%, respectively, among African communities (Bourne et al., 2014; Sigma Research, 2009). For pragmatic reasons, our survey did not elicit information on risk behaviours; hence, it is difficult to assess whether the intervention was able to reach those most at risk; nonetheless, over 50% could be potentially deemed to be eligible for testing (24.2% had tested more than a year ago and 30.8% had never tested). A systematic review of 45 community HIV testing interventions in resource-rich countries concluded that ‘the large majority of clients (between 62%–100%) had previously had an HIV test’ (Thornton et al., 2012: 421). These findings, as well as ours, suggest that more work needs to be done in order to understand who interventions are targeting and whether or not the most vulnerable are being reached.
In terms of socio-demographic characteristics, the composition of the study sample (including HIV testing history) was strongly comparable to participants in the aforementioned UK national surveys among African communities (Bourne et al., 2014; Sigma Research, 2009).
No one declined research participation on the grounds of not having a phone, confirming that mobile phone use is high among African community members (Ofcom, 2013). Slightly more men (n = 85) than women (n = 67) participated in the study, and the majority of participants were university educated (79%); however, we were unable to examine the reasons for potential differences in uptake. Although the intervention was available in three languages, the majority (89.3%) chose English. This is perhaps because proficiency in English was required to consent and take the baseline survey. Overall, our results suggest that mobile phone–based health education approaches have good potential to reach widely into African migrant communities across different demographics, but future research should examine variations in uptake and use in more depth, particularly in relation to gender, education and language.
Influence on HIV-testing determinants
The intervention had a positive influence on some aspects of HIV-related knowledge and awareness, including a small but significant improvement in participants’ knowledge about where to get help and support around HIV and testing, and perceptions of the ease and accessibility of HIV testing. This suggests that some of the messages may have helped to clarify issues that may motivate or prevent individuals from accessing testing. It is unclear why no significant changes to perceived susceptibility (risk) was found but may be related to the fact that HIV remains a stigmatised condition in which a risk discourse is often externalised (i.e. considered a disease of ‘others’) and where fear of social consequences acts as a barrier to testing (Blondell et al., 2015).
Influence on general health status, quality of life and other health behaviours
High levels of general health and quality of life were reported both before and after the intervention. Still, one-quarter to one-third of participants reported a positive trend in a range of health domains. Health behaviours often cluster together and it may be that consideration of one area of health led to increased attention being paid to several aspects of health (Buck and Frosini, 2012). Hence, these findings indicate the potential to use SMS messaging to promote other aspects of health in UK African communities.
Study limitations
Formative research we had earlier conducted highlighted the importance of providing the intervention in three languages: English, French and Arabic (Evans et al., 2016). Yet, the majority of participants (89.3%) requested to receive the messages in English. This may be due to the eligibility requirement of English proficiency for consent and baseline survey completion. Hence, to reach non-English-speaking African migrants in the UK, Arabic and French may need to be used in all study components.
There was a poor response rate to online or text-based method at follow-up which hampered the measurement of intervention effects. Follow-up data were collected within a relatively short time after intervention. Furthermore, in an effort to keep the survey short, a limited number of items and several single-item measures were used.
While the feasibility objectives were met by this study design, the effectiveness of the intervention in changing testing behaviour, health and quality of life outcomes needs to be tested in a well-designed randomised controlled trial with longer follow-up periods.
Conclusion
This study demonstrates the potential health benefits of mobile phone–based interventions for African migrant communities in two respects. First, it showed that an SMS intervention designed to prompt HIV testing behaviour is feasible and well accepted by the target communities. While demonstrating impact on HIV testing with a single group study was not possible, clear improvements in HIV testing determinants, attitudes towards HIV and testing, and indication of potential for improvement in other health behaviours were shown. Findings lend support to the study’s strategy of incorporating HIV testing messages among other general health messages. Second, the study findings indicate that mobile phone–based interventions may be an acceptable and wide-reaching mechanism for health promotion more generally among African migrant communities. When co-constructed with communities, SMS initiatives may thus help to overcome some of the health-related barriers faced by migrant populations in new countries. Future research and service development should focus on evaluating this potential in relation to other key health priorities.
Footnotes
Acknowledgements
The authors would like to sincerely thank all the study participants and the AISD community research team.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nottingham City Public Health Department provided funding for the study.