
Abstract
Objective:
In this systematic review and meta-analysis, we aimed to quantify the effects of text messaging interventions to reduce depressive symptoms and identify variables that might influence the effectiveness of the intervention.
Design:
Electronic databases including EMBASE, CENTRAL, MEDLINE, CINAHL, PsycINFO and SCOPUS, as well as Clinicaltrials.gov and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) were searched for randomised controlled trials that sent one or more text messages with health-related content to adults who had been identified by a healthcare provider.
Results:
Seven trials (nine comparisons), with 1,918 participants, were included in the review, and the pooled analysis revealed a borderline statistically significant reduction in depressive symptom scores between the text messaging intervention and control groups (standardised mean difference [SMD], −0.27; 95% confidence interval [CI], −0.54 to 0.00; p = .00) favouring intervention at the end. Statistically significant reductions were shown in important subgroups, for example, where the primary aim of the messages was to reduce depressive symptoms; in those using the Beck Depression Inventory (BDI) or 9-item Patient Health Questionnaire (PHQ-9) questionnaires; where text message content was targeted at mental well-being, mood improvement and cognitive behavioural therapy information; and when the message frequency was ⩾2 times per week.
Conclusion:
Text messaging has potential to reduce depressive symptoms. The results of this review should be interpreted with caution, however, due to the methodological limitations of included trials. More research is required before recommendations can be made about the routine use of text messaging for the management of depressive symptoms.
Introduction
Depression can vary in aetiology, presentation and duration. However, common symptoms include sadness, irritability or emptiness, with somatic or cognitive changes that disrupt functioning (American Psychiatric Association, 2018). Depression affects 322 million people globally, and depressive disorders are now the largest contributor to non-fatal health loss, accounting for more than 50 million Years Lived with Disability (World Health Organization [WHO], 2017).
Global estimates suggest up to two-thirds of people suffering from a mental health disorder never seek treatment from a health professional (WHO, 2001). This may be partially explained by the lack of safe, effective, low-cost treatments for depressive symptoms in many countries. The primary treatments, psychological therapy and pharmacotherapy, can be resource-intensive, costly and have side effects (Allida et al., 2020). In high-income countries where treatments are more readily available, the relatively low rates of seeking treatment (46%) are likely caused in part by the stigma associated with having a diagnosis and seeking or requiring treatment (The Black Dog Institute, 2015). Stigma is also a barrier in lower resource countries where the highest burden of mental illness lies, compounded by a lack of funding and workforce shortages preventing many from accessing treatment (Bruckner et al., 2011). Confounding these barriers is the intrinsic nature of depressive symptoms which may include a lack of motivation to seek treatment or comply with lengthy courses of drugs or therapy.
In the last 20 years, mobile phones have almost universally integrated into daily life. To date, there are 7 billion people who live in an area covered by a mobile telephone network (Sood et al., 2016). Ninety percent of adults own a mobile phone in the USA (Hughes and Granger, 2014). Mobile phone ownership in low- and middle-income countries has increased exponentially, faster than any other health, transport or communication infrastructure (Abaza and Marschollek, 2017), positioning mobile phones as accessible devices, quite literally at our fingertips, that offer a highly adaptable (personalisation, frequency, content) communication channel between healthcare professionals and consumers.
Community attitudes to health-related mobile phone–delivered interventions have been positive regardless of sex, education level or employment status of participants, including those with symptoms of anxiety or depression. Perceived benefits include convenience and the potential to reduce isolation (Proudfoot et al., 2010). Qualitative interviews with HIV-positive participants in an antiretroviral adherence text messaging intervention revealed they derived greater emotional meaning from simple reminder messages, for example, recurring themes of feeling ‘cared about’ and ‘seen’ providing a theoretical mechanism of action (Ware et al., 2016). Pearson et al. found mobile phone ownership (after adjustments for wealth and education) increased mental well-being among rural Ugandans, suggesting that mobile phone interventions that increase social connectedness may also have value in mental health treatment in lower resource countries, remote locations and isolated communities, where such approaches may be more applicable. Other potential mechanisms of text message intervention efficacy (Dallery et al., 2015) include altering normative beliefs, promoting acceptance of feelings, changing awareness, and increasing knowledge and motivation.
In this systematic review and meta-analysis, we aim to summarise the evidence and quantify the effects of using text messaging as an intervention to reduce depressive symptoms for people presenting to healthcare professionals. We also seek to identify what variables (content, frequency and personalisation) may influence the effectiveness of text messaging as a health intervention for reducing symptoms of depression.
Methods
The full systematic review protocol was registered prospectively in PROSPERO: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=110027
Types of included trials
Randomised controlled trials (RCTs).
Types of participants
We included trials of adults aged ⩾18 years. Participants were identified for the trial by a healthcare provider so as to minimise volunteer bias. No exclusions were made on the basis of any reported medical condition among the participants.
Types of interventions
Text messaging interventions were defined as one or more text messages with health-related content sent to a personal mobile device. The comparator had to be usual care or an attention control (a small amount of interpersonal interaction without the main intervention). One-way (reply not permissible or participants’ informed system was one way) and two-way text messaging trials were included; however, trials of smartphone applications were excluded.
Types of outcome measures
The primary outcome was depressive symptoms (mean depression scores) measured using a validated questionnaire at the end of the intervention. Secondary outcomes included depression present/absent: proportion of people not meeting the authors’ criteria for depression (not depressed) and adverse events if recorded and reported.
Search methods for identification of trials
A search strategy was designed with a librarian using terms including (but not limited to) ‘depress’ OR ‘depression’ AND ‘SMS’ OR ‘text message’ OR ‘short message service’. Electronic databases including EMBASE, CENTRAL, MEDLINE, CINAHL, PsycINFO and SCOPUS were searched from 1992 to 18 September 2018. Other sources such as clinicaltrials.gov and WHO International Clinical Trials Registry Platform (ICTRP) registries were also searched. We sought to include all trials since the inception of text messaging (1992). No language restrictions were imposed. The reference lists of relevant trials and reviews were also screened, and further trials were identified for assessment.
Study selection, data extraction and management
The titles and abstracts identified through the search were screened by two independent reviewers (K.L.C. and S.M.A.) for eligibility for inclusion. Any disagreements were resolved by a third reviewer (M.L.H.). Eligible trials were assessed, and the following data were extracted for included trials using a standardised data extraction form:
Publication details: authors, year and source;
Sample characteristics: socio-demographics, descriptions of text messages, usual care and depression criteria, country and attrition;
Participants: age, sex/gender, ethnicity, history of depression, co-morbidities, and prior and current treatments for depression;
Trial design: randomisation method, sampling mechanism, adherence, follow-up length and trial setting;
Intervention features: type and content of messages, frequency, timing, duration and total number of messages sent;
Effect size: sample size, estimate, standard error and power;
Measurement tools: outcome scales or measurements;
Comparison group details;
Outcome: depression present/absent and mean depression scores at the end of treatment (and follow-up data if available) and adverse events (if recorded and reported).
Trials that met all the inclusion criteria with no available outcome data (from the trial report or the authors) could not contribute meaningfully to a pooled estimate of effect. These were regarded as ‘dropouts’ rather than ineligible, to indicate that they have not been overlooked. Trials with insufficient information to assess whether they met our inclusion criteria were labelled as ‘awaiting assessment’, and the authors were contacted for further information. Any trials that met our criteria but had not been completed were regarded as ‘ongoing’.
Risk of bias and GRADE assessments
Risk of bias was assessed by two independent reviewers (K.L.C. and S.M.A.) using the Cochrane risk of bias tool for RCTs (Higgins et al., 2019). A judgement of low, high or unclear risk was allocated based on the domains of random sequence generation, allocation concealment, selective reporting, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data and any other potential sources of bias such as unbalanced variables at baseline. Any disagreement between judgements was discussed and referred to a third reviewer (M.L.H.).
The quality of evidence was assessed and adjusted using the five GRADE considerations: trial limitations, consistency of effect, indirectness, imprecision and publication bias (Brożek et al., 2009). An overall rating was given to reflect the level of confidence we have in the strength of evidence collated in this review.
Statistical analysis
Trial results were pooled and analysed using Stata 16 software (StataCorp, StataCorp LLC, 2019). The pooled reduction in depressive symptoms was calculated using the random-effects approach (DerSimonian and Kacker, 2007). The standardised mean difference (SMD) was calculated for continuous end points as different outcome measures were used. Trials with three arms were included as two separate trials with the numbers in the intervention group compared with half the number in the control group. Heterogeneity of the estimates between trial populations was calculated using I2 statistics. Inconsistency in results was categorised as low (I2 = 0–29), moderate (I2 = 30–49), substantial (I2 = 50–89) and considerable (I2 = 90–100) (Higgins et al., 2003). Subgroups included analysis by depression questionnaire used, and content and frequency of messages. A sensitivity analysis was run for all trials with depression (yes/no) as the primary outcome and for trials that assessed depression symptoms using validated rating scales.
Results
Results of the search
We screened 3,762 titles and abstracts and excluded 3,704 irrelevant records. We retrieved 58 articles for full-text review. After reading the full texts, the primary reasons for excluding 32 studies were the interventions being mHealth smartphone apps, Internet-based or part of a package of intervention which included text messages as an adjunct to other components rather than the primary intervention being tested (see Figure 1).
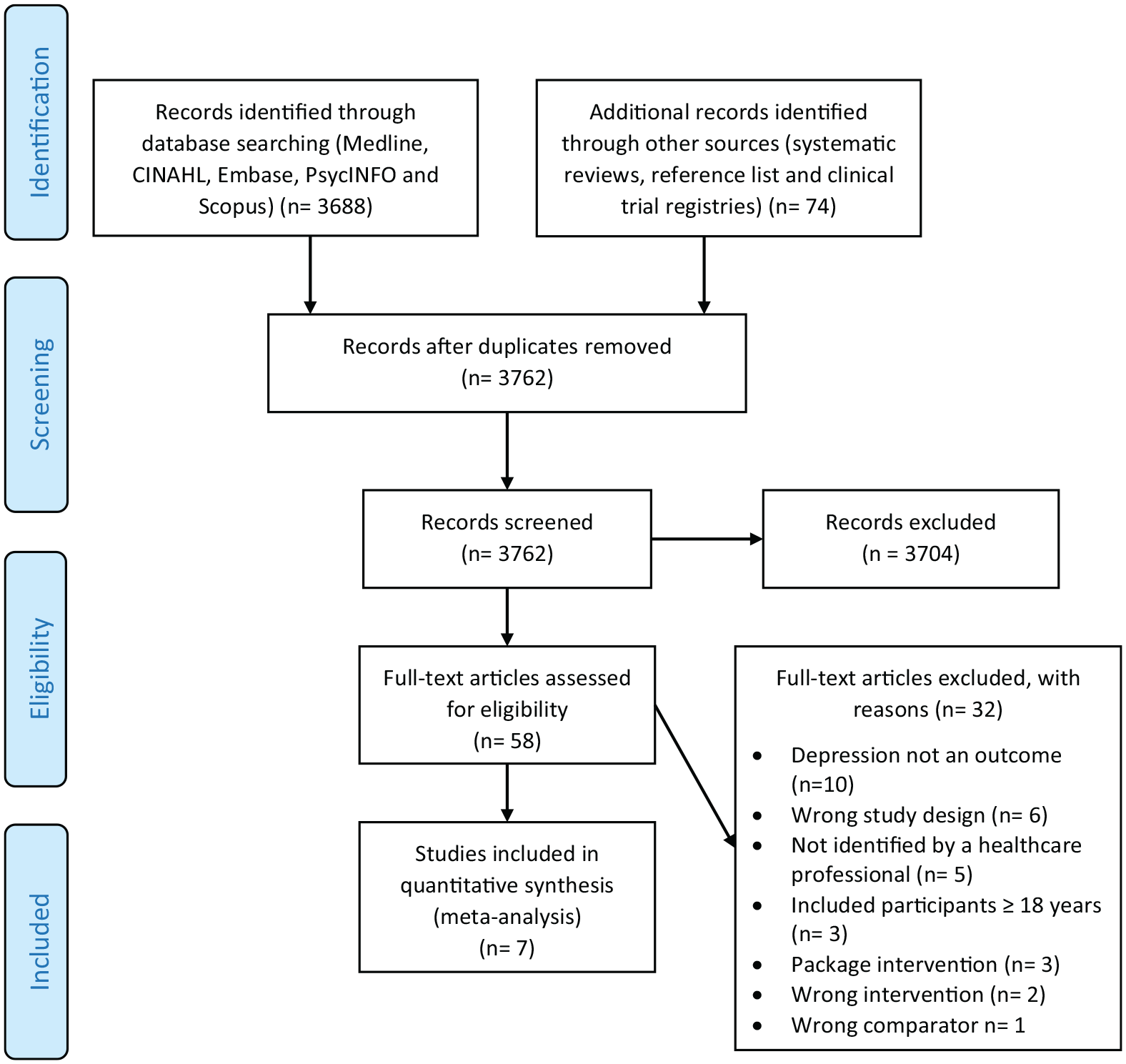
PRISMA flow diagram.
We included seven trials (nine comparisons, n = 1,918 participants). Suffoletto et al. (2013) and Schlicker et al. (2018) were parallel, three-armed RCTs (see Table 1 for characteristics of the included trials).
Characteristics of the trials included in text messaging interventions for reducing symptoms of depression review.
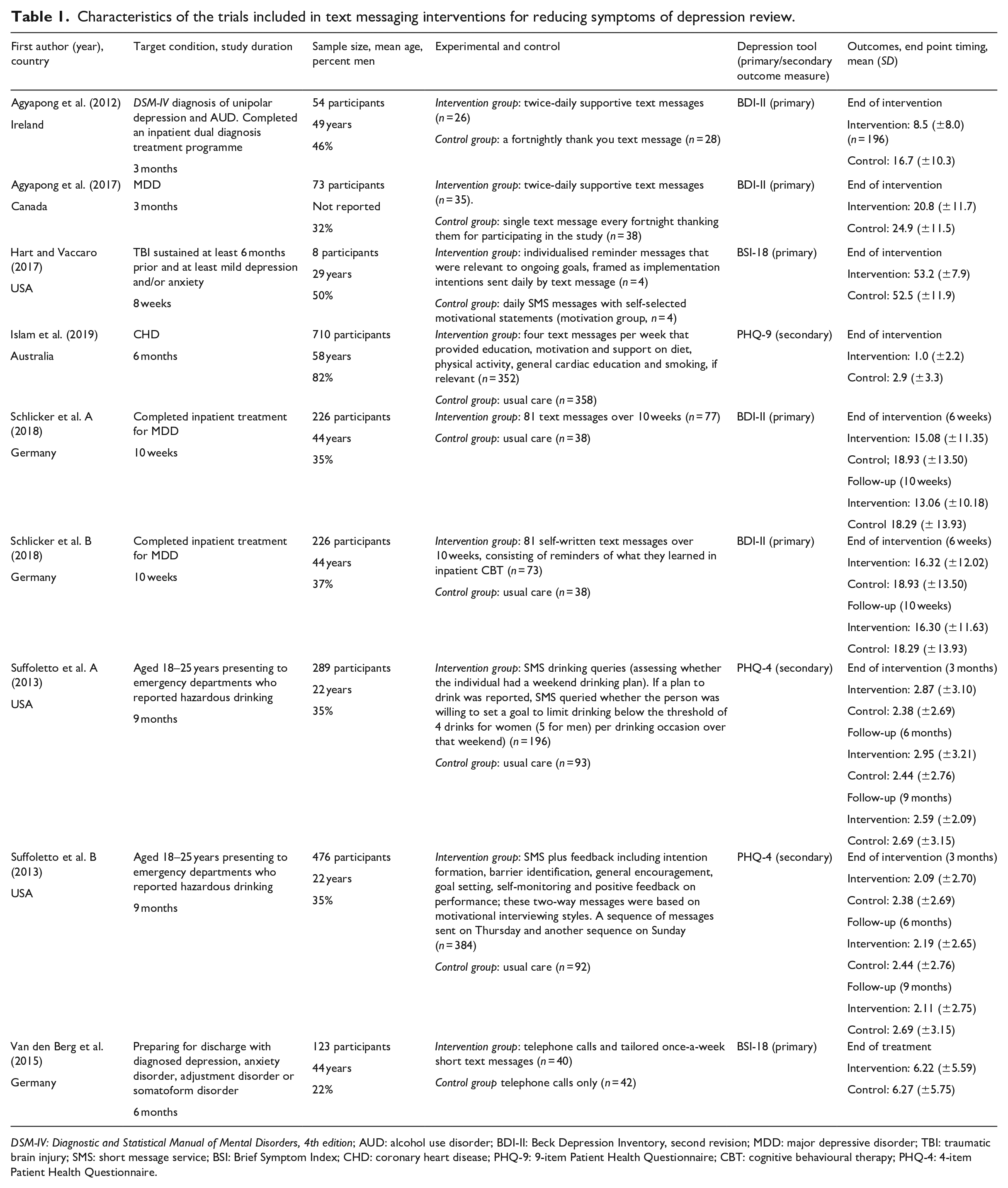
DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, 4th edition; AUD: alcohol use disorder; BDI-II: Beck Depression Inventory, second revision; MDD: major depressive disorder; TBI: traumatic brain injury; SMS: short message service; BSI: Brief Symptom Index; CHD: coronary heart disease; PHQ-9: 9-item Patient Health Questionnaire; CBT: cognitive behavioural therapy; PHQ-4: 4-item Patient Health Questionnaire.
Eight trials were ongoing at the time of the review (Berrouiguet et al., 2014; Chow et al., 2018; Clark et al., 2018; Hartnett et al., 2017; Husain, 2015; Jiskoot et al., 2017; McCarter et al., 2018; Tandon, 2018) and eight awaiting classification (Ben-Zeev, 2017; Boeschoten et al., 2012; Fletcher et al., 2018; Haas et al., 2017; Moore et al., 2015; Ohora, 2016; Schueller, 2018; Taleban et al., 2016). These study authors were contacted to clarify the recruitment methods. Three trials were considered ‘dropouts’, two studies did not report depression scores at the end of the intervention and one study did not report results by allocation arm (Pijnenborg et al., 2010; Spoelstra et al., 2016; Wolf et al., 2016).
Participants
Five trials (six comparisons) recruited participants prior to discharge from hospital and one trial recruited from community mental health clinics. Four trials (five comparisons) required participants to have depression at entry (Agyapong et al., 2012, 2017; Hart and Vaccaro, 2017; Schlicker et al., 2018). Participants in two of the trials (three comparisons) had received an inpatient treatment programme consisting of psychotherapy prior to recruitment in the trial (Agyapong et al., 2012; Schlicker et al., 2018). In one trial, people with a variety of diagnosed mood disorders (e.g. depression and anxiety) were included (van den Berg et al., 2015). The conditions of interest in other trials were coronary heart disease (Islam et al., 2019) and hazardous drinking (Suffoletto et al., 2013). Participants’ mean age ranged from 22 to 58 years, and the ratio of women to men was unbalanced in all but two trials (Agyapong et al., 2012; Hart and Vaccaro, 2017). The trials were conducted in the USA (2), Germany (2), Ireland (1), Canada (1) and Australia (1).
Interventions and comparators
Two comparisons sent one message a week (Suffoletto et al., 2013; van den Berg et al., 2015), whereas the other seven comparisons sent two or more. Six interventions had depression as the primary outcome (Agyapong et al., 2012, 2017; Hart and Vaccaro, 2017; Schlicker et al., 2018; Suffoletto et al., 2013; van den Berg et al., 2015). Five interventions had usual care as the comparator (Islam et al., 2019; Schlicker et al., 2018; Suffoletto et al., 2013). Two trials sent fortnightly thank you messages as the attention control (Agyapong et al., 2012, 2017). One trial administered telephone calls to both groups and also sent tailored SMS messages to the intervention group with therapy themes (van den Berg et al., 2015). Four comparisons had mental health content in the messages (Agyapong et al., 2012, 2017; Schlicker et al., 2018).
Suffoletto et al. had two intervention groups: group A received a weekly text message about alcohol drinking intentions and group B participated in two-way messaging, both compared with usual care (Suffoletto et al., 2013). Schlicker et al. group A received standard messages and group B received personalised self-written text message reminders from inpatient cognitive behavioural therapy (CBT) work, both compared with usual care (Schlicker et al., 2018).
Risk of bias assessment
A graphical summary of risk of bias assessments as determined by review authors for the included trials is provided in Figure 2.

Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
Allocation
One trial used a systematic method of allocation (alternating week by week) and was assessed as high risk of bias (Schlicker et al., 2018). Two studies did not describe their method of randomisation and therefore were judged as unclear risk (Hart and Vaccaro, 2017; van den Berg et al., 2015). Only one study gave sufficient detail of its allocation concealment and was rated low risk of bias (Islam et al., 2019). Risk of bias for the remaining trials was unclear.
Blinding
Blinding of participants was not possible due to the nature of the intervention; therefore, all studies received a high risk of bias judgement for performance bias. One study blinded the outcome assessors; however, it reported that the blinding was broken in many instances by the participants divulging their allocation group; thus, it was rated as high risk of detection bias (Agyapong et al., 2012). One study had a self-reported outcome which was rated as high risk due to potential detection bias (Suffoletto et al., 2013). Two studies did not report blinding of outcome assessment and therefore received an unclear assessment (Schlicker et al., 2018; van den Berg et al., 2015)
Incomplete outcome data
Three trials conducted per-protocol analysis (where only the participants who completed the study are included in the results), potentially leading to bias (Islam et al., 2019; Suffoletto et al., 2013; van den Berg et al., 2015). One trial had high attrition across the groups (19.4% in group A, 24.6% in group B and 22.3% in the control group), with the number of imputed values potentially contributing to measurement bias (Schlicker et al., 2018). All were rated as at high risk for incomplete outcome data.
Selective reporting
The frequency of medical contact and acceptability of the intervention were mentioned in one trial’s protocol; however, neither outcome was reported in the publication; as such, a high risk of bias was awarded for reporting bias (van den Berg et al., 2015). Only one other trial had a published protocol (Islam et al., 2019); as such, all others were awarded unclear risk.
Other bias
There were concerns regarding other sources of bias in six studies due to unbalanced variables at baseline (Agyapong et al., 2017; Hart and Vaccaro, 2017; Islam et al., 2019; Schlicker et al., 2018; Suffoletto et al., 2013; van den Berg et al., 2015).
Outcomes
Primary outcome
The pooled analysis of seven trials (nine comparisons) (Figure 3) revealed a borderline statistically significant reduction in depressive symptom scores between the text messaging intervention and control groups (SMD, −0.27; 95% confidence interval [CI], −0.54 to 0.00; p = .00; n = 1,918 participants) at the end of treatment. Substantial heterogeneity was observed (I2 = 83%).

Forest plot of comparison: text messages vs control; outcome, depression: mean scores at the end of treatment.
Secondary outcomes
Only one trial reported the presence (defined as a 9-item Patient Health Questionnaire [PHQ-9] score of 5–27) and absence of depression at the end of treatment (Islam et al., 2019). There was a significant difference (p < .001) in the proportions with depression in the intervention (6.3%) and control (24.6%) groups at 6 months (end of treatment). No trials reported adverse events.
Subgroup analysis
Content of the messages
The subgroup analysis of the three trials (four comparisons) with messages that contained a mental health component demonstrated a statistically significant reduction in depression symptom scores compared with the control group (SMD, −0.39; 95% CI, −0.64 to −0.14; n = 353 participants; I2 = 24%). The four trials (five comparisons) without a mental health component in their text messaging intervention found no reduction in depression symptom scores in comparison with controls (SMD, −0.15; 95% CI, −0.57 to 0.27; n = 1,515 participants; I2 = 90%). Considerable heterogeneity observed may be due to variations in the intervention and population groups enrolled in the latter trials (Figure 4).
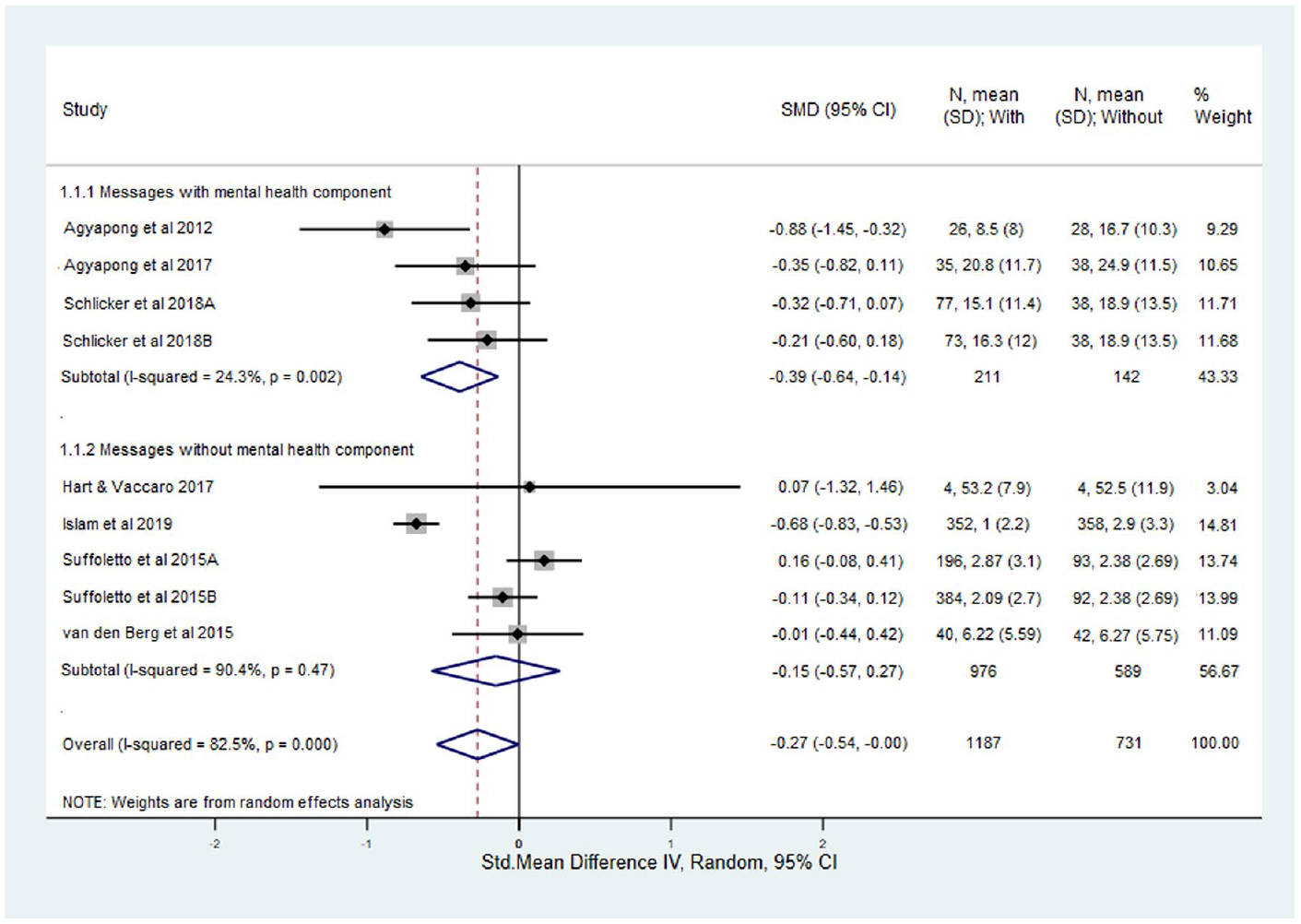
Forest plot of comparison: text messages vs control, content of the messages; outcome, depression: mean scores at the end of treatment.
Frequency of the messages
The subgroup analysis of seven comparisons where ⩾2 messages were sent per week showed a statistically significant reduction in depressive symptoms (SMD, −0.39; 95% CI, −0.65 to −0.13; n = 1,409 participants; I2 = 73%). The two comparisons that delivered <2 messages per week showed no statistically significant difference (SMD, 0.12; 95% CI, −0.09 to 0.34; n = 459 participants) (Figure 5).
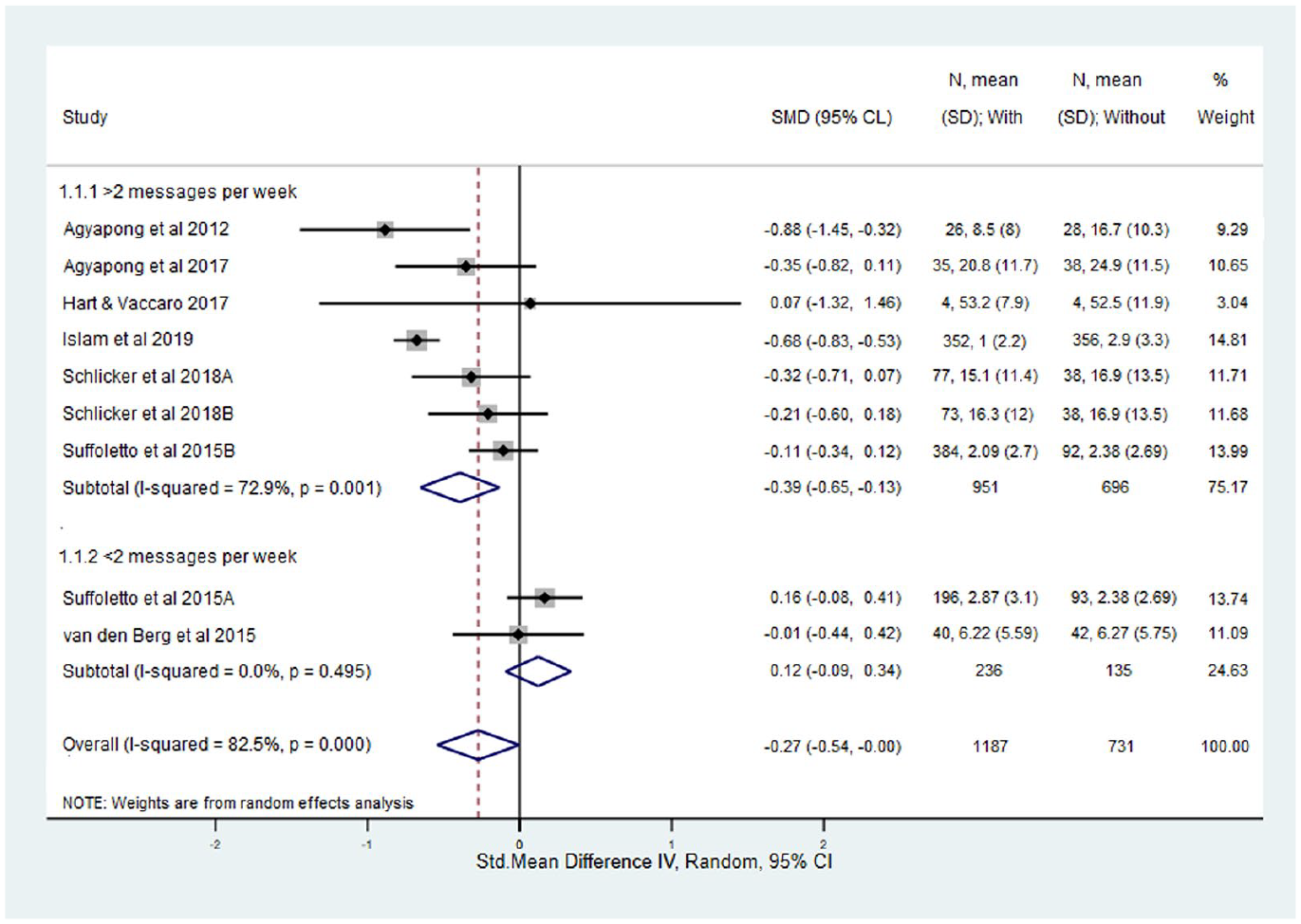
Forest plot of comparison: text messages vs control, frequency of messages; outcome, depression: mean scores at the end of treatment.
Sensitivity analysis – trials with depression as the primary outcome
Sensitivity analysis was performed using five trials (six comparisons) with depression as the primary outcome (Agyapong et al., 2012, 2017; Hart and Vaccaro, 2017; Schlicker et al., 2018; van den Berg et al., 2015). A statistically significant reduction in mean depression symptom scores was found in the intervention group compared with the control group (SMD, −0.30; 95% CI, −0.53 to −0.08; n = 439 participants) at the end of treatment. There was low heterogeneity (I2 = 23%) but very wide CIs (Figure 6).
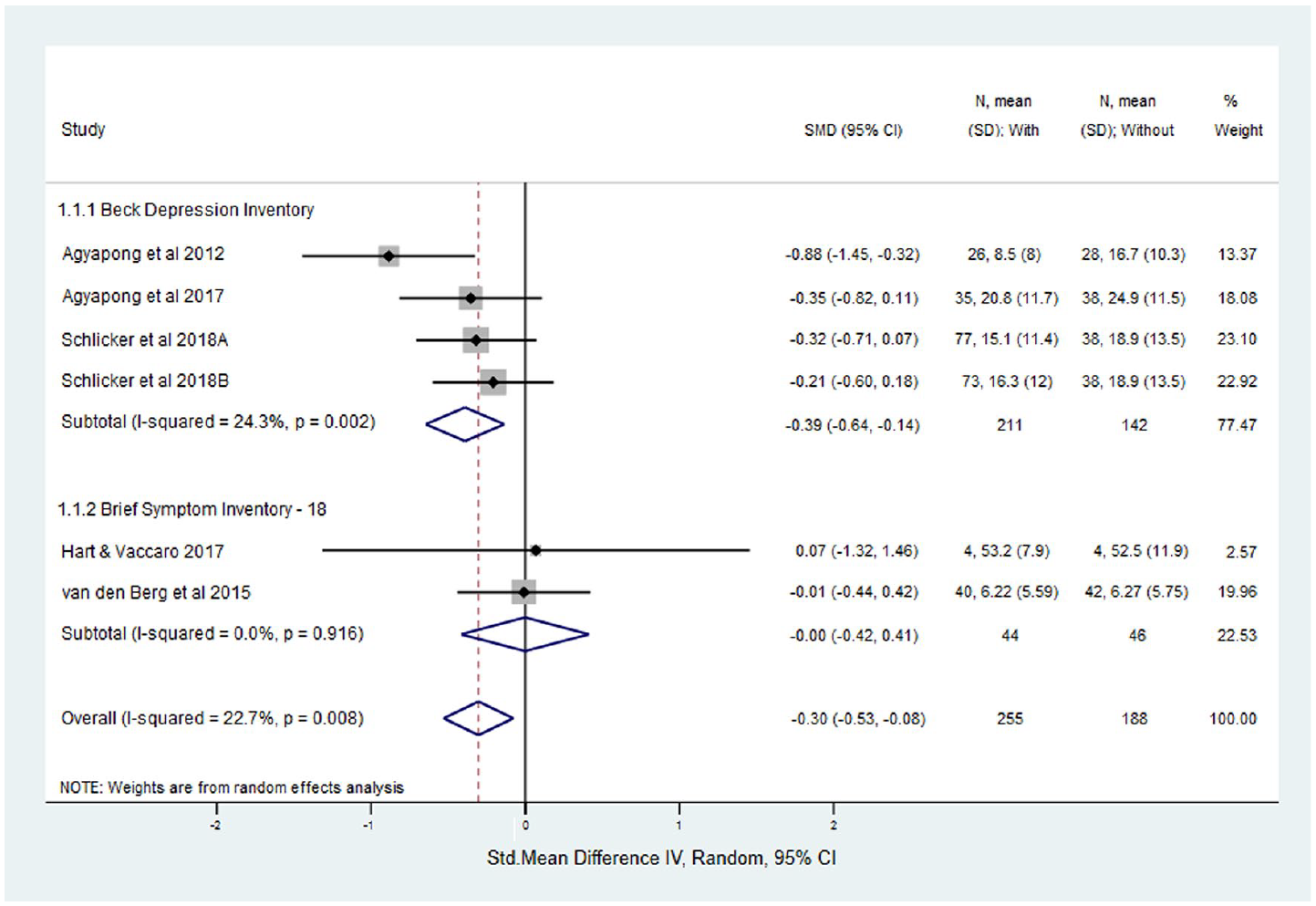
Forest plot of comparison: text messages vs control, studies with depression as the primary outcome; outcome, depression: mean scores at the end of treatment.
Sensitivity analysis – trials using standard depression rating scales
Sensitivity analysis was performed in the four comparisons using the Beck Depression Inventory (BDI) (Agyapong et al., 2012, 2017; Beck et al., 1961; Schlicker et al., 2018), and statistically significant lower depressive symptom scores were found in those in the text messaging intervention group compared with control (SMD, −0.39; 95% CI, −0.64 to −0.14; n = 353 participants) at the end of treatment. There was low heterogeneity (I2 = 24%) but wide CIs.
The pooled result of the four comparisons using the BDI (Agyapong et al., 2012, 2017; Beck et al., 1961; Schlicker et al., 2018) combined with one trial that used the PHQ-9 (Islam et al., 2019; Kroenke et al., 2001) was statistically significant for lowering symptoms of depression (SMD, −0.49; 95% CI, −0.73 to −0.26; n = 1,063 participants; p < .0001), favouring text messaging over control (Figure 7).
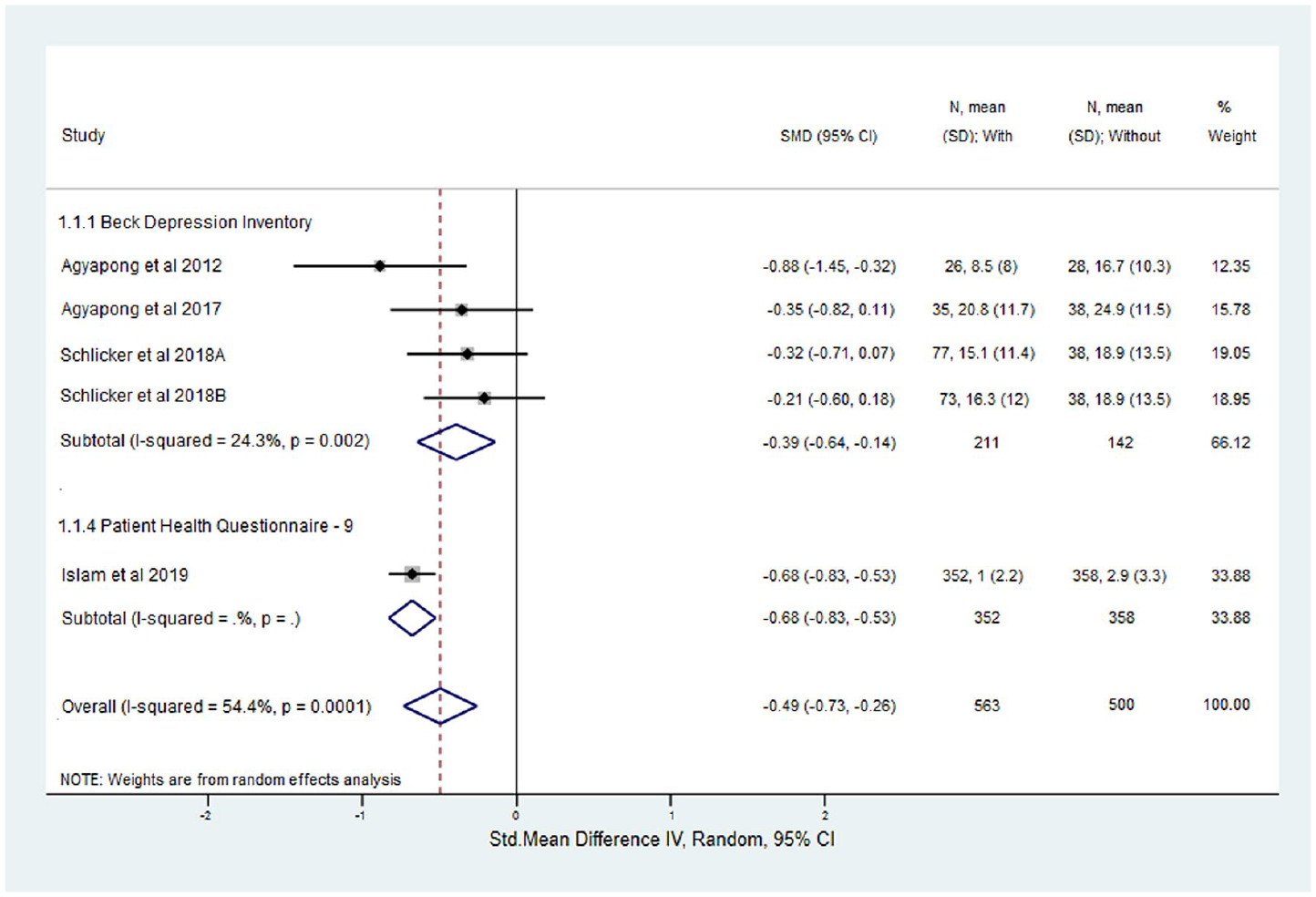
Forest plot of comparison: text messages vs control, studies with standard depression rating scales; outcome, depression: mean scores at the end of treatment.
Summary of findings
The overall rating of the quality of evidence of the effectiveness of text messaging was very low, as presented in the Summary of Findings (Table 2). The evidence from the trials was downgraded in quality due to a high risk of selection and performance bias, heterogeneity and very wide CIs. We did not assess publication bias due to the small number of included trials (Brożek et al., 2009).
Summary of findings table.

CI: confidence interval; SMD: standardised mean difference; RCT: randomised controlled trial.
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
Explanations:
We downgraded the quality of evidence as the studies were rated as high risk for multiple risk of bias domains.
We downgraded the quality of evidence as there is considerable heterogeneity (I = 75%–100%) observed.
We downgraded the quality of evidence as the CIs were wide.
We downgraded the quality of evidence as the CIs were very wide.
We downgraded the quality of evidence as there are only two studies with <100 participants contributing to the analysis.
Discussion
Text messages are often included in health research as part of an intervention package. This review assessed text messaging as a standalone intervention to reduce depressive symptoms. It is useful to understand the value of the individual components of an intervention package for optimum programme design, and this information will be of particular importance in lower resource settings where funding for complex packages of care may not be available.
Data from seven trials (nine comparisons, n = 1,918 participants) showed text messages on their own were not associated with a reduction in depressive symptom scores at the end of the intervention. However, statistically significant reductions in depressive symptoms were shown in important subgroups specified a priori, for example, where the primary aim of the messages was to reduce depressive symptoms; in those using the BDI (Agyapong et al., 2012, 2017; Schlicker et al., 2018) or PHQ-9 scales (Islam et al., 2019; Kroenke et al., 2001); where text message content was targeted at mental well-being, mood improvement and CBT information; and when the message frequency was ⩾2 times per week. We found no data on the long-term effects of text messaging interventions or the length of time required to show maximal or sustained response to the receipt of text messages.
Due to the paucity of trials assessing text messaging as a standalone intervention, we also included trials that used other mood rating scales to measure depressive symptoms such as the Brief Symptom Index (BSI)-18 (Derogatis, 1993) and 4-item Patient Health Questionnaire (PHQ-4) (Kroenke et al., 2009). The BSI-18 tool (Derogatis, 1993) is a general mood rating scale that measures psychological distress broadly with only six questions focused on depression, while the PHQ-4 (Kroenke et al., 2009) is a brief screening tool with two questions on depression and two on anxiety. While we acknowledge that the use of different scales makes comparisons across trials difficult, the sensitivity analysis showed significant results in trials using the BDI or PHQ-9. Thus, we recommend future trials use depression-specific scales when measuring depressive symptoms.
Any indication of benefit must be considered alongside methodological limitations in the included trials, for example, short duration of the text messaging intervention (from 6 weeks to 6 months), variation in the types of trial participants, the content and frequency of the text messages, and the inadequate reporting of methods in many of the included trials (particularly in the domain of allocation concealment). The overall quality of the evidence was rated as very low due to these limitations and considerable heterogeneity (I2 = 80%) within and between the trials.
A recently published systematic review evaluating the effectiveness of text messaging found marginal evidence to support its use as a treatment modality for people with clinical depression (SMD, −0.27; 95% CI, −0.48 to 0.02; p < 0.07; seven trials, n = 845 participants) (Senanayake et al., 2019). In contrast to our review which included adults (⩾18 years) regardless of their baseline depression score, that review included adolescents (⩾13 years) diagnosed with depression at baseline (with any accepted tool). In addition, while our review was registered prospectively in PROSPERO, their review was retrospectively registered: https://www.crd.york.ac.uk/PROSPERO/RecordID=141100. Most importantly, our review performed sensitivity and subgroup analyses to identify factors in the design of the text messaging interventions that might influence the reduction of depressive symptoms. A review of systematic reviews into text messaging for health (no mental health trials were included) supported the integration of text messaging into public health practice; however, it was unable to recommend optimum intervention characteristics or comment on long-term effects and called for further research into potential risks and unintended consequences (Hall et al., 2015).
One theory for a potential mechanism of action is the impression of ‘connection’ between the sender and the recipient of the messages. Social isolation or lack of connectedness, participation and infrequent social contact have been linked to poorer mental health and are predictors of increased risk of mortality, compared with less socially isolated individuals (Pantell et al., 2013). The feeling of connection established during a text messaging intervention may help reduce social isolation. Based on our findings, a minimum threshold for the frequency of messages is indicative of 2 or more per week.
The stigma associated with mental illness is also a barrier to treatment access for many people. Although not explored in the included studies, anonymity and confidentiality of text messaging interventions are positive characteristics reported in the area of sexual health where stigma is also often a barrier to care (Willoughby and L’Engle, 2015). Qualitative research focusing on the experiences and perceptions of text messaging programmes would further add to the evidence base.
In addition, the smaller group of trials where the primary focus was to reduce depressive symptoms showed benefit. This points to the importance of close alignment between messages received and the outcome being targeted. However, it is important to note that in two trials, participants had undergone an inpatient treatment programme which involved psychotherapy before commencing the text messaging intervention. Thus, the reduction in depressive symptoms may be the result of the combined effect, including reinforced learning from the therapy received during the inpatient treatment programme.
While we acknowledge that text messaging is not a suitable substitute for mental health service support, it has the potential to augment the current gold standard of care. It is a practical and cost-effective approach, one that is able to reach remote locations and isolated communities. Furthermore, it has the potential to be used in low-income countries as a standalone intervention to reduce symptoms of depression as complex packages of interventions come at a higher cost per capita which may be prohibitive in some settings (Hall et al., 2015).
It is important to note that most of the trials were conducted in high-income countries, and text messaging applicability and acceptability in lower resource countries have not been extensively studied. Since text messaging is simple and cost-effective, more research should be conducted in lower resource countries where the highest burden lies in order to bridge this knowledge gap. Nevertheless, factors such as low literacy levels may present a barrier to the use of this mode of treatment.
Further research measuring fidelity to and compliance with the text messaging programme is crucial to ascertain the true effect of the intervention and whether the impact of text messaging remains after a messaging programme has ceased. Adverse event data should be systematically recorded and reported. Interviews with participants could explore other neglected topics to date, such as intrusiveness of messaging and participant burden (Berrouiguet et al., 2016).
Limitations
The inadequate reporting of some trials precluded classification of risk of bias as either low or high risk. This led us to rate some of the trials across the categories as unclear risk of bias. Another limitation is the small number of included trials and participants which contributed to the wide CIs observed in the meta-analysis. These limitations resulted in an overall rating of ‘very low’ quality of evidence in the summary of findings.
Conclusion
Statistically significant reductions in depressive symptoms were identified where the primary aim of the messages was to reduce depressive symptoms; in those trials using the BDI or PHQ-9 questionnaires; where text message content was targeted at mental well-being, mood improvement and CBT information; and when the message frequency was ⩾2 times per week. These results should be interpreted with caution due to methodological limitations associated with the included trials. More research is required before recommendations can be made about the routine use of text messaging interventions in this area.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. M.L.H. is a co-author of one of the included studies.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article. M.L.H. is funded by a National Health and Medical Research Foundation Career Development Fellowship (Level 2), APP1141328.