
Abstract
Background:
People with mental illness are vulnerable to abuse in the community. Cultural and social practices may be contributory.
Aim:
To explore the social representation of abuse of persons with mental illness among the inhabitants of Jakiri municipality in Cameroon.
Method:
This was a qualitative study based on the Theory of Reasoned Action, conducted in 2018 among 11 inhabitants of Jakiri municipality, aged above 18 years and who had lived in the town for at least 2 years. In-depth face-to-face semi-structured interviews were conducted. Data were analyzed using the basic thematic approach.
Results:
The belief that mental illness is incurable, a curse from the gods, a result of witchcraft, and a punishment for violation of core social norms were identified as the reasons for physical violence against persons with mental illness. Beliefs that persons with mental illness were disorganized, destructive, physically aggressive, and dependent on others were identified as reasons for emotional abuse.
Conclusion:
A misconception of mental illness was the major underlying factor for the abuse of persons with mental illness.
Background
The Universal Declaration of Human Rights (UDHR), a milestone document in the fight for human rights, states clearly that all human beings are equal in dignity and rights without distinction of any kind (UDHR, 1948). There are thirty articles in the document which affirm the right of every human being and these have been further elaborated over the years in international treaties and national constitutions (UDHR, 1948; United Nations International Covenant on Economic, Social and Cultural Rights [ICESC], 1976). Some of these seek to promote social protection, an adequate standard of living, and the highest attainable standards of physical and mental well-being as human rights (ICESC, 1976). All persons, including those with a disability are entitled to these.
To stem the high rate of violations against those living with disabilities, the treaty Convention on the Rights of Persons with Disabilities (CRPD) was declared in 2006 to ensure that persons with a disability had the right to equal treatment under the law, freedom from discrimination, social and economic rights in areas like education, health care, employment, and transport (United Nations. Department of Economic and Social Affairs Disability, 2006). Unfortunately, despite these and many other resolutions and their adoptions by several countries, the human rights violation of persons with disability (mental illness especially) continues unabated and at a global scale described as an “emergency” (Puras & Gooding, 2019; World Health Organization [WHO], 2020). These violations are on the rise and are reported to occur more frequently in low and middle-income countries (Puras & Gooding, 2019).
The abuse of persons with mental illness cannot solely be explained by a lack of resources (Puras & Gooding, 2019). It has been reported that cultural and societal practices that encourage the stigmatization, discrimination, and social exclusion of persons with mental illness could be contributory factors especially in developing countries (Mfoafo-M’Carthy & Sossou, 2017).
Unfortunately, global attention, especially by the mainstream media, has been mainly focused on the violence perpetrated by persons suffering or presumed to suffer mental illness, with many gruesome acts of violence attributed to mental illness (Pescosolido et al., 1999). The media sensationalizes such acts, thus giving rise to the unfortunate impression that most persons with mental illness are violent (Pescosolido et al., 1999). This has, in turn, has led to negative impression, fear, stigma, and discrimination towards persons with mental illness (Kabir et al, 2004; Varshney et al., 2016).
Research has shown that those who suffer mental illness constitute a small proportion of violent offenders and are vulnerable to violence and abuse (Large et al., 2011; Varshney et al., 2016). It has been reported that about 80% of persons with mental illness experience physical violence more than twice in their lifetime (Large et al., 2011; Varshney et al., 2016).
Some of the abusive practices against persons with mental illness could be related to how the abuse of persons with mental illness is represented in society. The social representation theory proposes that knowledge is a product of social construct and not merely a product of social cognition (Wagner & Hayes, 2005). It stipulates that social phenomena and its processes can only be truly understood if the historical, cultural, and macro-social conditions are put into perspective (Wagner et al., 1999). Thus, the social representation of mental illness is determined by ethnicity, cultural beliefs, religion, and language (Mfoafo-M’Carthy & Huls, 2014). In some patriarchal and highly traditional societies in Africa and Asia, differences in power dynamics may result in the belief that those who do not suffer mental illness rank higher in the societal strata than those with mental illness (Hofstede, 2011; Rosenfield, 2012). This has resulted in the belief that society (those without mental illness) has absolute power to protect and treat those who suffer mental illness, and has to safeguard itself from them (Hofstede, 2011; Rosenfield, 2012). This at times results in unintentional abuse, in a purported attempt to help and safeguard the individual, his family, or the society. The belief that persons with mental illness are cursed, different, dangerous, unproductive, and dependent on others for livelihood leads to segregation, discrimination, and abuse (Awad & Voruganti, 2008; Mfoafo-M’Carthy & Huls, 2014; Reisse & Roth, 1993). Poverty, lack of facilities, and human resources for the treatment of persons with mental illness make it difficult for these persons to receive the care they need (Mfoafo-M’Carthy & Huls, 2014). These lead to a prolonged illness, perpetuating of belief that mental illness is untreatable, caregiver fatigue, and ultimately abuse.
The violent acts against persons with mental illness include but are not limited to physical, sexual, or psychological abuse (Varshney et al., 2016). The specific acts include intimidation, neglect, beatings, forceful and prolonged restraint, sometimes leading to loss of limbs, amputations, rape, and refusal of rights to inheritance (Mfoafo-M’Carthy & Huls, 2014). The form and severity of abuse suffered are dependent on cultural factors, and the availability of resources for the management of these persons (Mfoafo-M’Carthy & Huls, 2014).
In Cameroon, there is no documented research work on the social representation of abuse of persons with mental illness. The frequent reports of abuse of persons with mental illness have prompted the researchers to seek to study the way the general society in Cameroon values, views, or represents violence in persons with mental illness.
This study will add to the existing literature on the social representation of violence. It will also identify the various socio-cultural factors that influence the abuse of persons with mental illness. The information provided could help social sensitization on the rights of this group of persons.
This research aims to study the social representation of violence against persons with mental illness and to describe the opinion of inhabitants of Jakiri, an urban municipality in Cameroon on physical violence and emotional abuse of this group of persons. It is hoped that the findings from the study will be used to identify the various socio-cultural factors that positively and negatively influence violence against persons with mental illness, provide information that could be used to sensitize the public against violence perpetrated against this group of persons.
Methods
The research was carried out in Jakiri, the urban capital of the Bui Division, Cameroon. The population of Jakiri town is well above 67,000 inhabitants. The inhabitants of Jakiri town are typically youthful and consist of indigenes, people from other parts of the country, and immigrants. A majority of the inhabitants are the indigenous people known as the Nso. There is limited access to good quality health care and education due to limited infrastructure, human resources, and funds. The inhabitants are mostly farmers and petty traders. The division has one psychiatric center and two mental health specialists.
Jakiri was chosen for this study because it has many homeless persons with mental illness probably because of its urban location and population. Abuse and violent acts against persons with mental illness are pronounced in the area and the inhabitants have strong cultural beliefs about mental illness.
This was a qualitative descriptive study based on the Theory of Reasoned Action. This method was thought to be fitting as it would enable the researchers to identify and uncover the meaning behind the social representation of violence against persons with mental illness. This method seeks to understand the perspectives of research participants in ways to bring about social change through collective action, through the belief that social practices determine how people view experiences, and that practices need to be modified to improve quality of life (Willig & Rogers, 2017).
Convenience sampling method was used. The sampling method was chosen in consideration of the subjects’ availability and willingness to participate, and the ability to communicate experiences and opinions in an articulate, expressive, and reflective manner. Primary data collection for this study took place in Jakiri, a sub-division of Bui, Cameroon, between March and April 2018. Face-to-face, semi-structured interviews with 11 inhabitants of Jakiri (7 male, 4 female) were conducted. The sample size was reached when no additional information on the topic was gotten from the respondents.
Participants were included in the study if they had lived in Jakiri town for at least 2 years, were aged above 18 years, could speak and understand English or Lamnso the local dialect, and gave consent to participate.
Semi-structured interview questions were used for the collection of data. The questions were divided into three sections. The first section covered demographic data. The second part was concerned with their views on physical violence towards persons with mental illness while the last section covered their impressions on emotional abuse of persons with mental illness. The interview guide was pretested in Kumbo for validity and some questions were modified. The instrument was translated into Lamnso language by a language expert. The iterative method was adopted. TCB clarified technical terms during the translation.
Door-to-door sample collection was done in the evenings on Sundays when most people could be reached at home. Only one eligible person was selected per household. The reasons for the research were explained to the occupants of the household and consent sought. Some of the participants who were not ready to respond to questions at the moment were revisited later at an agreed time that was convenient for them. Each interview lasted an average of 30 minutes. Those who could speak English were interviewed in English while the others were administered the translated version of the instrument by TCB.
The responses made by the participants were audio-recorded with the participants’ permission. Handwritten notes to complement the audiotapes and probes that could be followed up on subsequent interviews were taken. After each interview, data were coded and summarized into themes that served as probes to facilitate further interviews. These were done until data saturation was achieved.
Ethical consideration
An authorization letter was gotten from the authorities in Jakiri, which has an ethics committee to enable the researchers to carry out the study in the area. It was explained that participation was voluntary and that participants could decide to drop out at any time. Participants were informed that any information provided would be kept confidential. Written informed consent was obtained.
Analysis of data
This was based on thematic analysis. This approach was developed by Braun and Clarke for the identification of patterns or themes within qualitative data (Braun & Clarke, 2008). Thematic analysis was used because it is a flexible method that can be used in a wide range of research questions and epistemologies to generate trustworthy and insightful findings (Braun & Clarke, 2008). It helped in summarizing the key features of the data and allow for an accurate interpretation of data based on the perspectives of the different participants, highlighting the similarities and differences (Braun & Clarke, 2008; King, 2004). Since this was an exploratory study, the thematic analysis allowed for detailed, complex, and accurate analysis of the data (Braun & Clarke, 2008).
Data was gotten from a direct interview, transcribed, summarized and themes brought out which were grouped into categories and used for analysis. The analysis was done category by category and theme by theme.
The interviews were transcribed verbatim and checked for accuracy against the audio recording. Information that could identify the participants was removed from the manuscript. The manuscript was read several times to identify the emergent themes, which were coded manually. To ensure credibility, pre-existing expectations were set aside during the process of analyzing the data to ensure an accurate representation of the participants’ narrative (Braun & Clarke, 2008; Myers & Avison, 1997). Two researchers with a good knowledge of qualitative studies coded the manuscript differently; similarities and differences in the two resulting sets of codes were discussed and resolved. The themes and sub-themes identified were discussed (Merriam, 2002).
Findings
Socio-demographic distribution of the participants
Seven males and four females participated in the study. Nine of the participants were indigenes of Jakiri while the rest were non-indigenes who had been living in Jakiri for more than 2 years. Seven were aged 18–39 years; three were aged 40–59 years while one was above 60 years old. Six of the males were married, while one was divorced. Three of the female participants were married and one widowed. Six of the participants had completed primary education, one had an ordinary level certificate, two had completed advance levels, and two had completed tertiary education.
Definition of mental illness
Three major themes were identified in the definition of mental illness; altered thinking process, disruption of function, and incurable disease (Table 1). On an altered thinking process, some of the participants believed mental illness is a disease of the mind and a disease that brings about disability. Rahina noted that “they are diseases that make someone not to reason well or work.” Under disruption of functions, mental illness was believed to be a disease of the brain. Clifford noted that “It damages the brain of the affected person and makes him as an imbecile”. Others saw mental illness as a disease that has no cure. Boris said, “They are a disease of witchcraft and curses from gods and so has no cure.”
Emerging themes and sub-themes on the representation of mental illness.
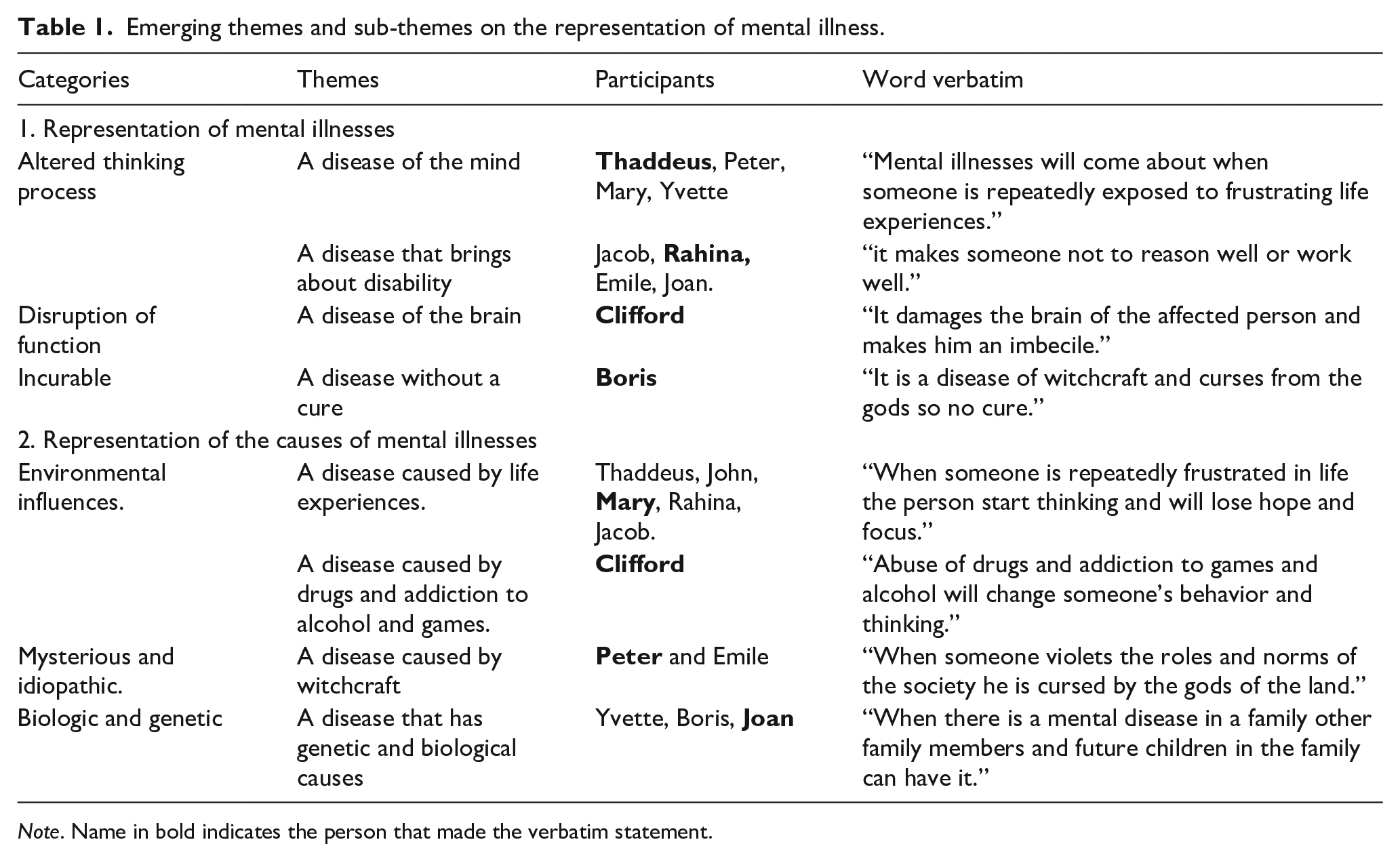
Note. Name in bold indicates the person that made the verbatim statement.
Representation of the causes of mental illness
On the representation of the causes of mental illness, the categories were; environmental cause, mysterious or idiopathic cause, and genetic or biological cause (Table 1).
On environmental cause, the themes brought forward were that mental illness was caused by adverse life experiences and abuse of /addiction to drugs, alcohol and, gambling. Mary reported that “when someone is repeatedly frustrated in life the person starts thinking and will lose hope and focus” while Clifford believed that “abuse of drugs and addiction to gambling and alcohol will change someone’s behavior and thinking.” Some of the participants believed that the origins were mysterious and idiopathic. Peter reported that “when someone violates the social norms and roles of the society, he or she is cursed by the gods of the land.” Others believed in a biological cause. Joan reported that “when there is a mental illness in a family, other family, members and future children in the family can have it.”
Representation of physical violence against persons with mental illness
Three themes emerged. These were maltreatment of persons with mental illness, a form of minimization of worth and, an act of hatred (Table 2). Thaddeus said, “When you think someone is inferior to you in everything, you start to minimize the person.” As an act of maltreatment, John reported that “when you do something bad to someone when he or she does not like it”. While as an act of hatred, Peter said, “When you hate someone, you start beating him or her and can even kill the person.”
Emerging themes and sub-themes on the representation of physical violence.
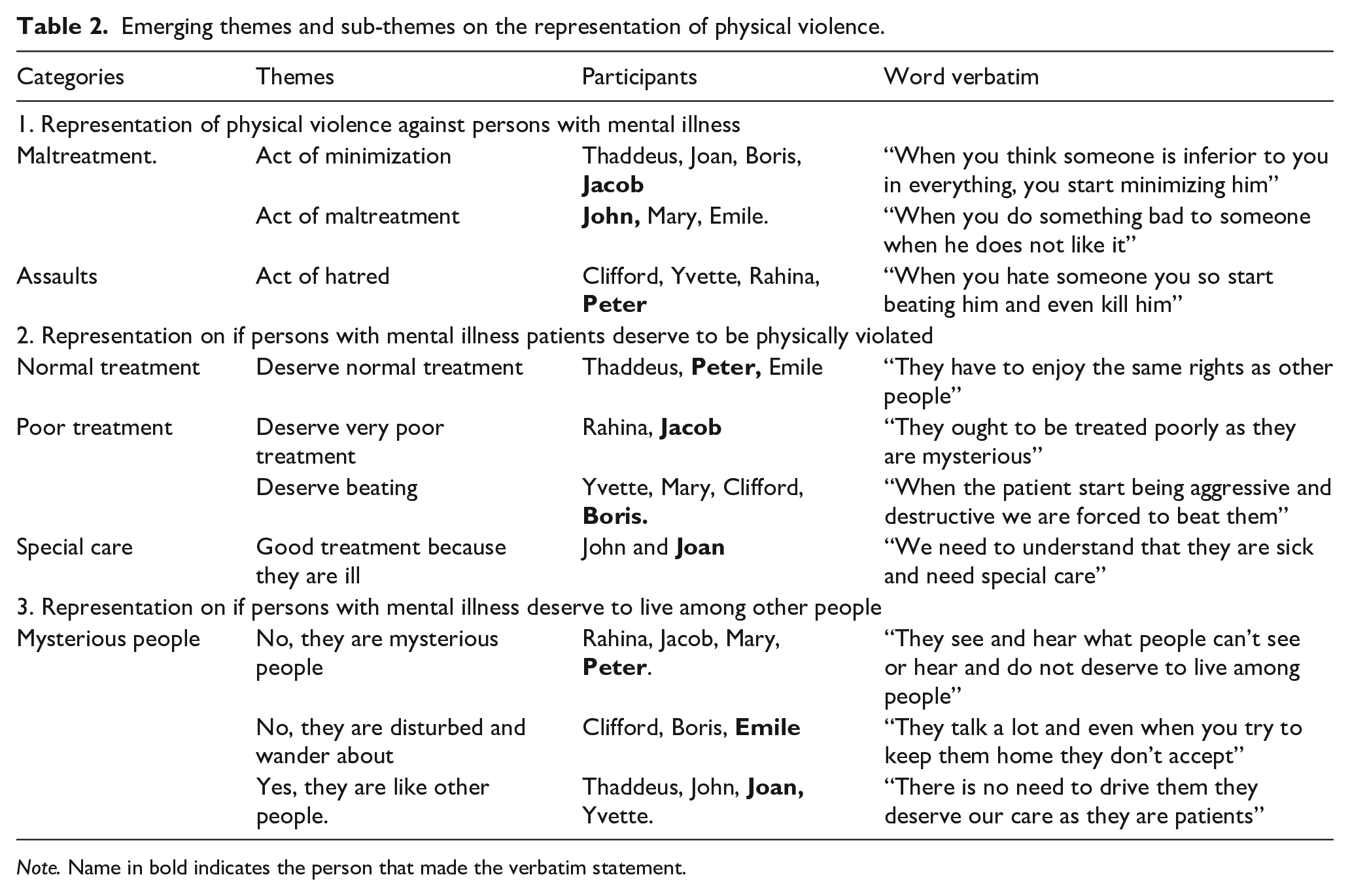
Note. Name in bold indicates the person that made the verbatim statement.
Opinions on whether persons with mental illness deserve to be physically violated
The participants had a diverse opinion on this which included categories like persons with mental illness deserve normal treatment, deserve to be treated poorly and, deserve to be treated well. Peter believed that they should be treated like every other person in the community. He said, “They have the same right to be treated like other people or children in the society they are in.” Others felt they should be treated poorly. Jacob said, “They ought to be treated poorly as they are mysterious.” Boris shared the same thoughts because of their behavior. He said, “when they start being aggressive and destructive we are forced to beat them very well.” Joan who did not support this view said, “We need to understand that they are sick and need special care.”
Representation on if persons with mental illness deserve to live among people
Some of the participants believed that persons with mental illness should not live among other people. Peter believed that “they see and hear things that other people can’t see or hear therefore do not deserve to live among people.” Emile said “they talk a lot and even when you try to keep them home they don’t accept” so they don’t have to live amongst people. Joan believed they were sick and as a result “there is no need to drive them away. They need and deserve our care as they are ill.” (Table 2).
Representation of emotional abuse of persons with mental illness
Representation of stereotyping persons with mental illness
Some of the participants believed that stereotyping was a way to undermine, discriminate, and stigmatize persons with mental illness. Boris believed that “they do not reason well and are dirty.” Rahina believed that this occurs because the patients are dependent on other people for survival and said “providing for someone all the time is exhausting, especially if he or she keeps asking.” The patient’s behavioral problems contribute to name-calling. It is believed that sometimes they like the names and give it to themselves. Yvette reported, “Some of them like the names and some are the ones that give themselves the names” (Table 3).
Emerging themes and sub-themes on the representation of emotional abuse.
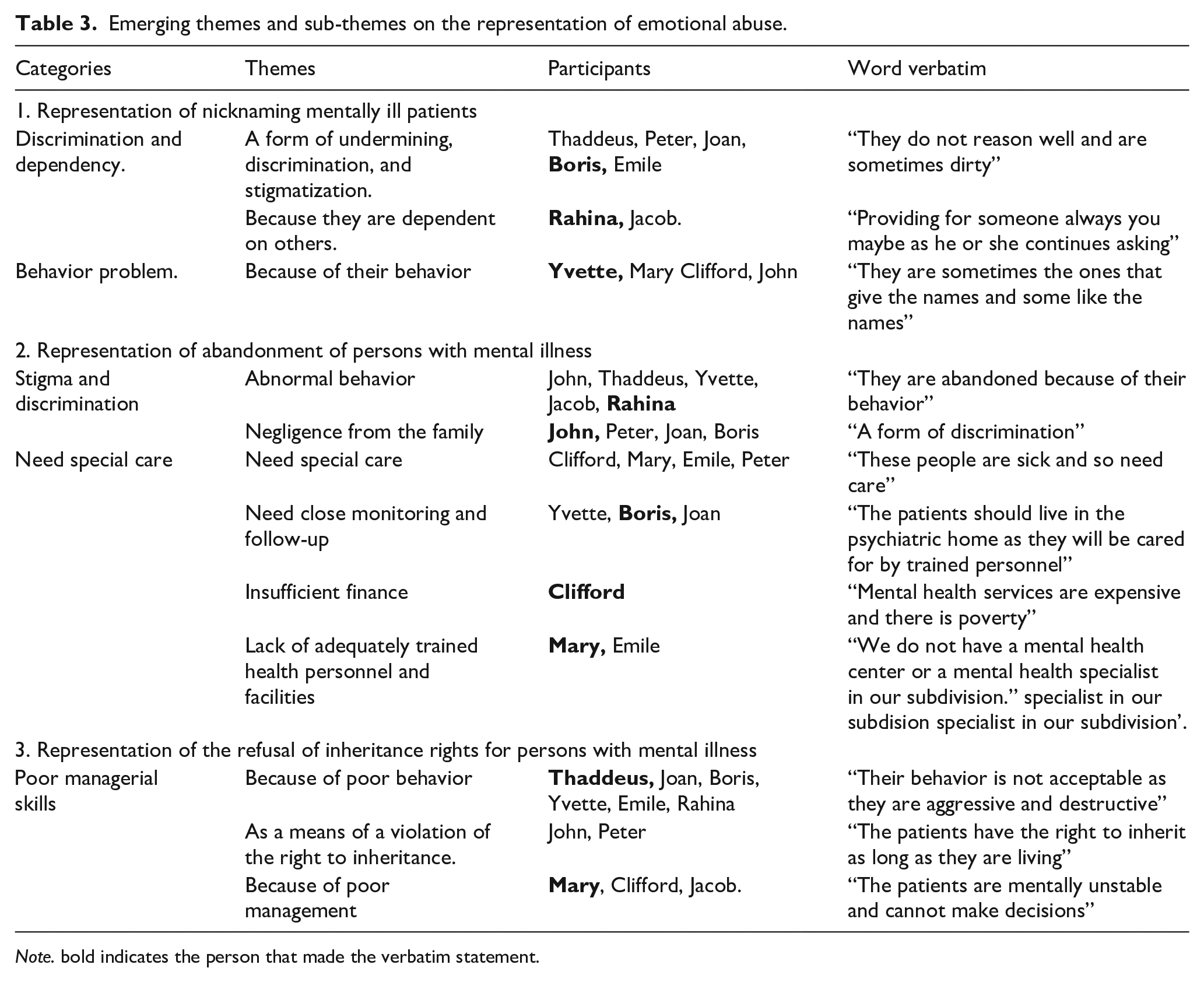
Note. bold indicates the person that made the verbatim statement.
Representation of the abandonment of persons with mental illness
Stigmatization and the need for special care were identified as the main categories. Insufficient finances, lack of adequately trained health personnel, and mental health facilities were identified as the sub-categories under the need for special care.
Abandonment was seen to be a result of stigma and discrimination towards these persons. Rahina said, “They are abandoned because of their abnormal behavior.” Jacob justified abandonment by claiming “they are abandoned because the patients themselves do not like to stay home and never come back when they go out.” John opined that “they are abandoned just to separate them from other people. That is all.” He also believed it was an act of negligence from the family, “a form of discrimination” (See Table 3).
It was believed that persons with mental illness need specialized care and close monitoring, and need to live in specialized homes and hospitals. Boris stated, “The patients should live in psychiatric homes and be cared for by trained personnel.” The need for special care for the persons with mental health conditions was identified as a serious issue by Clifford who said, “The people are sick and so need care.”
Insufficient finance, adequately trained health personnel, and health facilities posed a big problem to Clifford who said, “given that mental health services are expensive and there is poverty, it is difficult to care for them and we have no choice than to abandon them.” Mary thought that “we do not have a mental health center or a mental health specialist in our subdivision.”
Representation of the refusal of the right to inheritance
Patients are refused the right to inheritance because of their perceived abnormal behavior as expressed by Thaddeus who stated, “Their behavior is not accepted as they are destructive and aggressive.” Refusal of inheritance was seen by Peter as a violation of human rights and the basic right to inheritance. His opinion is “a person has the right to inheritance as long as he or she is living.” Notwithstanding, because of perceived poor managerial skills, persons with mental illness are disinherited. Mary stated, “The patient is unstable mentally and cannot take the right decisions” (See Table 3).
Discussion
This paper studied the representation of violence against persons with mental illness in a district in Cameroon, Central Africa.
Representation of mental illness
The participants had different views on the definition of mental illnesses. It was believed that mental illness was an illness associated with altered behavior, thinking, reasoning, and disturbance of the mind. These views are similar to what was reported in a study carried out in Slovakia by Letovancová et al. (2017) on the attitude of the society towards people with mental illness. They found that the knowledge that mental illness was a disturbance of emotion, thinking and, behavior ensures a more positive attitude towards persons with mental illness. The participants variously believed that mental illness was caused by adverse life events, witchcraft, violation of social norms and roles, loss of a valued object or a significant figure, substance abuse, and gambling. Choudhry et al. (2016) reported that mental disorders were interpreted to be the result of the wrath of God, curses, and evil spirits. The views represented here may be linked to the observation that many people with mental illness are people who use psychoactive substances. The responses we got on supernatural causes of mental illness may have been informed by the widespread strong cultural belief system that supernatural forces play a major role in the causation of mental illness (Razali et al., 1996). This belief is bolstered by the erroneous portrayal by the indigenous film industry of mental illness being a result of malevolent spirits, witchcraft, and charms (Aina, 2004). These patients are also portrayed as malicious and violent (Aina, 2004). This belief system is so entrenched that even after medical education, health practitioners still hold on to the belief of the supernatural origins of mental illness (Adewuya & Oguntade, 2007). They perceived these patients as dangerous and with poor prognosis (Adewuya & Oguntade, 2007).
Representation of physical violence against persons with mental illness
The participants were knowledgeable about physical violence perpetrated against persons with mental illness in the town. Unfortunately, five of the eleven participants found nothing strange in persons with mental illness being abused. Their responses were not strange as there exists a common saying in the town that “the cure for mental illness is beating” (Lamso proverb), as a result of which indigenes mostly from Banso tribe see physical violence as a solution to mental illness. The belief that persons with mental illness should be isolated from the wider community because they were responsible for their problems and could harm other people is similar to views held in different communities in both developed and developing countries (Harvey & Brophy, 2011). However, more of the participants believed that mental disorders were not different from physical disorders and were of the view that persons with mental illness should be allowed to live among the general populace. This is similar to the views of Hall et al. (2019) that persons with mental illness deserve social inclusion, respect, and empathy just like other persons.
Representation of emotional violence against the mentally ill
Stuart et al. (2003) reported that the acceptance of discrimination and violation of the right of persons with mental illness occurs as a result of the public perception of a link between mental illness and violence. Dependence, strange and aggressive behavior, and blame for being responsible for their illness were some of the reasons given for emotional violence. The opinion that the mentally ill person should be abandoned may stem from the belief that mental illness cannot be cured, that the patient is uncontrollable, destructive, a nuisance and when allowed or sent out may bring relief to the family members. Lack of access to care, exorbitant cost, and out of pocket nature of treatment increases the burden of care on relatives and these could lead to the abandonment of the relative when they can no longer cope with the illness. These views remain unchanged partly due to a lack of policies in most countries on the rights of persons with mental illness.
Conclusion
Violence against persons with mental illness has been and is still a major public health problem. The misconception that mental illness is incurable, caused by witchcraft, a violation of social norms and customs, a curse from the gods, and that the persons were responsible for their predicament were identified as the main reasons why physical violence was meted out on persons with mental illness in Jakiri. The belief that these persons were aggressive and a burden to others were identified as some of the reasons for emotional abuse.
Strengths and limitations of the study
The result cannot be easily generalized to other populations, since data collection was limited to a particular town of the region whose indigenes have their peculiar experience with mental illness. It is recommended that the breadth of research in terms of regions covered be widened in future research. It would also be necessary in subsequent research to get first-hand knowledge from the key stakeholders how these representations can be changed.
Recommendations
Given the widespread misconception of mental illness among the participants, it is suggested that healthcare providers and other stakeholders should make more effort in increasing the awareness of mental illness. They should create mechanisms to assess and improve the human rights conditions of people with mental illness. Also, more mental health personnel and facilities need to be provided, especially at the primary healthcare level to improve access to care and enhance the proper treatment of persons with mental illness.
Footnotes
Acknowledgements
We wish to appreciate Dr. Menguene Laure for helping with data coding.
Author note
This paper has not been published in any other journal.
Declaration of conflicting interests
e.g., The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article..
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.