
Abstract
Objective:
Research and study the Lebanese employers’ attitudes, toward recruiting candidates with a mental illness and toward their employees who suffer chronic mental illnesses (A CMI) and the factors that may play a role in affecting it.
Methods:
A combined cross sectional and retrospective study. Interviews conducted with a mix of 63 human resource managers and high executive employees to assess the integration of people with A CMI at the workplace, and the attitudes toward them.
Results:
Primarily, the engagement of an occupational physician or a social worker in the process, was associated with a reduction in stigma surrounding the subject matter. Moreover, hiring a candidate with A CMI was perceived as a social image improvement of the hiring company. However, A CMI employees were perceived as having lower efficiency and self-esteem, as well as a greater vulnerability to dismissal.
Conclusion:
The presence and engagement of an occupational physician, and/or a social worker, has been found to be the main positive stigma modulator against mental illness, in a corporate setting.
Introduction
Employment is considered to play a major role in a person’s health and wellbeing. It leads to integration in society, ensures a sense of autonomy, and enhances physical, mental, and social wellbeing (Stoewen, 2016). Therefore, the workplace represents an important setting that improves overall health and welfare, as well as all socioeconomic domains (Luciano & Meara, 2014). Those findings apply to both, the general population and people with mental illness. As a matter of fact, work has a positive impact, among people with a chronic mental illness (A CMI), associated with psychosocial, clinical, and economic improvements, which correlates with a reduction in mental health related costs (Luciano & Meara, 2014). Despite this, people with a mental disorder suffer higher unemployment rates. In fact, across the entire range of occupations, only less than half the population with mental disorders, are employed, leaving millions of others unemployed (e.g. 5–6 million in the US). These rates are higher in developing countries (e.g. 78.62% of the self-reported mentally ill in India were unemployed) and in people with more severe mental illnesses (Luciano & Meara, 2014; Mechanic et al., 2002; Ramasubramanian et al., 2016). For example, employment rates for people with schizophrenia are estimated between 10% and 20% in Europe, 4% and 27% in the UK, and 3% and 42.8% in the US (Eurostat Statistics Explained, 2021). Moreover, among those who do actually work, mental illness causes them a decrease in annual income by an amount ranging between $3,500 and $6,000 (Marcotte & Wilcox-Gök, 2011). In fact, 38.5% of people with A CMI have an annual income under $10,000 (Mechanic et al., 2002). Therefore, it is a public health priority to monitor disparities in employment by mental health status.
There exist multiple barriers to employment. Mainly related to medical factors, such as multiple hospitalizations records, longer illness durations, comorbid personality disorders, depression symptoms, and drug intolerance (Tse et al., 2014). In addition, they can be due to psychosocial factors, such as a lack of social services and protective legislation, low education level, low cognitive performance, and marital status (Cook, 2006; Milfort et al., 2015).
However, of all barriers, stigma and social representations surrounding mental illness remain the greatest obstacles to employment (Ebuenyi et al., 2018). Stigma is linked to general public attitudes, characterized by strongly negative stereotyping, including misperceptions about such people being frightening, aggressive, unpredictable, less intelligent, and lacking self-control. This leads to the marginalization of people with A CMI with regards to employment (Hampson et al., 2018; Schulze & Angermeyer, 2003). In the workplace, disclosure of mental health problems are often surrounded by stigma, hence recruitment discrimination, behavior misattributions, and stress (Brohan et al., 2014). In addition, there are employers and colleagues who exhibit quite a stigmatizing behavior toward other employees who are known to have a mental illness. Those behaviors go to the extent of restricting opportunities for promotions, micro-managing, over-attributing mistakes to the illness, malicious gossiping, and subtle forms of social exclusion (Corrigan & Lundin, 2001). Finally, social stigma can also be harmful to the mentally challenged, causing greater self-stigmatization, (self-categorization as ‘mentally ill’ or internalization of stigma) associated with lower self-esteem and self-efficacy (Pasmaztzi et al., 2016). Consequently, reducing social stigma remains one of the most important action steps, to encourage and improve the integration of people with A CMI in the workplace (Ebuenyi et al., 2018).
While a multitude of studies have been undertaken in the western world, only a few were initiated in the Middle East, specifically in the Lebanese society, still with no official data available, in regards to the number of mentally challenged people in Lebanon. Nonetheless, according to a few studies, the number of people with a mental illness, is in the vicinity of 25% (Karam et al., 2008). The literature focuses mainly on studying stigma toward individuals with a mental illness in the general population, which is substantial in the Middle East. In fact, stigmatizing attitudes are particularly prominent with regard to culturally proscribed mental illnesses, like alcoholism and drug abuse, and less prominent regarding other disorders such as depression and psychosis (Sewilam et al., 2015). Multiple interviews were carried on with a number of employers in firms, of which, only seven, were found to employ persons with intellectual deficiencies. All seven employers, recommended the supervision of these specific people at work, at least for the duration of their first month of employment. However, when compared to their colleagues, there was total benefits equality (equal salaries, access to social security, number of days-off), and even additional benefits (multiple breaks, facilitation of tasks in case of difficulties, call for assistance. . .).
Given the scarcity of data on the Lebanese job market, concerning the employment status of individuals with mental illnesses, and their experiences, we launched this study to analyze the views of employers toward people with A CMI, as well as their attitudes when it comes to recruiting and employing them. This study will provide a better understanding regarding the needs of individuals with A CMI. Allowing us to develop specific and relevant social interventions for a better guidance in the workplace.
Methods
Study design
This study is a combined cross sectional that was conducted during the period between March and June of 2018. Quantitative data were collected through interviews, conducted with 63 human resources managers (HRM) and high executive employees (HEE) who are in charge of recruiting candidates, for national and international companies, located on the Lebanese territories The 63 HRM and HEE were selected randomly at the ESA business school (Ecole Superieure des Affaires), where more than 100 were enrolled in a Masters (MBA) or a Doctorate in Business Administration (DBA). The companies they represent, function across several different sectors (communication and media, sales and manufacturing, education, healthcare and pharmaceutical, business/banking and finance, hospitality. . .), and they are located in both urban and rural areas. The questionnaire filled by each one of the HRM/HEE interviewees consisted of three parts. One single meeting was held for the duration of around 1 hour, and without any benefits to engage in the study.
Ethical approval
The study protocol got its approval by the Saint-Joseph University in Beirut ethics committee. The study was conducted maintaining anonymity, to respect the confidentiality of respondents. All participants agreed by providing a written consent.
Questionnaire
The questionnaire consisted of, first, a characteristics data preview (company size, head office location, working sector, reliance on occupational physicians and social workers), second, a shortened version of the Community Attitudes Toward the Mentally Ill (CAMI) survey for the general attitudes and representations, and third, a 20-item questionnaire, specifically prepared to target various aspects of the integration of people with mental illness in the workplace.
For the purpose of this study, we used a modified version of the CAMI questionnaire developed by Mehta et al. (2009). It consists of a 26-item survey divided into four subscales illustrating different aspects of attitudes. It has a solid multicultural validity, which is the reason we selected it for this study. The first subscale is authoritarianism (AU) and it refers to the view of a person with a mental illness, as someone inferior and who requires supervision. The second subscale is benevolence (BE), it refers to a humanistic and sympathetic view toward people with a mental illness. The third subscale is social restrictiveness (SR), which refers to the belief that people with A CMI are a threat to society and should be avoided. Finally, the fourth subscale is community mental health ideology (CMHI) and it refers to the acceptance of mental health services, and the integration of people with A CMI in the community. A higher score on each subscale correlates with a higher rejection of mental illness in the community (Mehta et al., 2009).
Finally, a 20-item tailored questionnaire was developed in order to target various ‘aspects of the integration of people with A CMI in the workplace’. The professional and functional aspect (absenteeism, efficiency, and peer interaction: questions 1–4), the benefits (salary, retirement benefits, annual and sick leave, social security: questions 5–9), the legal aspect (dismissal, disease disclosure: questions 10 and 11), the positive predictors (trainings, supervision, higher level education: questions 12–14), the work limitations (stigma, prerequisites, social interaction, self-esteem: questions 15–18), and the positive representations (questions 19 and 20). We used the Likert scale from 1 to 5 (1: strongly disagree, 2: disagree, 3: neither agree nor disagree, 4: agree, 5: strongly agree), with higher scores reflecting a negative representation toward people with A CMI.
Participants
The criteria for inclusion of participants in the study, consisted of representing a national or an international company, located on the Lebanese territories, and offering only paid employment. Whereas the exclusion criteria were the following: charitable associations, non-lucrative associations, and establishments adapted to people with special needs. Having a known psychiatric condition was also an exclusion criteria for participants.
Data analysis
Data analysis was performed, using SPSS 23.0 software for statistics. Normality of distributions was checked using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Owing to their significant departure from Gauss distribution, the variables were analyzed using independent samples Kruskal Wallis, Mann Whitney U test and the Spearmann rank correlation test. Significance level between variables and CAMI sub scales were determined at p < .05.
Results
Company’s characteristic
A total of 63 executive employees were interviewed about their companies’ strategies and perceptions regarding people with A CMI. The majority of the companies were in urban areas, big sized, and national. However, only a minor amount of those companies had an occupational physician or a social worker, and an even lesser amount, who had employees with any kind of disability (physical or mental), more specifically employees with A CMI. All selected companies’ characteristics are shown in Table 1.
Company’s characteristics.
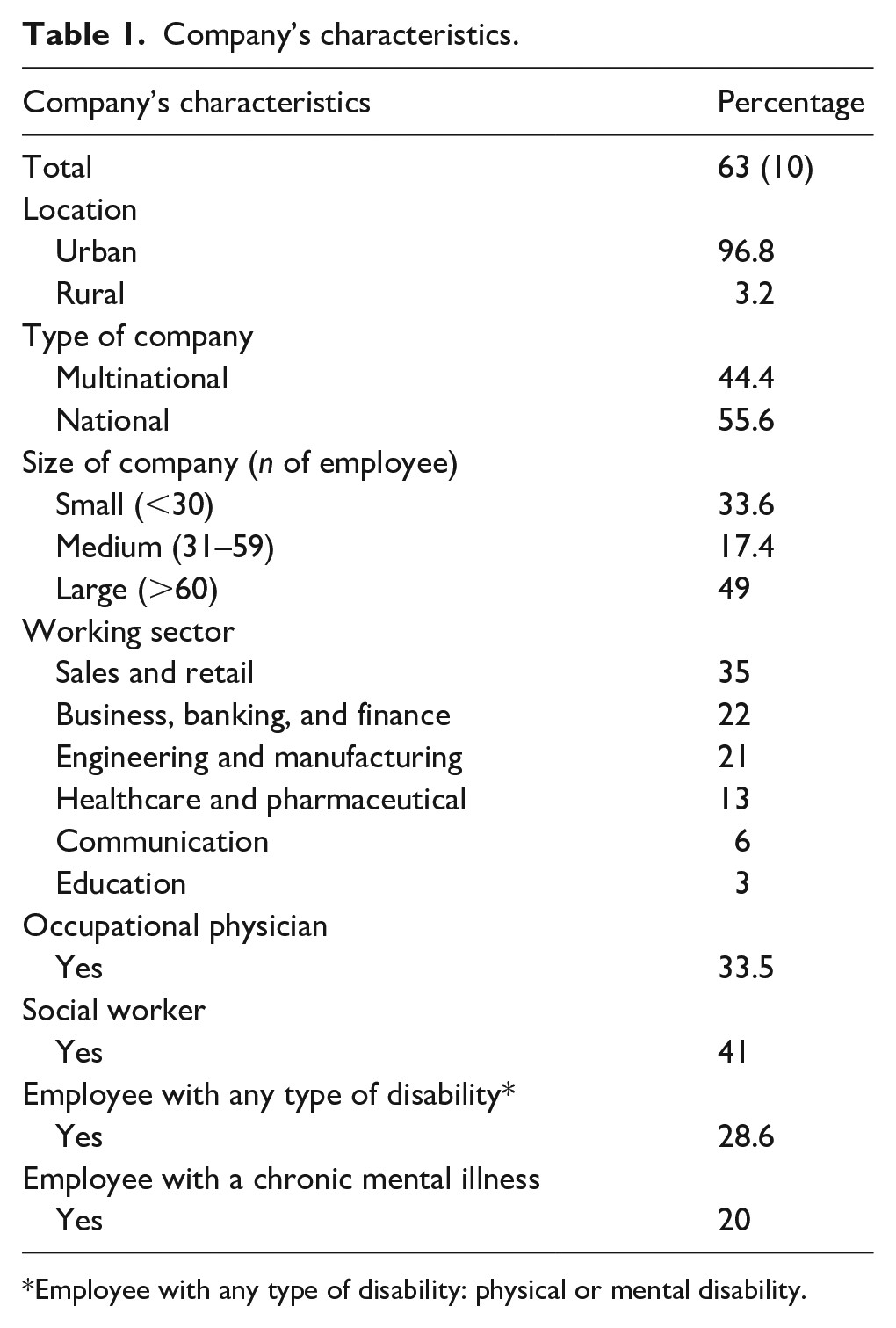
Employee with any type of disability: physical or mental disability.
CAMI scores and differences according to the company characteristics
The highest and lowest mean scores were measured on BE (26.4 ± 6.9) and CMHI (16.2 ± 5.1) respectively. As for AU and SR, mean scores were 18.94 ± 4.2 and 16.27 ± 5.1, respectively.
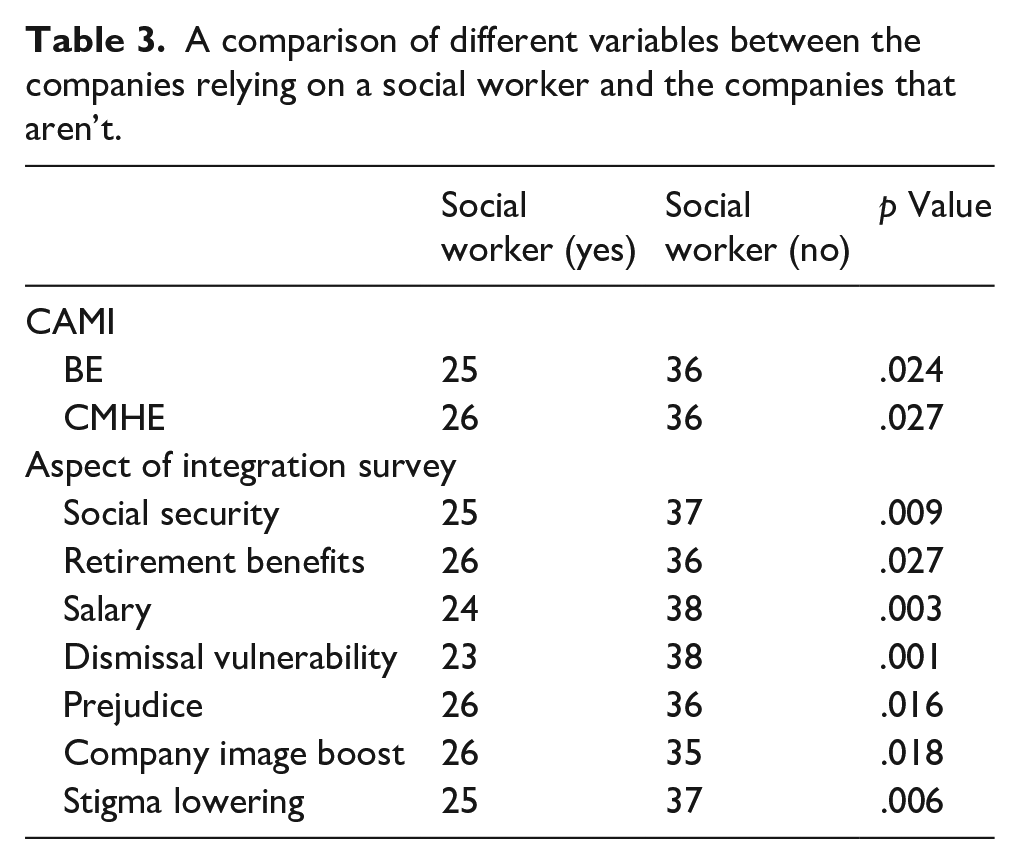
None of the four subscales of the CAMI questionnaire showed a significant statistical difference regarding the location of the company, the working sector, the size, and the type of the company. The only significant difference was found for companies who have an occupational physician, or a social worker. In fact, companies who have an occupational physician, had lower BE (myes = 24, mno = 36, p = .02) and CMHI scores ((myes = 24, mno = 35, p = .019). The same goes for those who have a social worker, they also had lower BE ((myes = 25, mno = 36, p = .024) and CMHI scores ((myes = 26, mno = 36, p = .027). Tables 2 and 3 illustrate the significant results of the CAMI and ‘aspect of integration survey’ according to the presence or absence of an occupational physician or a social worker, respectively.
A comparison of different variables between the companies relying on an occupational physician and the companies that aren’t.

A comparison of different variables between the companies relying on a social worker and the companies that aren’t.
The previous results show that involving a social worker or an occupational physician for the company, are the main factors that may positively affect the attitudes toward employees with A CMI.
‘Aspects of the integration of people with a A CMI in the workplace’ questionnaire
None of the aspects of this questionnaire showed a significant statistical difference regarding the location, the working sector, the size, and the type of the company. The only significant difference, was found for companies who have an occupational physician, or a social worker involved. In fact, a significant positive association was noted between having an occupational physician and acknowledging the rights of people with A CMI regarding social security, annual leave, retirement, salary, and perceiving their hiring, as an improvement to the social image of the company. On the other hand, having an occupational physician was associated with perceiving lower efficiency and self-esteem of people with A CMI and a greater vulnerability to dismissal. Table 2 illustrates the latter findings.
In addition, there was a significant positive association between having a social worker involvement with the company and acknowledging the rights of people with A CMI regarding social security, retirement, salary, and acknowledging prejudice as an obstacle to employment. Furthermore, these companies perceived hiring someone with A CMI as a boost to their social image and a way of lowering the stigma associated with health issues. On the other hand, having a social worker engaged, was also associated with perceiving a greater vulnerability to dismissal for people with A CMI. Table 3 illustrates the latter findings.
Discussion
In this study, the highest and lowest mean scores of the CAMI subscales were measured on benevolence and community mental health ideology respectively. This reflects an overall low humanistic and sympathetic approach toward people with A CMI, but a satisfying acceptance of their integration in the community and a positive reaction toward applying mental health services. Overall stigma was less prominent in Lebanon and mainly concentrated in lower benevolence, comparing to other Arab or even middle-income countries (as classified by the World Bank Economies, 2018), which are known to be more stigmatizing than the developed countries (Mehta et al., 2009).
Indeed, having an occupational physician and/or a social worker was associated with lower BE and CMHI scores. This reflects less stigma and a better acceptance of people with A CMI and their integration in the community. This is partly because employers who have access to mental health information through an occupational physician or a social worker could have better understanding on mental illness. This may result in accepting people with A CMI and dissolving prejudice toward them (Taylor & Dera, 1981).
The companies relying on an occupational physician, showed a better acknowledgement of the rights of people with A CMI (salary, social security, retirement benefits. . .) and perceived their hiring as an improvement of their social image. In fact, having an occupational physician well informed about mental health was associated with a faster and sustainable ‘return to work’ after a relapse, which improved the self-efficacy of the employee (Ciftci et al., 2013). Thus, the employee can function at the same level of a healthy person, and would therefore be entitled to the same benefits, without any kind of discrimination. Acknowledging this, improves the public image of the company.
On the other hand, having an occupational physician, was associated with perceiving a greater vulnerability to dismissal. This can be explained by the poor assumption, that the occupational physician, can denounce a relapse and let the employee incur a risk of dismissal. Psychiatrists are often concerned about putting their patients in a vulnerable situation, by providing their personal medical information to the company’s occupational health doctor (Barke et al., 2011). This misconception may be due to a lack of collaboration between the concerned specialties involved with the occupational health physician, as shown in a German survey, revealing that around 30% of the primary care physicians, psychiatrists and psychotherapists never had contact with an occupational health physician (Van Beurden et al., 2015).
Relying on a social worker in a company, protects the employees’ rights, especially those with A CMI, regarding a fair salary and an equal access to social security and retirement benefits. It also decreases prejudice against mental illness, which is well acknowledged by the social workers to be an obstacle for employment (Okawara et al., 2018). Companies relying on a social worker, also perceive hiring someone with a stable mental disorder as a way to lower social stigma, associated with health issues, and as a consequence, a way to improve the work performance of the employee with an A CMI. In fact, social stigma leads to a greater self-stigma, which is associated with lower self-esteem and self-efficacy (Pasmatzi et al., 2016).
This study has possible limitations. First, the views expressed may not be generalized, since the data presented are based on a convenience sample. Second, some of the answers to questions about stigma, might have been vulnerable to social desirability: respondents could have refined their answers to suit expectations. Third, the expression ‘mental illness’, however explained to each participant at the beginning of the survey, might have been misunderstood and susceptible to different interpretations. Respondents might have had a more limited range of disorders in mind when they answered the questions, or on the contrary, confounded certain common misused terms as mental disorders (ex: ‘malade imaginaire’ and ‘hysteria’ were found between the answers of the participants).
Conclusion
We studied the perceptions and attitudes of a sample of companies located on the Lebanese territories regarding the employment of people with a stable mental illness. Our results showed an overall low humanistic and sympathetic approach toward them; however, they were not majorly perceived as inferior or as a threat to others. Two positive stigma modulators were identified: relying on an occupational physician and hiring a social worker. These modulators contributed to the improvement of the mental health services’ integration in the community, and to improve acknowledgement of the rights of the employees suffering an A CMI.
A collaboration on a multidisciplinary scale (psychiatrist, occupational physician, social worker) can provide a better perspective on how to manage the limitations related to mental illness.
Further qualitative studies need to be conducted, in order to evaluate the personal experience of people with A CMI in the workplace. This might be of interest to duplicate our results and draw some conclusions in order to suggest further social interventions to improve working conditions.
Footnotes
Author’s note
The manuscript does not contain clinical studies or patient data.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.