
Abstract
Aims:
The aim of the study was to estimate the prevalence and correlates of psychological distress (PD) in three small Pacific Island countries.
Method:
National cross-sectional data (pooled sample N = 3,088, 18–69 years) of participants from the STEPS surveys in Nauru (2015/16; N = 1382), Tukelau (2014; N = 554) and Tuvalu (2015; N = 1152) were analysed.
Results:
In the pooled sample 30.4% participants had PD (⩾20 scores), 18.1% mild (20–24 scores), 7.8% moderate (25–29 scores) and 4.4% severe (30–50 scores) PD. The prevalence of PD in Nauru was 41.5%, in Tukelau 5.0% and in Tuvalu 22.7%. In the adjusted logistic regression analysis with the pooled sample, younger age (18–39 years), alcohol family problems, heart attack/stroke, current smoking, high salt intake and high sedentary behaviour were positively associated with PD, while male sex and being from Tukelau and Tuvalu were negatively associated with PD.
Conclusion:
Almost one in three participants reported PD and several associated factors were found that can be targeted in population interventions.
Introduction
Psychological distress (PD) (mainly depressive and anxiety symptoms) (American Psychological Association, 2023) is often used for the description of mental health in the general population (Drapeau et al., 2014). In national population-based surveys, the prevalence of PD among adults in high-income countries ranged from 10.0% to 11.1% in Australia (Enticott et al., 2016), 20.7% in Canada (Caron and Liu, 2011) to 26.8% in Japan (Sakurai et al., 2010), and in middle income countries 23.9% in South Africa (Mthembu et al., 2017), 18.1% in Kiribati (Pengpid & Peltzer, 2021a) and 18.9% in Solomon Islands (Pengpid & Peltzer, 2021b). There is scant information on PD in small Pacific Island countries, such as in Nauru, Tokelau and Tuvalu, which prompted the study. Nauru is an upper middle-income country (9,852 population, 68.3 years life expectancy) (The World Factbook, 2023a), Tokelau has a population of 1,647 (The World Factbook, 2023b) and Tuvalu is an upper middle-income country (11,639 population, 68.7 years life expectancy) (The World Factbook, 2023c). It is important to identify the prevalence and correlates of PD in the study countries so that policy makers can develop and prioritize interventions to prevent and control PD (Tadic et al., 2023).
Several studies showed that lower socioeconomic status (Caron and Liu, 2011; Chittleborough et al., 2011; Enticott et al., 2016; Myer et al., 2008), female sex (e.g. Matud et al., 2015; Mthembu et al., 2017), not married (Mthembu et al., 2017; Pengpid & Peltzer, 2021b, Takeuchi & Speechley, 1989) and were associated with PD. History of adverse life events (Caron & Liu, 2011; Lui et al., 2018), such as alcohol related problems in the family and family history of suicide or suicide attempt (Pengpid & Peltzer, 2021a), including the diagnosis of a serious disease, such as cardiovascular disease (Chittleborough et al., 2011; Kuriyama et al., 2009; Pengpid & Peltzer, 2021a, 2021b), have also been found associated with PD.
Furthermore, various health risk behaviours increasing the odds of PD, include low vegetable/fruit consumption (e.g. Cockerham et al., 2006; Richard et al., 2015), physical inactivity (e.g. Rees et al., 2012; Sloan et al., 2013), current smoking (e.g. Chittleborough et al., 2011; van der Deen et al., 2011), hazardous alcohol use (Cockerham et al., 2006; Mthembu et al., 2017), salt intake (Shimizu et al., 2015) and high sedentary behaviour (Chu et al., 2018; Sloan et al., 2013), The aim of the study was to estimate the prevalence and correlates of psychological distress (PD) in three Pacific Island countries (Nauru, Tokelau and Tuvalu).
Methods
Participants
National data from the 2015–2016 Nauru (74.5% response rate), 2014 Tukelau (70.0% response rate) and 2015 Tuvalu (76.0% response rate) cross-sectional STEPS surveys were analysed (World Health Organization [WHO], 2018). A simple random sample design was applied to produce representative population data (aged 18–69 years) in Nauru, Tukelau and Tuvalu (WHO, 2018). The questionnaire was administered in face-to-face interviews (WHO, 2018). The ethics committees of the Department or Ministry of Health of Nauru, Tukelau and Tuvalu approved the study, and the study participants provided written informed consent (WHO, 2018).
Measures
Outcome variable
PD was measured with the Kessler PD Scale (K10) and defined as 20–50 scores, 10–19 no, 20–24 mild, 25–29 moderate and 30–50 severe PD (Kessler et al., 2002). Cronbach alpha for the K10 ranged from 0.80 in Nauru to 0.90 in Tuvalu in this survey.
Sociodemographic data included number of years of formal education, age, sex and marital status.
Alcohol family problems in the past 12 months were assessed with the item, ‘During the past 12 months, have you had family problems or problems with your partner due to someone else’s drinking?’ (WHO, 2018).
Heart attack/stroke was self-reported by asking about the history of a ‘heart attack or chest pain due to heart disease (angina) or a stroke (cerebrovascular accident or incident)’.
Health risk behaviours included current smoking, current heavy episodic drinking (defined as past month intake of ⩾6 standard alcoholic drinks of 60 g pure alcohol in one session), perception of extent of salt consumption, fruit/vegetables intake per day, and based on the ‘Global Physical Activity Questionnaire’ (Armstrong & Bull, 2006), sedentary behaviour (coded ‘<4 hours, 4 to <8 hours and 8 or more hours per day’) and high, moderate and low physical activity (WHO, 2018).
Data analysis
Data were analysed with STATA software version 15.0 (Stata Corporation, College Station, Texas, USA), considering the complex study design. Pearson chi-square statistics were used to test for differences in proportions. Logistic regression was used to assessed the determinants of PD by country and pooled data. Multinomial regression was applied to estimate mild PD and moderate to severe PD by sex of pooled data. p < .05 was accepted as significant, and missing values were discarded.
Results
Characteristics of the sample
The pooled sample included 3,088 18–69 years (Median = 36 years, IQR = 27–50), 1,382 from Nauru, 554 from Tukelau and 1,152 from Tuvalu. Alcohol family problems were the highest in Mauru (27.1%), as well as heart attack or stroke (20.1%), too much salt consumed (35.0%) and high sedentary behaviour (34.8%), while current smoking (60.7%) was the highest in Tukelau, as well as heavy drinking (41.0%), and high physical activity (69.1%); further details are shown in Table 1.
Weighted characteristics in Nauru, Tukelau, Tuvalu, and pooled, 2014–2015.

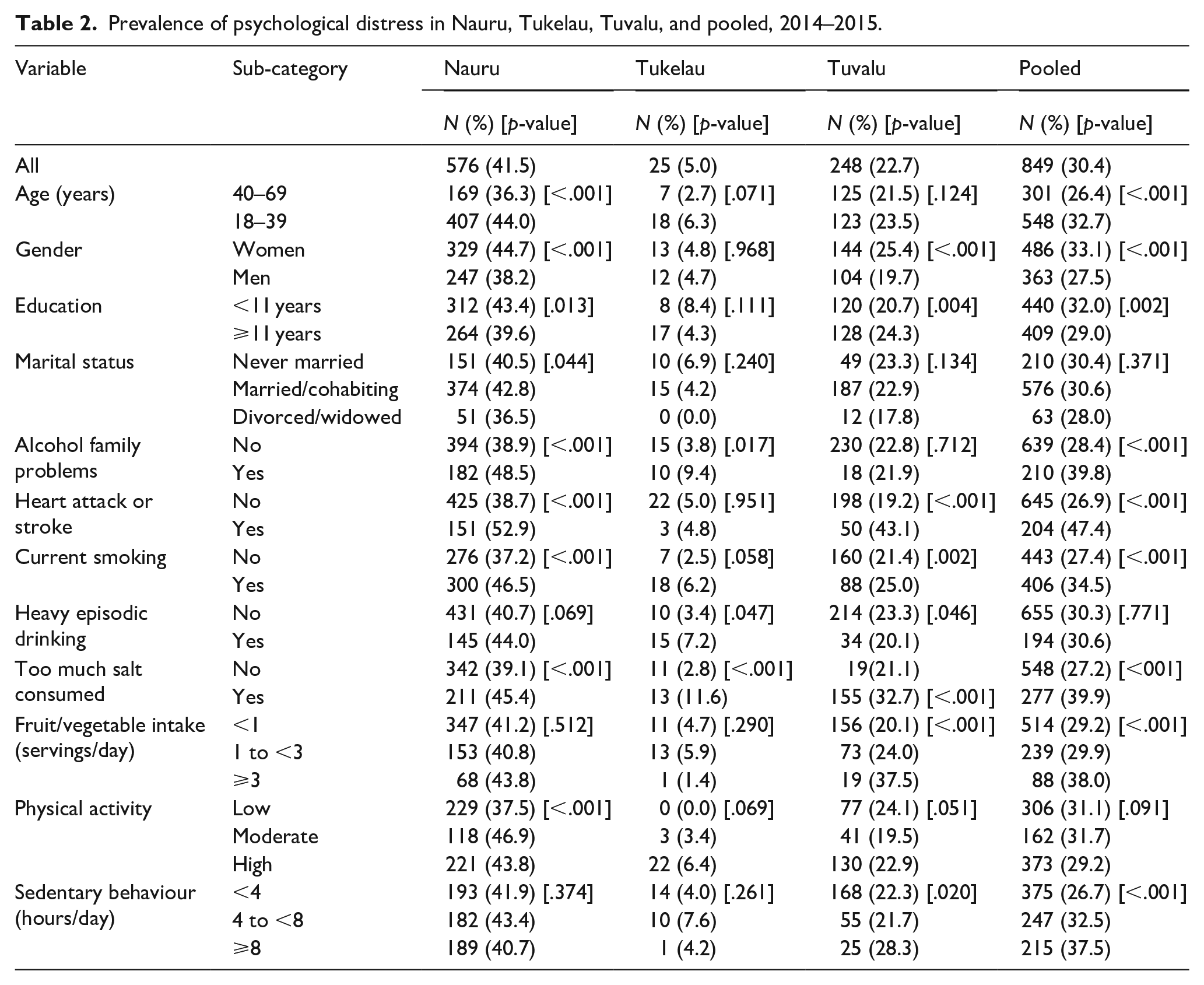
In the pooled sample 30.4% of participants had PD (⩾20 scores), 18.1% mild (20–24 scores), 7.8% moderate (25–29 scores) and 4.4% severe (30–50 scores) PD. The prevalence of PD in Nauru was 41.5%, in Tukelau 5.0% and in Tuvalu 22.7%. In the pooled sample, the prevalence of PD was higher among the younger age group (18–39 years), among women, those with lower education, those with alcohol family problems, had a history of heart attack/stroke, were currently smoking, consumed too much salt, ate 3 servings of fruit and vegetables and higher sedentary behaviour (see Table 2).
Prevalence of psychological distress in Nauru, Tukelau, Tuvalu, and pooled, 2014–2015.
Associations with psychological distress
In the adjusted logistic regression analysis with the pooled sample, younger age (18–39 years), heart attack/stroke, alcohol family problems, current smoking, high salt intake and high sedentary behaviour were positively associated with PD, while male sex and being from Tukelau and Tuvalu were negatively associated with psychological distress. In addition, higher fruit and vegetable intake was in Nauru and heavy episodic drinking was in Tukelau positively associated with PD (see Table 3).
Associations with psychological distress (⩾20 scores) in Nauru, Tukelau, Tuvalu, and pooled, 2014–2015.
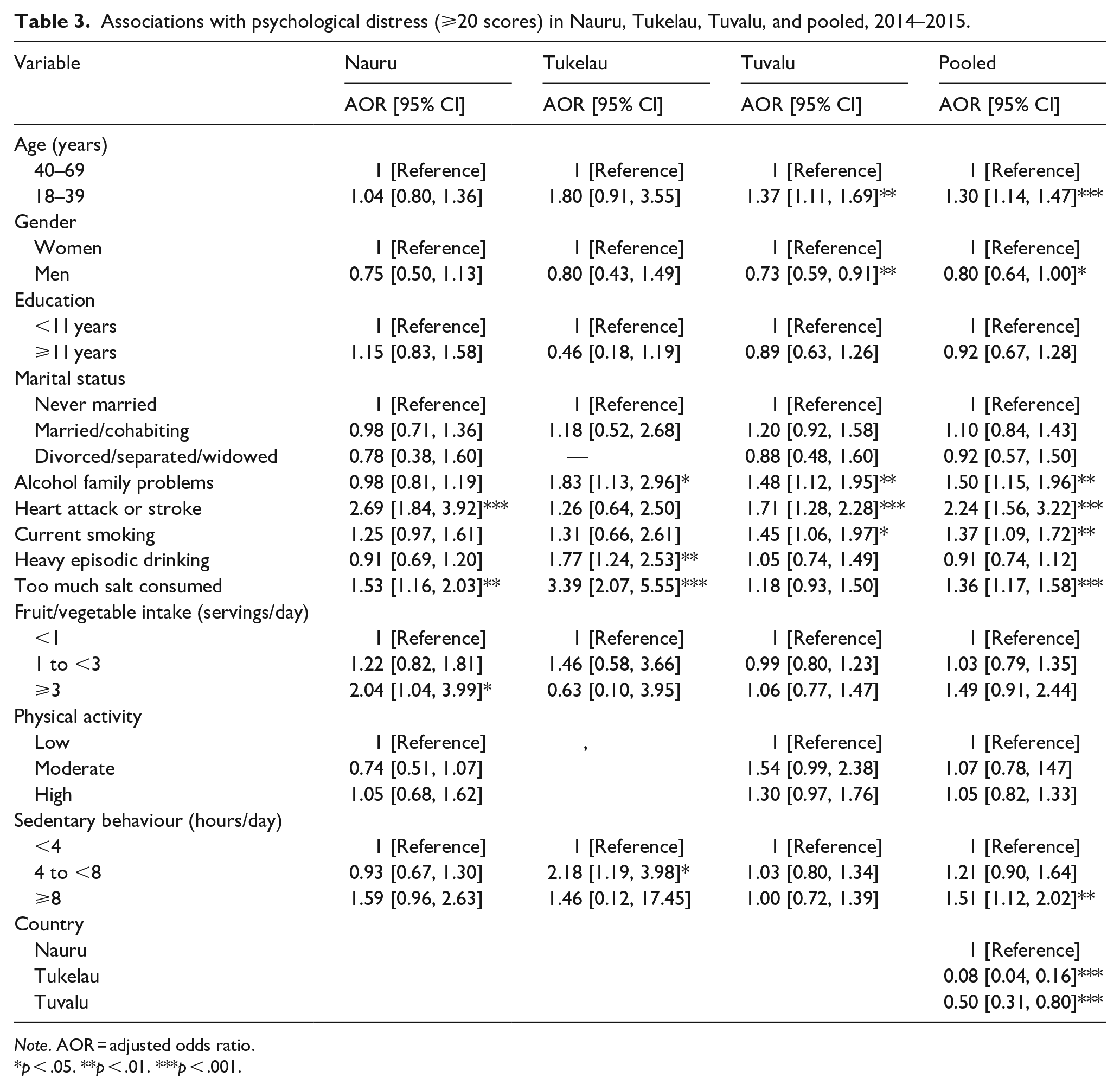
Note. AOR = adjusted odds ratio.
p < .05. **p < .01. ***p < .001.
Multinomial logistic regression with mild and moderate/severe psychological distress
In the adjusted model, among men and women, younger age, alcohol family problem, sedentary behaviour and heart attack/stroke increased the odds of mild and/or moderate/severe PD. Among women, current smoking and too much salt consumed, and among men higher fruit/vegetable intake and heavy episodic drinking were positively associated with mild and/or moderate/severe PD (see Table 4).
Multinomial logistic regression with mild and moderate-severe psychological distress by sex pooled data, 2014–2015.
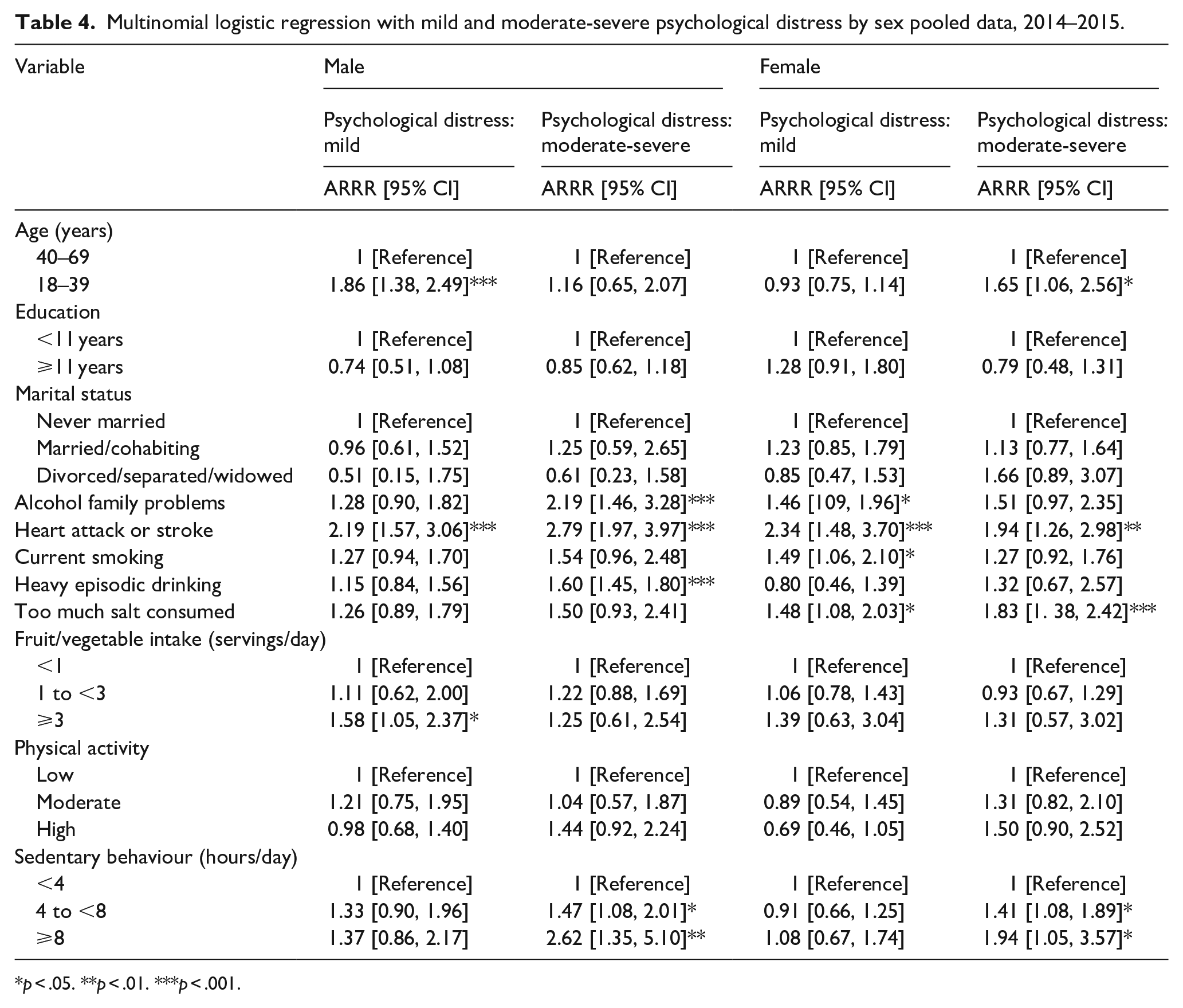
p < .05. **p < .01. ***p < .001.
Discussion
The prevalence of PD differed among adults in the three studied small countries in Oceania, ranging from 41.5% in Nauru to 5.0% in Tokelau (average 30.4%) and was higher than in Solomon Islands (18.9%) (Pengpid & Peltzer, 2021b), in Kiribati (18.1%) (Pengpid & Peltzer, 2021a), other middle-income countries, such as in South Africa (23.9%) (Mthembu et al., 2017), and high-income countries, including Australia, Canada and Japan (Caron & Liu, 2011; Enticott et al., 2016; Sakurai et al., 2010). PD may be prevented and controlled by improving or expanding mental health care into general health services as well as increasing community and family support (Bachmann, 2018; Maukera & Blignault, 2015; Orotaloa & Blignault, 2012). In Nauru, only one mental health outpatient facility attached to a hospital exits (WHO, 2017), and in Tuvalu only four mental health professionals (3 psychologists and 1 social worker, no mental health nurses, no psychiatrists) (WHO, 2022). However, in Tuvalu mental health is functionally integrated into primary care in terms of pharmacological and psychological interventions for mental health conditions and primary care workers have been trained on managing of mental disorders (WHO, 2022).
Consistent with a study in Australia (Chittleborough et al., 2011), the study found the younger population (18–39 years) had higher odds of PD, and in line with several other studies (e.g. Kuriyama et al., 2009; Mthembu et al., 2017), female sex was associated with PD. Unlike some former studies (Enticott et al., 2016; Mthembu et al., 2017; Pengpid & Peltzer, 2021b; Takeuchi & Speechley, 1989), we did not find an association between not married, lower education and PD.
We found that having a history of heart attack/stroke was associated with PD, which is consistent with previous studies (e.g. Chittleborough et al., 2011; Kuriyama et al., 2009; Lui et al., 2018). The possible higher degree of disability in people with a history of a cardiovascular event may lead to higher PD (Caponnetto, 2018). This study found a positive association between current tobacco use and among men heavy episodic drinking with PD, which concurs with former research (e.g. Chittleborough et al., 2011; Kuriyama et al., 2009; van der Deen et al., 2011). It is possible that participants self-medicate with substance use to cope with PD, ‘perpetuating psychosocial distress and reinforcing the anxious or depressive symptoms related to emerging distress syndrome’ (Walter et al., 2005).
Contrary to previous studies (Cockerman et al., 2006; Richard et al., 2015), we found that higher fruit/vegetable intake was positively associated with PD among men and in Nauru. It is possible that the overall very low rate of fruit and vegetable intake hindered the protective effect of fruit and vegetable consumption against PD (Richard et al., 2015). Contrary to a study among men in Japan (Shimizu, et al., 2015) that found an inverse association between daily salt intake and PD, we found a positive association between perceived high salt intake and PD. On the other hand, some studies point to the role of excessive salt intake in the induction of severe inflammatory reactions which in turn influence the pathophysiology of neuropsychiatric disorders (Abdoli, 2017).
In agreement with previous research (Chu et al., 2018; Pengpid & Peltzer, 2019; Sloan et al., 2013), we showed that high sedentary behaviour was associated with PD but we did not find an association between low physical activity and PD, as found previously (Chu et al., 2018; Pengpid & Peltzer, 2019; Sloan et al., 2013). In particular among women sedentary behaviour contributed to PD, emphasising the need of physical activity to possibly having beneficial effects on mental health (Hoare et al., 2016).
Study limitations
The study limitations included the cross-sectional nature of the study and the self-reporting of data. PD was assessed with a screening instrument and future studies may include at least on a sub-sample psychiatric interviews. In addition, history of adverse life events and mental disorders would be included. Due to high rate of missing values, physical, and biochemical measurements and household income were excluded from in the analysis.
Conclusion
This study found among national populations of 18–69 years in three small Pacific Island countries that almost one in three participants had PD (⩾20 scores), with the highest in Nauru (two in five participants). Several factors associated with PD were identified, such as being from Nauru, younger age (18–39 years), female sex, alcohol family problems, heart attack/stroke, current smoking, high salt intake and high sedentary behaviour, that can aid in the prevention of PD in the three small Pacific Islands populations.
Footnotes
Acknowledgements
This paper uses data from the Nauru (2015–2016), Tukelau (2014) and Tuvalu (2015) STEPS surveys, implemented by the Department or Ministry of Health with the support of the World Health Organization.
Authors’ contributions
All authors fulfil the criteria for authorship. SP and KP conceived and designed the research, performed statistical analysis, drafted the manuscript and made critical revision of the manuscript for key intellectual content. All authors read and approved the final version of the manuscript and have agreed to the authorship and order of authorship for this manuscript.
Data availability statement
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.