
Abstract
Peer support arrangements involve peers without disabilities providing academic and social support to students with severe disabilities (i.e., students eligible for their state’s alternate assessment) in general education classrooms. We conducted a systematic literature review of studies published through 2016 to determine whether peer support arrangements meet Council for Exceptional Children (CEC) criteria as an evidence-based practice. From our review of 11 studies, we found that peer support arrangements are an evidence-based practice for promoting social interactions for secondary students with severe disabilities in both core academic and elective classes. Evidence for increased academic engagement of students with severe disabilities is mixed, and evidence for other outcomes is promising—including increased academic engagement for peers who provide support. We provide recommendations for teachers.
Keywords
The field of special education has emphasized the importance of evidence-based practices for over a decade. However, some teachers remain unfamiliar with the concept of evidence-based practice, and others report implementing practices with little or no empirical support (Burns & Ysseldyke, 2009). Moreover, teachers of students with severe disabilities are often tasked with selecting instructional strategies appropriate to address the widely varying needs of their students—a challenge that grows as students enter middle and high school, and are enrolled in a wider range of classes. Secondary educators struggling to effectively support students with severe disabilities in inclusive settings may turn to unproven models of support, such as overdependence on paraprofessional support—a practice that may have an inadvertent negative impact on students’ social outcomes (Giangreco, 2010). Efforts to ensure the implementation of evidence-based practices must target useful, practical educational practices with high-quality empirical support and ensure that the information is accessible to practitioners (Carnine, 1995). Bridging this research-to-practice gap necessitates commitment by researchers to the clear evaluation and synthesis of research to determine for whom, for which outcomes, and under what conditions evidence-based practices are effective.
The Council for Exceptional Children (CEC) established standards for evidence-based practices. These standards provide a framework for evaluation and synthesis of special education research, as well as guidelines for categorizing practices based on the strength of supporting evidence (CEC, 2014). Not only are these standards widely accepted as an effective means of establishing evidence-based practices, their application to research on educational practices for students with severe disabilities is particularly fitting. CEC’s guidelines include quality indicators designed to identify studies that are methodologically sound and sufficient to establish a causal relation between practices and student outcomes. In addition, CEC’s categorization of practices as evidence based, potentially evidence based, having mixed evidence, having insufficient evidence, or resulting in negative effects provides guidance for educators beyond a dichotomous distinction of evidence based or not evidence based. Identification of evidence-based and promising practices for students with severe disabilities is especially critical, given the relative scarcity of evidence-based practices currently identified for this population. For example, in a systematic review of interventions for students with autism, Wong and colleagues (2015) identified 27 evidence-based practices, yet authors reported only 22 and 19 practices with research support for use with students in middle and high school, respectively. In a similar review of instructional practices to teach academics to students with severe disabilities, Spooner, Knight, Browder, and Smith (2011) found the use of time delay to teach both chained and discrete responding to be evidence based but only identified 12 and six studies of sufficient quality, that included middle school and high school students, respectively.
It is critically important for researchers to apply CEC’s standards to the research literature to guide educators struggling to identify the best instructional strategies to meet the diverse educational needs of students with severe disabilities. Practitioners equipped with an understanding of which practices have the most empirical support—even when the most promising practices do not quite meet the rigorous standards required for an evidence-based practice—are better able to design educational programs with potential to optimize student outcomes. However, the challenges faced by educators do not stop at identifying evidence-based practices. They are also tasked with matching evidence-based practices to student’s educational needs, targeted outcomes, and the wide range of educational contexts in which students participate throughout their school day. For educators to make well-informed decisions, researchers must review research evidence to determine for which students, for which outcomes, and under what conditions evidence-based practices are most effective.
In this systematic review, we focus on applying CEC’s standards to the research base supporting the efficacy of peer support arrangements for students with severe disabilities. Peer support arrangements involve one or more peers trained to provide social, academic, and behavioral support to middle and high school students with severe disabilities in general education classrooms (Carter, Moss, Hoffman, Chung, & Sisco, 2011). Specifically, Carter and colleagues (2015) outline clear, replicable steps for implementing peer support arrangements, including (a) an individualized plan designed for the student with severe disabilities and his or her specific general education classroom, (b) an initial training for one to three peer partners, and (c) ongoing adult facilitation as peer partners provide both social and academic support during ongoing class activities. The primary purpose of this intervention is to improve social interactions and class participation as students sit and work alongside each other with regular monitoring, guidance, and feedback provided by an adult facilitator (e.g., paraprofessional, general educator, special educator). A qualified general or special education teacher should develop the individualized plan, and should direct and closely supervise any paraprofessional implementation. Although peer support plans—like any effective practice for students with severe disabilities—provide flexibility for individualization, researchers have clearly defined and measured the implementation steps associated with this practice (e.g., Biggs, Carter, & Gustafson, 2017; Brock & Carter, 2016; Huber, Carter, Lopano, & Stankiewicz, in press).
Although research testing the efficacy of peer support arrangements has spanned almost 20 years, researchers have yet to conduct a systematic review of the research literature to determine whether and under what conditions peer support arrangements are evidence based. Carter, Sisco, Chung, and Stanton-Chapman (2010) examined the intervention research targeting peer social interactions for students with intellectual disability and/or autism, and found substantial support for a number of peer-focused approaches, including peer interaction training, peer networks, and peer awareness training. However, the authors cited an insufficient number of studies to support peer support arrangements as an evidence-based practice, and they did not review whether studies were of sufficient methodological quality to provide support. In their review of evidence-based practices for students with severe disabilities, Browder, Wood, Thompson, and Ribuffo (2014) include peer support interventions as a recommended practice for students with severe disabilities. However, Browder and colleagues noted that their purpose was to provide a brief summary of “high-quality research” (p. 6), which did not involve systematically reviewing the literature to “make judgments about each study’s design” but instead “relied heavily on existing reviews of the literature and a few current studies” (p. 10). Both of these reviews contributed to moving the field forward, but neither was designed to address the question of whether peer support arrangements are evidence based.
Beyond the mere absence of a systematic literature review, we chose to focus on peer support arrangements for a number of reasons: First, descriptive research studies suggest that students with severe disabilities, when included in general education classrooms, rarely interact and learn alongside their peers (Feldman, Carter, Asmus, & Brock, 2016). If indeed evidence-based, peer support arrangements offer a means to improve the quality of inclusion for these students. Second, although peer support arrangements are defined by a set of core components, there is room for a great deal of flexibility in implementation. For example, researchers have selected students with different disability labels to receive support, used different strategies to select peers, and identified different classroom contexts for implementation. Although the flexible nature of this intervention is often appealing to practitioners, they need guidance to understand the conditions under which peer support arrangements are most effective. Third, models of implementation for peer support arrangement have changed over time, with more recent studies focusing on providing replicable training to school practitioners (i.e., teachers, paraprofessionals, speech-language pathologists), who then assume primary responsibility for implementation. Teachers and administrators need direction regarding how they might most effectively train facilitators to implement peer support arrangements under typical conditions.
In this systematic review, we address these issues by applying CEC’s standards for evidence-based practice to the research literature supporting peer support arrangements for secondary students with severe disabilities. Specifically, we address four questions: First, are peer support arrangements an evidence-based practice? If so, for what outcomes are they evidence based? Second, under what conditions are they evidence based? Specifically, what are the characteristics of students with disabilities and their peers who have participated in these interventions? In what kinds of classrooms did these interventions occur? Third, what type of training was required for practitioners to implement these interventions? Fourth, what innovations have been added that might hold promise?
Method
Inclusion Criteria
We required studies to meet the following criteria: First, researchers must have tested peer support arrangements as the independent variable. We define peer support arrangements as including these key components: (a) one or more peers without developmental disabilities provide support to a student with a diagnosis of intellectual disability, autism spectrum disorder (ASD), or multiple disabilities in a middle or high school general education class; (b) a written plan is developed detailing individualized strategies for support based on the needs of the student with a disability and the classroom context; (c) support is focused on promoting both social and academic outcomes; (d) an adult facilitator provides initial training to peers who provide support; and (e) an adult facilitator provides ongoing support to peers. Second, researchers must have utilized an experimental design that meets CEC’s design standards (CEC, 2014). Specifically, authors must have implemented a group-comparison design comparing two treatment groups that did and did not receive the intervention, or a single-case design in which the researcher manipulated delivery of the intervention to allow for three or more opportunities to demonstrate effects.
Search Strategies
First, in September 2016 we searched PsychInfo, ERIC, and Social Sciences Abstracts databases with the following search strings: (“peer support*”) AND (severe disabilit* OR significant disability*), yielding 24 hits. We did not include any date limiters; therefore, all studies published up to September 2016 were included in this search. Next, we screened articles out based on titles and abstracts that clearly did not meet inclusion criteria, and we completed full-text review of the remaining 11 articles. During full-text review, we found that seven of the 11 articles met all inclusion criteria. Then, we performed citation searches using Google Scholar and reviewed the reference lists for these seven studies, from which we identified two additional studies. Finally, we asked the authors of included studies to identify any additional studies. They identified three studies accepted for publication but not yet in press; these studies have since been published. We conducted hand searches of Exceptional Children and Research and Practice for Persons with Severe Disabilities through the end of 2016; no additional articles were identified. Altogether, we identified 11 studies that met inclusion criteria.
Author Queries
In addition to the information in the 11 manuscripts, we queried authors in any case that we sought to code specific study characteristics not described in the manuscript. Therefore, the results include a combination of information from manuscripts and author queries. Although all authors were responsive to our queries, sometimes authors indicated that studies had occurred long enough ago that they no longer could recall information, nor were original data available.
Study Coding
CEC quality indicators
We applied the CEC (2014) quality indicators for evidence-based practices to all studies included in the review. These included 22 indicators for single-case-design studies and 24 indicators for experimental group-design studies that focus on the context and setting, participants, intervention agent, description of practice, implementation fidelity, internal validity (e.g., interrater reliability), outcome measures, and data analysis. We coded each indicator dichotomously (i.e., “yes” or “no”).
Study design
We categorized each study’s design as a single-case design or a group experimental design. We categorized each single-case design based on the designs outlined by Gast and Ledford (2014; for example, reversal, multiple-baseline across participants). We categorized each group experimental design as a randomized-controlled trial or a quasi-experimental study.
Study effects
For single-case-design studies, we used visual analysis to calculate success estimates (Reichow & Volkmar, 2010). A success estimate is not an effect size, and does not represent the magnitude of effects. It simply summarizes visual analysis of data as a ratio of the number of times an experimental effect was demonstrated (numerator) over the number of opportunities an experimental effect could have been demonstrated, given the experimental design (denominator). For group-design studies, we computed Cohen’s d. In one group-design study (i.e., Carter et al., 2016), the authors computed group differences through regression in a multilevel model and calculated effect sizes by dividing the unstandardized regression coefficient for the treatment group by the pooled standard deviation across groups. We replicated these calculations to confirm their accuracy. In a second group-design study (i.e., Asmus et al., 2016), the authors did not report effect sizes. We computed effect sizes by dividing the difference between the posttreatment means by a pooled standard deviation.
Characteristics or participants with disabilities
We recorded the numbers of students with disabilities who received support from peers. We then categorized students by (a) disability label (i.e., only intellectual disability, only ASD, both intellectual disability and ASD, or multiple disabilities when they had a combination of two or more categories other than intellectual disability and ASD); (b) gender; (c) eligibility for alternate assessment (i.e., yes, no, or unreported); (d) ethnicity (i.e., White, African American, Asian American or Pacific Islander, Hispanic, Native American, other, or not reported); and (e) school level (i.e., middle or high school). We categorized each student’s mode of communication as primarily verbal (i.e., authors describe only verbal speech, or state that verbal speech was the primary mode), primarily augmentative and/or alternative communication (AAC; i.e., authors describe only AAC, or state that AAC was the primary mode), or verbal and AAC (i.e., the authors describe both verbal speech and AAC but do not indicate a primary mode).
School and classroom settings
We coded the urbanicity of schools as urban, suburban, or rural. We recorded whether classrooms were in a middle or high school. We recorded author description of class content, and we categorized each class as core academics (i.e., math, science, language arts, or social studies) or elective and related arts (i.e., all classes that do not meet the definition of core academics). We recorded the mean and standard deviation of total students in each class across each study. If authors reported the number of students in each class but did not report a mean and standard deviation, we computed these values from the information provided.
Identification and characteristics of peers providing support
We recorded the number of peers in each study who provided support to students with disabilities. We categorized these peers by (a) gender (i.e., male or female), (b) ethnicity (i.e., White, African American, Asian American, Hispanic, Native American, or other/unreported), and (c) level (i.e., middle or high school). We developed categories to describe the basis on which peers were recruited. These categories included that peers (a) were preferred by the focus student, (b) were interested in the focus student, (c) might benefit themselves from providing support, (d) were positive role models, (e) had a history of positive interactions with the focus student, (f) had good attendance, (g) worked well with adults, (h) had good social skills, (i) had low academic engagement, and/or (j) had poor academic performance. We coded these categories based on author description, although the authors did not provide operational definitions. We did not include categories for generic descriptions (e.g., teacher thought that peer would work well with focus student) because they do not provide insight into why the teacher thought students might work well together, nor did we include a category related to peers agreeing to provide support, given that all peers must have provided their assent to participate in a research study.
Adult facilitators and their training
We coded (a) the role of the people who provided training to facilitators (e.g., researcher, special education teacher), (b) the roles of the facilitators who implemented peer support arrangements (i.e., research team, paraprofessional, special education teacher, general education teacher and/or speech/language pathologist), (c) the length of initial training delivered to a facilitator before implementation began, and (d) the number of times a trainer provided follow-up support to a facilitator after implementation began. We developed categories to describe the content of training based, including (a) overview of peer support arrangements, (b) development of peer support plan, (c) modeling facilitative strategies, (d) performance feedback on implementation, and (e) a self-monitoring checklist.
Innovations of peer support arrangements
If researchers included any other strategies in addition to or in combination with the core components of peer support arrangements (as outlined in the inclusion criteria above), we noted these innovations. Examples include structural analysis and collaborative planning with related service personnel.
Reliability of Study Coding
Both authors coded all variables, and we computed point-by-point agreement (i.e., number of agreements divided by number of opportunities for agreement). Overall agreement was 97%. Within categories of coding, agreement was 100% for study design, 92% for study effects, 97% for characteristics of students with disabilities, 97% for school and classroom settings, 97% for identification and characteristics of peers providing support, and 96% for implementation agents and their training. All disagreements were resolved through consensus.
Results
CEC Quality Indicators
Eight of the 11 studies met all the CEC quality indicators after review of the manuscript and author queries. Three articles (i.e., Cushing & Kennedy, 1997; Shukla, Kennedy, & Cushing, 1998, 1999) published prior to CEC standards in 2000 met most, but not all, quality indicators. In all three cases, the authors did not assess and report implementation fidelity, and in two cases (i.e., Shukla et al., 1998, 1999) authors did not describe training provided to implementation agents. We chose to retain these three studies for three reasons: First, four fifths of experimental special education studies published prior to 2000 are missing this type of information (Gresham, MacMillan, Beebe-Frankenberger, & Bocian, 2000), and systematically excluding older studies runs counter to the scientific process of building an evidence base by replicating similar findings over time. Second, a primary concern with missing implementation fidelity data is that poor fidelity (and not shortcomings of the intervention itself) might explain a lack of experimental effects; given that these three studies had strong positive effects, this particular concern is mitigated. Third, in most cases, inclusion or exclusion of these three studies does not affect the evidence-based classifications. In the one case their inclusion did affect an evidence-based classification, we highlighted this explicitly (see Results and Discussion).
Study Design and Effects
Data related to study design and effects are reported in Table 1. Authors utilized single-case designs in nine studies and a randomized-controlled trial in two studies. Statistically significant differences were reported across seven outcomes in one randomized-controlled trial (i.e., Carter et al., 2016), with the largest effects related to friendship gains, social goal attainment, peer interactions, and classroom participation. The second randomized-controlled trial was an underpowered pilot study (i.e., Asmus et al., 2016), so no statistically significant differences were reported; effect sizes for peer interactions and academic engagement were large, but there was no difference between groups for friendship gains. In single-case-design studies, researchers demonstrated experimental effects in 63 of 83 opportunities across four dependent variables and eight studies. Across studies, effects were most consistent for peer interactions (i.e., 37/39) and least consistent for academic engagement of students with severe disabilities (i.e., 9/22). Success estimates across other outcomes and studies included Individualized Educational Plan (IEP) goals (i.e., 2/3) and peer academic engagement (i.e., 15/19).
Study Design and Experimental Effects for Students With Severe Disabilities and Their Peers.

Note. For single-case design studies, we calculated success estimates (Reichow & Volkmar, 2010) that show the number of effects detected through visual analysis (numerator) over the number of opportunities to demonstrate effects (denominator). This is not an effect size but a summary of our visual analysis. For randomized-controlled trials, we report effect sizes as Cohen’s d. MB = multiple baseline; SCD = single-case design.
Characteristics of Participants With Disabilities
Data related to characteristics of the 85 students with disabilities who received support are reported in Table 2. Participants were mostly male (57%) and most had a diagnosis of only intellectual disability (48%). Students represented a range of ethnicities, although the majority (64%) was White. Student communication was described in terms of standardized test scores (i.e., Communication subscale of the Vineland Adaptive Behavior Scales) in randomized-controlled trials, but students’ mode of communication was not reported. Across single-case studies, students were nearly evenly split between those who communicated primarily through verbal speech (n = 11) and primarily through AAC (n = 13); some students used both modes without identification of a primary mode (n = 6). When reported, nearly all students were eligible for alternate assessment. Three studies were published prior to the federal requirement to use alternate assessment for students with severe disabilities and, therefore, did not report this information.
Characteristics of Participants With Disabilities.
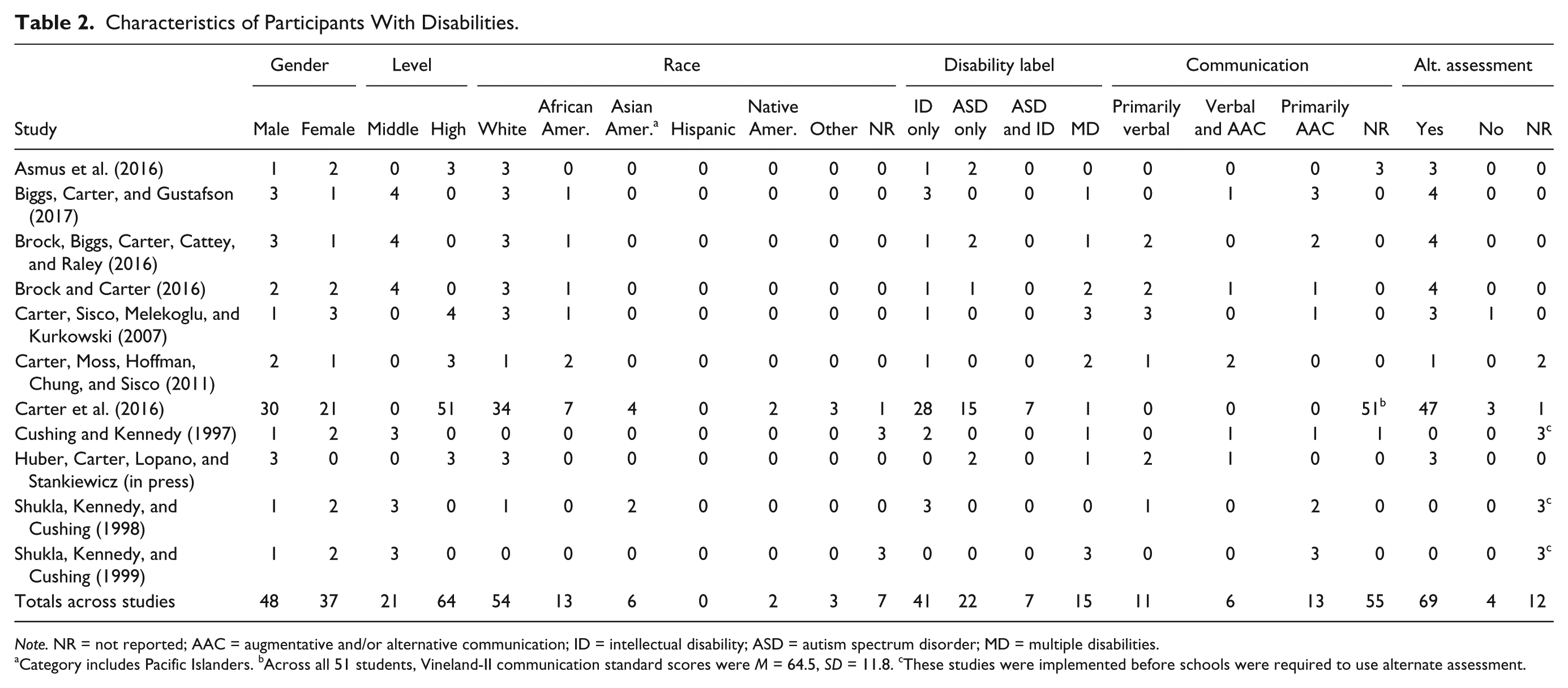
Note. NR = not reported; AAC = augmentative and/or alternative communication; ID = intellectual disability; ASD = autism spectrum disorder; MD = multiple disabilities.
Category includes Pacific Islanders. bAcross all 51 students, Vineland-II communication standard scores were M = 64.5, SD = 11.8. cThese studies were implemented before schools were required to use alternate assessment.
School and Classroom Settings
Data related to school and classroom settings are reported in Table 3. Across studies, students attended urban (six studies), suburban (seven studies), and rural (one study) schools. Studies were conducted in middle (six studies) and high schools (five studies). Students were split nearly evenly between core academic classes (n = 38) and elective and related arts (n = 47). The mean number of students per class ranged from 19 to 33 across studies.
School and Classroom Settings.

Note. NR = not reported.
Author reported range of 31 to 35 but not individual totals per classroom; therefore, mean reflects average of the minimum and maximum.
Identification and Characteristics of Peers Providing Support
Data related to identification and characteristics of the 173 peers who provided support are reported in Table 4. More peers were female (67%) than male. Similar to students with disabilities, peers represented a range of ethnicities, although the majority was White (64%). Across studies, the most common basis for selecting peers was potential benefit to peers themselves (six studies). In two studies focused primarily on peer effects, peers were selected specifically because they demonstrated poor academic engagement or performance.
Identification and Characteristics of Peers Who Provided Support.
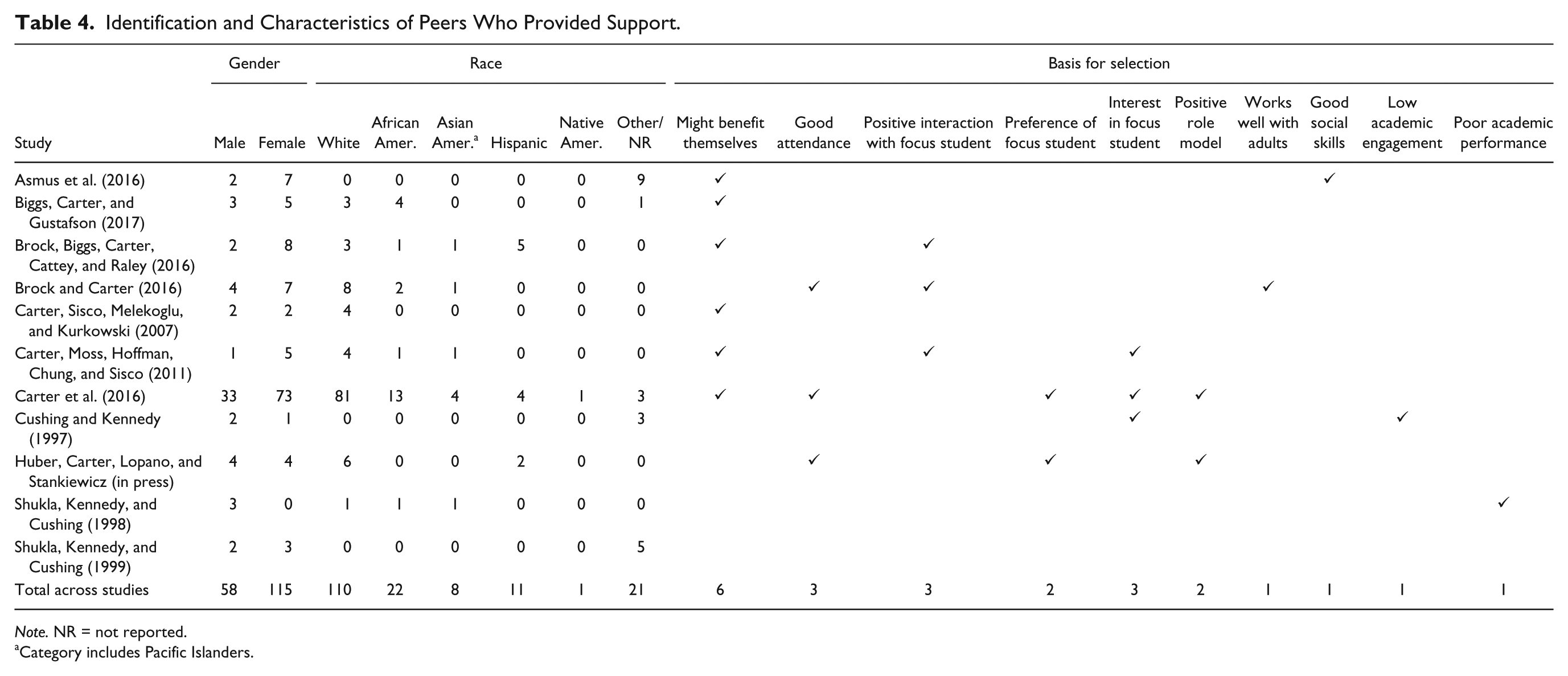
Note. NR = not reported.
Category includes Pacific Islanders.
Adult Facilitators and Their Training
Data related to adult facilitators and their training are reported in Table 5. In all studies, paraprofessionals were either the sole facilitators (five studies) or facilitated jointly with others (six studies). In all cases, paraprofessionals facilitated under the supervision of licensed special education teachers. In four studies, special or general education teachers directly facilitated with students. In two studies, research teams implemented components of the intervention alongside paraprofessionals. When reported, initial training for facilitators ranged from 1 to 4 hr, and they received 0 to 5 follow-up coaching visits. Training intensity tended to be greater when school practitioners were solely responsible for implementation. When reported, the content of training always included an overview of peer support arrangements, and often also included guided development of the peer support plan (eight studies), modeling strategies (eight studies), performance feedback on implementation (seven studies), and use of a self-monitoring checklist (seven studies). Inclusion of some training content (e.g., development of peer support plan) was contingent on whether school practitioners were responsible for that aspect of implementation. Two studies (i.e., Brock, Biggs, Carter, Cattey, & Raley, 2016; Brock & Carter, 2016) focused on special education teachers, training paraprofessionals; in all other studies, researchers delivered training.
Adult Facilitators and Their Training.
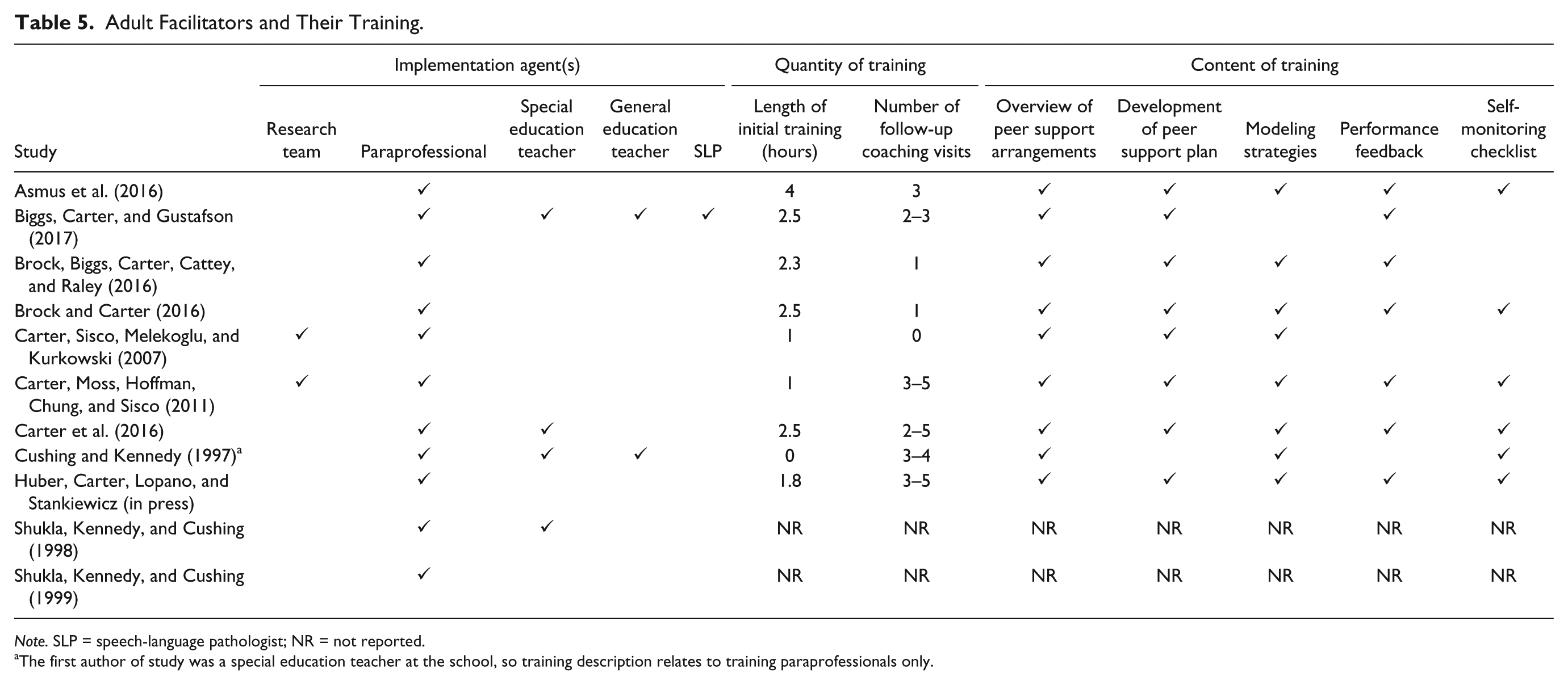
Note. SLP = speech-language pathologist; NR = not reported.
The first author of study was a special education teacher at the school, so training description relates to training paraprofessionals only.
Innovations of Peer Support Arrangements
Recent studies have introduced notable innovations. Huber et al. (in press) demonstrated that structural analysis can be used to identify and modify contextual variables (e.g., 1:1 peer support vs. working in a small group) to optimize outcomes for individual students. Biggs et al. (2017) demonstrated use of collaborative planning among educators and speech-language pathologists to create well-designed peer support plans for students with complex communication challenges.
Evidence-Based Classification
Based on our review, the research base for peer support arrangements garners different evidence-based classifications for different outcomes, per CEC’s (2014) guidelines. First, peer support arrangements are an evidence-based practice for increasing social interactions between students with severe disabilities and their peers. CEC criteria state that a practice is evidence based if supported by (a) one methodologically sound group-comparison study with random assignment with at least 30 participants, and (b) at least three methodologically sound single-subject-design research studies with positive effects and at least 10 total participants (CEC, 2014). The reviewed evidence base exceeds this criterion with one randomized-controlled trial with 51 participants and eight single-case-design studies with a combined 28 participants.
There is mixed evidence for the effects of peer support arrangements on the academic engagement of students with disabilities who received support. In randomized-controlled trials, Carter et al. (2016) and Asmus et al. (2016) demonstrated robust effect sizes for academic engagement (i.e., d = .34 and d = 1.18, respectively), but in single-case-design studies, researchers only demonstrated experimental effects in nine of 22 opportunities. When measured in single-case-design studies, the authors reported academic engagement was a secondary outcome, and the primary goal of peer support arrangements was to increase peer interactions without sacrificing academic engagement (e.g., Brock & Carter, 2016). For the nine participants in which experimental effects were demonstrated, academic engagement in the baseline condition tended to be very low (i.e., <20% of the class period), leaving more room for improvement than in other cases when baseline engagement was moderate or high.
Peer support arrangements are a potentially evidence-based practice for a number of other outcomes, including (a) social skills for students with severe disabilities, (b) attainment on individualized social goals for students with severe disabilities, (c) attainment on individualized academic goals for students with severe disabilities, (d) classroom participation for students with severe disabilities, (e) friendship gains for students with severe disabilities, and (f) academic engagement for peers who provide support. For each of these outcomes, evidence exists in the form of either one sound randomized-controlled trial or two to four methodologically sound single-subject studies with positive effects. This classification would change for one outcome (i.e., academic engagement for peers who provide support) if one excluded studies not meeting all CEC quality indicators (see “Method” section).
Discussion
Teachers need guidance about how to promote inclusion of students with severe disabilities using evidence-based practices. Although existing literature reviews provide valuable insight into peer-mediated strategies, they do not systematically analyze the research literature to determine the degree to which individual practices are evidence based. In this systematic review of the research literature, we aimed to determine the degree to which peer support arrangements are an evidence-based practice. We identified eight studies meeting all of CEC’s quality indicators and three studies published prior to development of CEC quality indicators which meet most, but not all, of these indicators. Across these 11 studies, sufficient evidence exists to support peer support arrangements as an evidence-based practice for promoting social interactions between students with severe disabilities and their peers. Evidence related to other outcomes is promising or mixed. These findings make a number of key contributions to the literature.
First, sufficient evidence has accumulated to deem peer support arrangements an evidence-based practice for promoting social interactions between students with severe disabilities and their peers in general education classrooms. These effects were replicated across 82 middle and high school students with a range of disability labels (i.e., intellectual disability, autism, both intellectual disability and autism, and multiple disabilities), and across both core academic and elective classes. Success estimates across single-case-design studies show high consistency of effects, and a moderate effect size from a fully powered randomized-controlled trial (i.e., Carter et al., 2016) equates to 25 additional interactions with peers during a 50-min class period. Given that many students with severe disabilities have extremely limited opportunities for interactions with their peers (Feldman et al., 2016), an intervention with such consistent and sizable effects represents an exciting avenue for improving social outcomes for this population.
Second, there is mixed evidence related to whether peer support arrangements promote academic engagement for students with severe disabilities. We think these mixed effects can be explained by four factors: study design, baseline performance, normative rates of engagement, and quality of direct support from paraprofessionals. In all cases in which effects were not demonstrated, researchers implemented single-case-design studies in which the primary outcome was social interactions, and the secondary outcome was academic engagement. Because decisions regarding introduction of the independent variable were based on analysis of social interactions and not academic engagement data, there are instances in which (a) stable baseline patterns were not established before the independent variable was introduced, and/or (b) a clear effect was not demonstrated before the independent variable was introduced for the subsequent participant in a multiple-baseline experiment. In these cases, treating academic engagement as the primary intervention outcome might have produced additional effects.
In addition, heterogeneous levels of academic engagement across participants in the baseline condition likely played a role in mixed outcomes. Across individual students, mean baseline academic engagement was as low as 2% of observed intervals (i.e., Bridget in Carter et al., 2011) and as high as 73% (i.e., Destiny in Brock & Carter, 2016). In most cases in which effects were demonstrated in single-case-design studies, students had extremely low levels of baseline engagement. Perhaps there is a ceiling effect for students with higher levels of engagement, making it relatively difficult to improve this outcome.
Another consideration is the normative rate of engagement. In three studies (i.e., Asmus et al., 2016; Carter et al., 2016; Huber et al., in press), researchers established normative rates of academic engagement for randomly selected classmates without disabilities. They found normative rates of engagement as low as 25% in some classes. They suggest that it might be most appropriate to gauge academic engagement of students with severe disabilities relative to normative comparisons, which seem to be extremely variable across classrooms. Also relevant is the quality of support provided by special education staff during the baseline condition. Across studies, all students received direct support from a special educator or paraprofessional during baseline. If special education staff are already providing highly effective academic support, it would be unreasonable to expect peer support arrangements to produce a marked increase in academic engagement. In these cases, the goals of peer support arrangements are to promote social outcomes and fade adult support while maintaining a high level of academic engagement.
Third, peer support arrangements are a potentially evidence-based practice for a number of outcomes, including promoting academic engagement for peers who provide support. The potential to improve outcomes for peers runs counter to a common (but unsubstantiated) concern that tasking peers to provide support might jeopardize their academic success. Indeed, two studies suggest that intentionally selecting peers with poor academic engagement or performance to provide support may be an avenue for improving these outcomes. Although outcomes for peers who already had high academic engagement and performance have not been as clearly documented, peer responses from social validity questionnaires across the included studies suggest that most peers perceive their experiences to be enjoyable and rewarding.
Fourth, more recent studies illustrate potential avenues for training practitioners to effectively facilitate peer support arrangements. In particular, Brock and Carter (2016) and Brock et al. (2016) provide clear descriptions of how special educators might train and support paraprofessionals to facilitate peer support arrangements and provide evidence to support the efficacy of the training model. This training model included an initial 2- to 2.5-hr training session in which special educators provided an overview of peer support arrangements, guided development of a peer support plan, and modeled facilitation strategies. In addition, teachers observed paraprofessionals at least once in the general education classroom to provide performance feedback and model facilitation strategies in context. In Brock and Carter (2016), paraprofessionals also used a self-monitoring checklist to remind them to use specific facilitation strategies. Other recent studies (e.g., Biggs et al., 2017) have adopted similar approaches for effectively training adult facilitators. Collectively, these studies provide a validated blueprint for how to promote effective implementation of peer support arrangements. Furthermore, a recent practitioner-oriented publication outlines all implementation steps (i.e., Carter et al., 2015).
Implications for Practice
Findings from this review have important implications for educators. Middle and high school general educators, special educators, and paraprofessionals should collaborate to implement peer support arrangements as part of a larger plan to promote the inclusion of students with severe disabilities in general education classrooms. We emphasize that paraprofessionals should only deliver support under the close direction and supervision of teachers. Teachers should (a) provide clear directions about how to implement peer support arrangements, (b) lead the development of the peer support plan, and (c) observe paraprofessionals and provide positive and corrective feedback about their facilitation (Brock et al., 2016). If teachers are unable to observe in person, an alternative is to have the paraprofessional share a video recording with the teacher at another time (e.g., Brock & Carter, 2016). Collaboration across special education teachers, general education teachers, and related service personnel can enhance the quality of peer support plans (Biggs et al., 2017). In addition, structural analysis may provide a means to further individualize peer supports and optimize outcomes (Huber et al., in press).
Our findings suggest that peer support arrangements are an evidence-based practice for promoting social interactions between students with severe disabilities and their peers. Although this approach might improve academic engagement for students who have very low baseline levels, evidence for this outcome is mixed, and other supports should be utilized to ensure academic engagement and progress on the general education curriculum. In addition, educators might consider selecting peer partners who might benefit themselves from providing support. Educators in the included studies often selected peers on this basis, and in some cases these peers improved their own academic engagement or performance as a result of providing support.
Limitations and Future Directions for Research
Some limitations of this review highlight potential future directions for research. First, we used success estimates to descriptively characterize the effects of single-case-design studies detected through visual analysis. Although the two authors of this study had a very high rate of agreement using this established and validated approach, visual analysis is inherently subjective, and it is possible other researchers might have made different judgments. Second, the studies in this review were conducted by a small number of authors. All studies include Dr. Craig Kennedy, Dr. Erik Carter, and/or one of their previous students as an author. Although current CEC criteria (2014) do not address the degree to which evidence should be provided by multiple research groups, guidelines by Horner et al. (2005) suggest at least three investigative teams and three geographic locations. We encourage other researchers to replicate and build on this research to establish an even more robust evidence base. Third, we included three studies that were published prior to development of CEC quality indicators and did not meet all of these indicators. However, we have made a case for why these studies should be included, and highlighted the one instance in which inclusion of these studies affected an evidence-based classification. Fourth, we were authors on some of the reviewed studies. However, we took steps to ensure objectivity, such as independently coding all variables before coming to consensus. Finally, there has been limited study of the degree to which effects from peer support arrangements generalize to other settings. In only one study did researchers address this issue, and they found limited generalization of peer interactions (Brock et al., 2016). Additional studies are needed to better understand generalization of effects.
Conclusion
Peer support arrangements are an evidence-based practice for promoting social interactions between students with severe disabilities and their peers in middle and high school general education classrooms. Furthermore, recent studies have demonstrated promise for several innovations. These innovations include use of structural analysis to identify and modify contextual variables to optimize student outcomes, and collaborative teaming across educators and a speech/language pathologist to ensure plans support complex communication needs. Given these promising innovations, there is reason to believe that future research might enable educators to further optimize this evidence-based practice to maximize benefits for both students with severe disabilities and their peers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.