
Abstract
Deaths occurring among agitated or violent individuals subjected to physical restraint have been attributed to positional asphyxia. Restraint in the prone position has been shown to alter respiratory and cardiac physiology, although this is thought not to be to the degree that would cause asphyxia in a healthy, adult individual. This comprehensive review identifies and summarizes the current scientific literature on prone position and restraint, including experiments that assess physiology on individuals restrained in a prone position. Some of these experimental approaches have attempted to replicate situations in which prone restraint would be used. Overall, most findings revealed that individuals subjected to physical prone restraint experienced a decrease in ventilation and/or cardiac output (CO) in prone restraint. Metabolic acidosis is noted with increased physical activity, in restraint-associated cardiac arrest and simulated encounters. A decrease in ventilation and CO can significantly worsen acidosis and hemodynamics. Given these findings, deaths associated with prone physical restraint are not the direct result of asphyxia but are due to cardiac arrest secondary to metabolic acidosis compounded by inadequate ventilation and reduced CO. As such, the cause of death in these circumstances would be more aptly referred to as “prone restraint cardiac arrest” as opposed to “restraint asphyxia” or “positional asphyxia.”
Keywords
Introduction
Physical restraint is used by law enforcement officers (LEOs) and health-care workers when dealing with people who are aggressive, uncooperative, or violent. Deaths have been reported during physical restraint of agitated individuals held in the prone (facedown) position, as detailed in case reports, case series, and inquests.1–13 However, the actual physiologic cause of death in these circumstances remains uncertain. There is currently controversy regarding the role of positional asphyxia as the primary factor underlying restraint-associated mortality.
Asphyxia is defined as a state of impaired oxygen intake and the accumulation of excess carbon dioxide that results in loss of unconsciousness and often leads to death. Asphyxia typically results from physical interference with the mechanics of breathing (i.e., inhalation, exhalation, and ventilation) and/or respiration (i.e., cellular exchange of oxygen and carbon dioxide). 14 In cases of compression asphyxia, the physical act of ventilation is impaired or prevented by compression due to an external force on the chest and/or abdomen. 15 The definition of death from positional asphyxia involves three specific criteria: (a) evidence that the individual’s body position interfered with or prevented ventilation or normal gas exchange, (b) evidence that the individual was unable to move to another position, and (c) clear exclusion of other causes of death based on finding from autopsy. 2
Restraint procedures currently in use include “hogtie restraint” in which the subject’s wrists are handcuffed behind their back with ankles strapped (hobbled), also known as the prone maximal restraint position (PMRP). 16 Other physical restraint procedures include (a) physically restraining the extremities while an individual is held in a prone position, and (b) placing downward pressure on a subject’s back (a weight force (WF)) while in the prone position. Individuals who expired while held in these restraint positions meet the previously defined criteria for positional asphyxia and their postmortem diagnosis can be referred to as restraint asphyxia.5,16
Epidemiological studies have revealed that deaths due to prone restraint are rare, and occur approximately two to three times a year in regions that include Los Angeles, 6 Ontario in Canada, 17 and England and Wales. 18 Other studies, including one carried out over a seven-year period in western Canada 19 and another one-year study that involved 11 agencies across the USA, 20 reported no deaths, despite the frequent use of prone restraint in cases involving police custody. These two studies led the authors to conclude that prone restraint was associated with no clinically significant effects 19 and that this method was safe. 20 Indeed, the authors of three independent textbooks stated clearly that there is no significant physiologic evidence indicating that force used on subjects held in the prone position results in significant respiratory compromise that could lead to asphyxia and death.16,21,63
The precise role of physical restraints and their impact on respiratory physiology and cardiac output (CO) remain unclear. While many experimental settings have attempted to reproduce the impact of prone restraint and PMRP, these experiments were typically performed on healthy volunteers. By contrast, agitated individuals may be in a state of preexisting metabolic acidosis. Restraint in the prone position may exacerbate this state via inadequate ventilation and a decrease in CO. These physiologic derangements can lead to pulseless electrical activity (PEA) and asystolic cardiac arrest.
In this review, the results of several published studies that report the effects of prone restraint on respiratory physiology and CO are reviewed. The review also focuses on the physiology of physical activity and secondary metabolic acidosis that has been reported in individuals with acute behavioral disturbances. Several alternative theories that may explain the cause of death in individuals subjected to prone restraint are also presented. Taken together, this consideration of the published literature explores the hypothesis that prone restraints may not be universally safe, and supports efforts to limit their use.
Methods
A literature search of PubMed, Medline, and Google Scholar was performed to identify all English language manuscripts published between 1980 and August 2020. Keywords used included positional asphyxia, postural asphyxia, restraint asphyxia, sudden death custody, sudden death restraint, excited delirium, acute behavioral disorder, physiological restraint death, and prone position adverse effects. Publications included were those that focused on both medical science and clinical aspects associated with deaths related to prone restraint with particular reference to positional or restraint asphyxia. Citation lists within these publications were searched and reviewed for additional source material. This information was used to build and to expand on an earlier review of the adverse effects of physical restraint by Barnett et al. 22 and also included studies that focused on metabolic acidosis and the impact of physical prone restraint on circulatory physiology.
Ventilation
Basic physiology
Contraction of the diaphragm is responsible for about two thirds of the air that enters the lungs during relaxed breathing (Figure 1). 23 During deep inspiration, the diaphragm can descend by as much as 10 cm. 23 Individuals in a prone position can experience an increase in intra-abdominal pressure, which limits the space available for movement of the diaphragm and expansion of the chest cavity, thereby decreasing ventilation.1,3 The prone position also restricts expansion of the ribs and external intercostal muscles, likewise limiting the expansion of the chest cavity (Figure 2).3,4,6
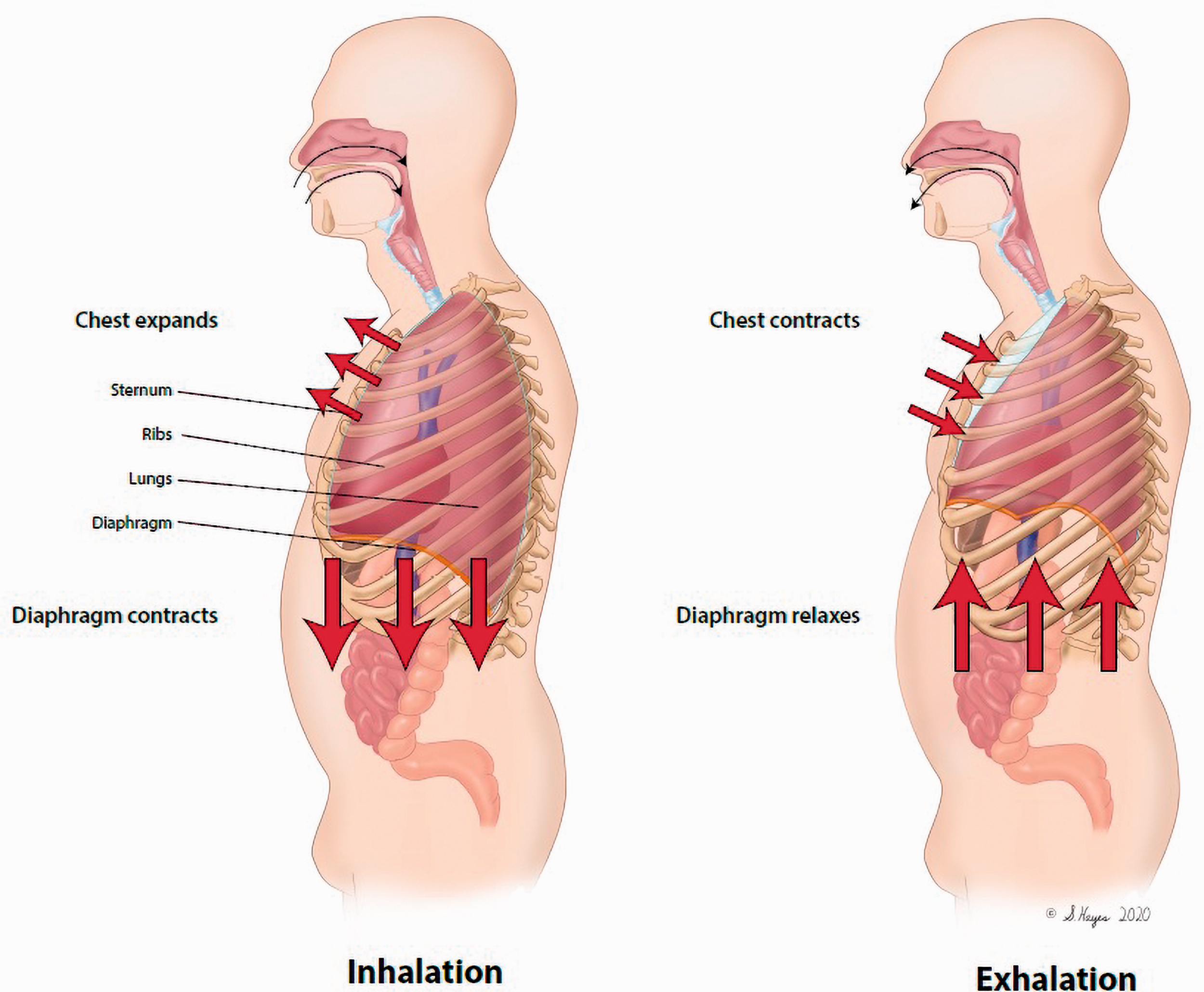
Normal breathing. Diaphragm expanding into abdomen and rib expansion are important components. (Illustrations by Suzanne Hayes.)
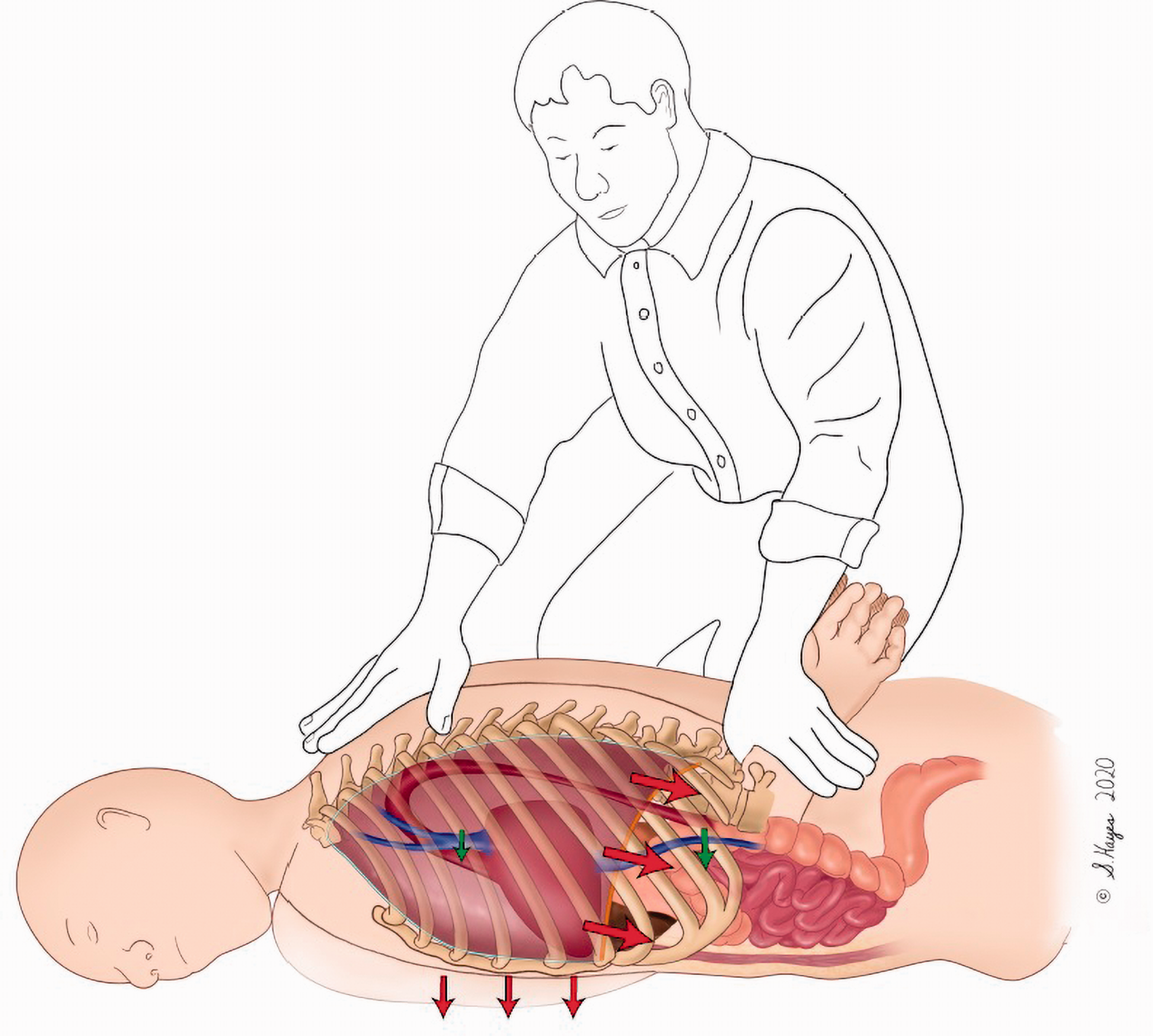
Prone restraint leads to an increase in intrathoracic pressure, thus reducing venous return. Decreased rib expansion also reduces ventilation. Prone restraint also increases intra-abdominal pressure, which compresses the low pressure inferior vena cava, thereby decreasing venous return. Lastly, intraabdominal compression also limits diaphragm expansion and decreases ventilation.
Several studies published in the medicolegal literature have focused on attempts to replicate prone restraint situations to assess an individual’s capacity for ventilation under these conditions (Table 1).24–31 These experimental models are limited by their inability to replicate real-world conditions and the chaotic situations in which prone restraint would ordinarily be applied. Most subjects in these experiments were healthy and not in a “fight-or-flight” or a fearful state that would most likely prevail during a confrontation with an LEO or health-care worker.
Ventilatory capacity in prone and restrained prone subjects.
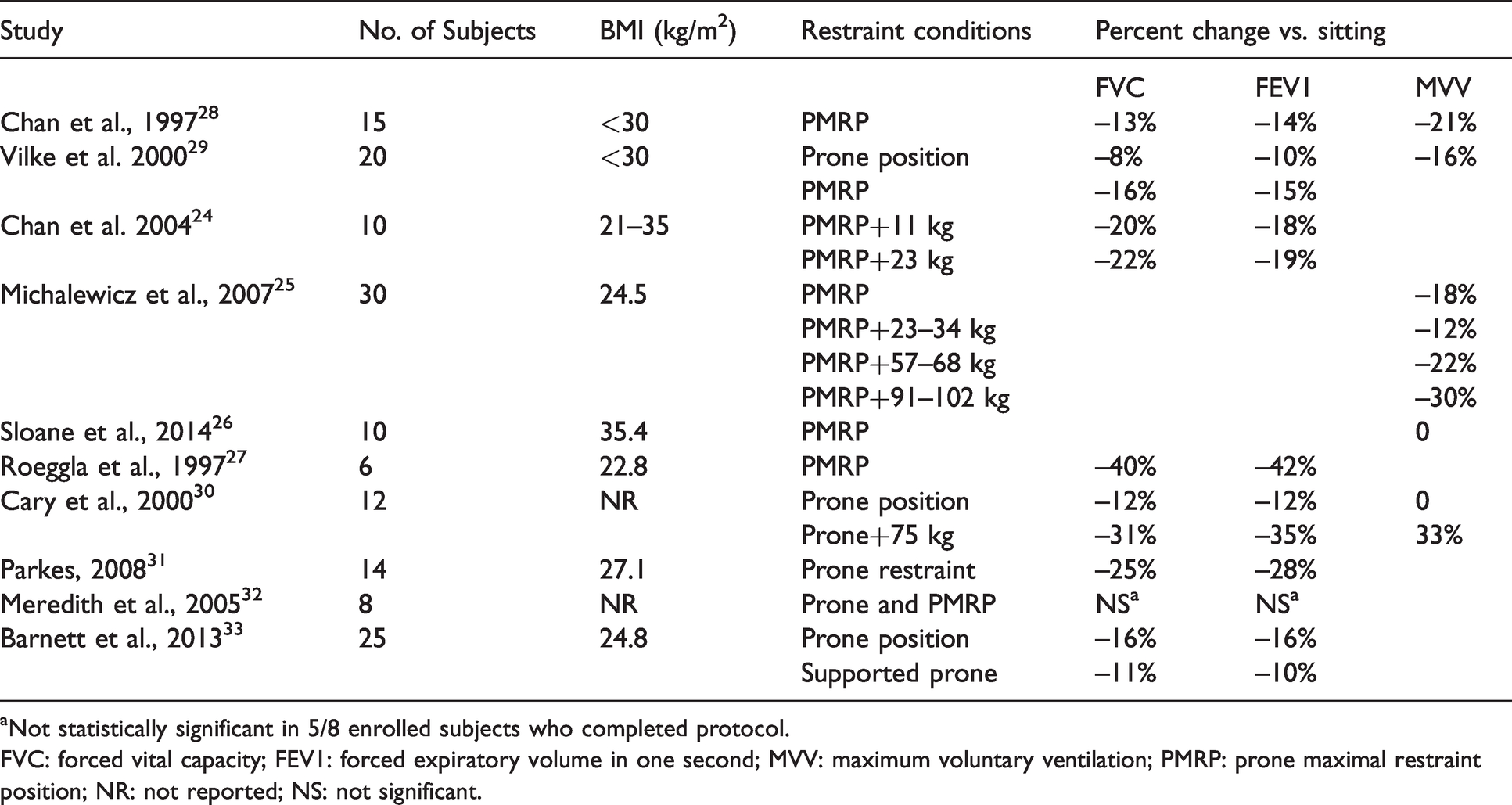
aNot statistically significant in 5/8 enrolled subjects who completed protocol.
FVC: forced vital capacity; FEV1: forced expiratory volume in one second; MVV: maximum voluntary ventilation; PMRP: prone maximal restraint position; NR: not reported; NS: not significant.
Pulmonary function tests
Pulmonary function tests (PFTs) are a set of clinical evaluations that document how well the lungs are functioning at a given moment in time. Forced vital capacity (FVC) is the amount of air an individual can exhale in a single breath. Forced expiratory volume (FEV1) is the amount of air an individual can exhale rapidly in the first second of exhalation. 23 ,34,35 Maximum voluntary ventilation (MVV) measures the largest volume of air that can be moved by voluntary effort in one minute. Individuals undergoing MVV testing are instructed to breathe rapidly and deeply for 12–30 seconds; the volume is then measured in liters per minute. 35 MVV can be used to estimate breathing reserve during maximal exercise and can provide an estimate of respiratory muscle endurance and fatigue. 35
Research studies from the University of California, San Diego
One research group at the University of California San Diego (UCSD) has published several studies that assessed ventilatory capacity in prone patients.24–26,28,29 Changes in PFTs were detected, although these findings were deemed as not clinically significant by the authors. The first study enrolled 15 healthy volunteers who were evaluated with PFTs while sitting, supine, prone, and in the PMRP after four minutes of exercise on a bicycle. The authors reported a 13% drop in baseline FVC, a 14% drop in baseline FEV1, and a 21% drop in MVV in participants in the PMRP when compared to responses from the same individuals evaluated while in a sitting position. 28 A second study from this group measured PFTs in the sitting, supine, and prone positions in 20 healthy men. The authors reported statistically significant reductions in PFT results, including an 8% reduction in FVC, a 10% reduction in FEV1, and a 16% reduction in MVV among participants in the prone position compared to the sitting position. 29
A third study from this group enrolled 10 healthy males with no exercise performed. As part of this study, FVC and FEV1 were determined at baseline, at one minute, and at five minutes while individuals assumed one of four positions (sitting, PMRP, or PMRP with 25 or 50 lb weights placed on the subject’s back). PFTs performed on participants held in the PMRP revealed a 16% drop in FVC and a 15% drop in FEV1 compared to results obtained in sitting position. PMRP plus a 25 lb weight resulted in reductions of 20% and 18% in FVC and FEV1, respectively, while PMRP with the added 50 lb weight resulted in losses of 22% and 19%, respectively. 24 End-tidal CO2 levels remained <45 mmHg (within normal limits) throughout the entire study.
A fourth study that included 30 healthy subjects measured MVV without FVC or FEV1 in five positions (sitting, PMRP, PMRP with an added low weight (LW; 23–34 kg (50–75 lb)), PMRP with added medium weight (MW; 57–68 kg (125–150 lb)), and PMRP with added high weight (HW; 91–102 kg (200–225 lb)). When compared to results obtained at a baseline seated position, MVV dropped 18%, 12%, 22%, and 30% among participants evaluated in the PMRP, PMRP with LW, PMRP with MW, and PMRP with HW, respectively. 25 The authors of this study concluded these changes were not clinically significant because the results of all PFTs remained >80% of the predicted normal range. However, it is critical to recognize that an earlier report from the American Thoracic Society/European Respiratory Society task force established that short-term changes in PFTs >12% are usually statistically significant and may be clinically important. 35
A fifth study from the UCSD group focused on obese subjects with an average body mass index (BMI) >35 kg/m2. 26 Prior UCSD studies had only included subjects with a BMI <30 kg/m2.24,25,28,29 Participants exercised on a bicycle until reaching 85% of their age-predicted maximal heart rate. MVV was then measured at 5, 10, and 15 minutes after exercise while participants were seated, prone, or in the PMRP. No significant positional changes were noted with respect to MVV, heart rate, oxygen saturation, or end-tidal CO2; FVC, FEV1, and respiratory rate were not included in the report. 26 These findings, which include no change in MVV in this experimental setting, conflict with the other studies carried out by the same group with non-obese participants in which results included reductions in MVV in the prone position, 29 in the PMRP 28 as well as PMRP with added weight burden. 25 These findings seem to be at odds with what might be expected physiologically, as obesity is associated with a higher degree of intra-abdominal compression, which would result in diminished ventilation while in the PMRP. One possible explanation is that rapid, shallow breathing compensated effectively for decreased lung volume, thus resulting in no change in MVV. The end-tidal CO2 reported post exercise was ∼20% below baseline, reflecting a normal compensation of ventilatory-associated respiratory alkalosis. However, no significant change in end-tidal CO2 was noted when comparing outcomes between these three positions—a finding that would be expected with no apparent change in MVV.
Other published trials
Several published trials from other groups identified significant decreases in lung capacity among participants held in a prone position and the PMRP.27,30,31 Roeggia et al. placed six healthy young males in a prone restraint position for three minutes and found that their FVCs and FEV1s dropped by 40% and 42%, respectively, from initial measurements; this decrease was described as “dramatic.” 27 These authors also reported that end-tidal CO2 increased by 14.7% among participants held in a prone restraint position. Likewise, Cary et al. evaluated the responses of 12 healthy subjects of unknown weight. 30 Subjects exercised by cycling until they reached 85% of their age-predicted maximal heart rate. Subjects were then tested during the post-exercise period while seated, in prone positions, and in the prone position with a 75 kg (165 lb) added weight burden placed across each subject’s back. Among their findings, the participants’ FVCs dropped by 12% while in the prone position and by 31% while in the prone position with the added 75 kg weight burden, while FEV1s dropped 14% and 35%, respectively. MVVs did not change significantly among participants in the prone position but dropped by 33% among participants in the prone position with the added 75 kg weight burden. The authors concluded that these findings represented “marked reductions” in ventilatory capacity.22,30 Parkes reported an average 25% drop in FVC and a 28% drop in FEV1 in a cohort of 14 healthy volunteers positioned in prone restraint. These findings were described as “significant.” One participant in this study experienced a 57% drop in FEV1. 31
Other published studies include that of Meredith et al., who examined PFTs in eight individuals (ages 45–80 years) with chronic obstructive pulmonary disease who were in prone the position and PMRP. Three of the eight participants were unable to tolerate the prone position due to clinical symptoms and deterioration. No statistically significant changes in FVC or FEV1 were identified among the five participants who completed the study protocol. The authors concluded that response to the prone position and PMRP varied on a case-by-case basis. 32 In another study, Barnett et al. reported that the prone position imposed pressure on the anterior chest and thereby restricted lung function. The participants in this study experienced a 16% decrease in FVC and a 16% decrease in FEV1 while in the prone position. Decreases in FEV and FEV1 were reduced to 11% and 10%, respectively, in what was described as a “supported prone” position that reduced pressure on the anterior chest. 33
Kroll et al. estimated that the application of a 260 kg (570 lb) weight will result in a flail chest, which is a major cause of acute fatal compression asphyxia. 36 This initial observation was followed by an evaluation of WF applied to prone mannequins by an LEO with three different single-knee techniques and one double-knee technique. 37 This group reported that the application of a single knee creates an average WF of 23.7–32.9 kg, independent of the weight of the LEO. The double-knee technique created a WF that was 23.3 kg plus 24% of the weight of the LEO. As such, the authors concluded that force typically applied by LEOs on subjects held in a prone position was safe and did not support the concept of restraint asphyxia.
Ventilation studies with individuals held in the PMRP both with and without added weights revealed no significant changes in blood oxygenation.24,25,27,30 At rest, the ratio of alveolar ventilation to pulmonary blood flow (the V/Q ratio) is normally ∼0.84. During intense physical activity, alveolar ventilation increases disproportionately to blood flow; the V/Q ratio may ultimately exceed 5.0 to ensure adequate aeration and oxygenation of blood. 38 As such, the decrease in ventilation noted in the aforementioned studies would be unlikely to result in hypoxia.
Prone positioning and mechanical ventilation
The recent coronavirus disease pandemic has resulted in increased awareness of prone positioning with respect to the treatment of patients who require mechanical ventilation for acute respiratory distress syndrome (ARDS). Prone positioning has been shown to improve oxygenation in patients with severe hypoxemia. As such, this intervention is likely to reduce mortality among patients with severe ARDS when it is applied for at least 12 hours a day. 39 Prone positioning may improve oxygenation in this patient cohort and prevent ventilator-induced lung injury by reducing overinflation while promoting alveolar recruitment. As such, prone positioning would serve to normalize the distribution of stress and strain within the lungs. 40 While undergoing mechanical ventilation, these patients are anesthetized and provided with a fixed volume (i.e., no decrease in the prone position) together with positive end-expiratory pressure (PEEP). In these cases, the diaphragm acts as a passive membrane. 41 The positive effects of prone positioning on regional blood flow and ventilation are substantially greater in patients under general anesthesia and those provided with PEEP than they are in patients who remain awake and capable of breathing spontaneously. 42 In other words, while prone positioning may serve to improve oxygenation of mechanically ventilated ARDS patients, these findings are not relevant to healthy unsedated subjects placed in prone restraint.
Cardiac output
Basic physiology
CO is the volume of blood pumped by the heart per unit time and is the product of heart rate and stroke volume. 38 The cardiac index (CI) is the CO divided by the body surface area. CO has a direct impact on oxygen and CO2 transport to and from the muscles during physical activity. The amount of oxygen that the body utilizes is the product of the CO and oxygen extraction (i.e., the arteriovenous oxygen difference). 38 A decrease in CO will result in decreased oxygen delivery to the muscles, including the heart and the lungs, and will reduce the amount of oxygen that can be utilized. A decrease in CO will also reduce the rate and amount of CO2 delivery to the lungs and result in diminished pulmonary blood flow and perfusion.
CO and prone position
The prone position generates an increase in intrathoracic pressure, thereby decreasing venous return (Figure 2) to the heart and thus decreasing CO. 38 The prone position can also lead to abdominal restriction and obstructed blood flow in the compliant inferior vena cava (IVC), thereby reducing preload and CO. IVC flow in the resting supine position represents ∼20–30% of total CO. 43 This value increases to ∼45% of total CO during supine leg exercise. 44 Patients who have undergone an IVC ligation experience a 45% reduction in CO in response to exercise compared to normal controls. 45 One recent publication reported the case of a patient who developed shock secondary to acute IVC occlusion. 46
Research studies
A study from the UCSD group enrolled 25 healthy subjects that were placed in five positions: supine, prone, PMRP, PMRP with an additional 50 lb of weight placed on the back, and PMRP with an additional 100 lb of weight placed on the back. No PFTs were performed. Vital signs, CO, and CI were determined by echocardiography, and IVC diameters were measured. No statistically significant changes in these parameters were noted, except the CI underwent a 16% drop upon addition of the 50 lb weight, and the IVC diameter dropped by 19% in response to the addition of the 100 lb weight (Table 2). 47
Cardiac output and IVC diameter changes in restrained prone subjects.
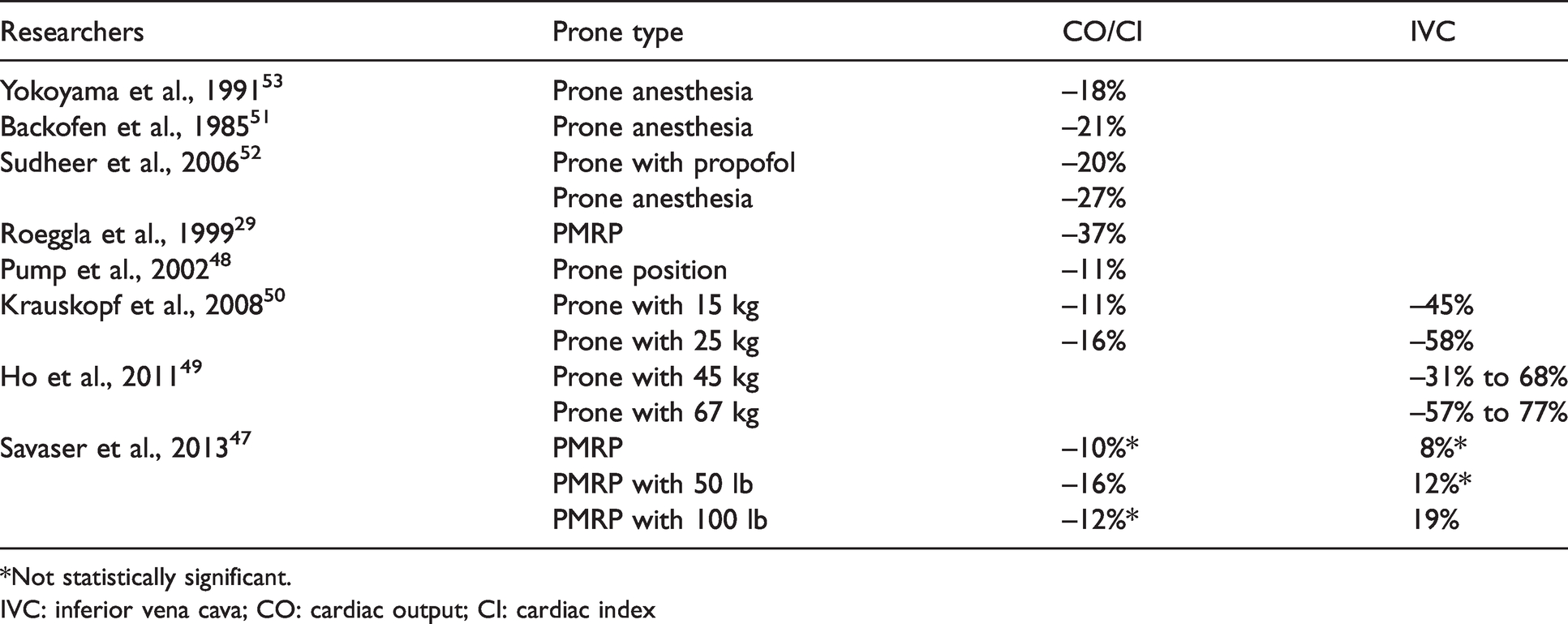
*Not statistically significant.
IVC: inferior vena cava; CO: cardiac output; CI: cardiac index
By contrast, results from studies carried out by other groups revealed significant decreases in CO and IVC diameter under similar conditions. For example, Roeggia et al. reported a 37% drop in CO in patients held in prone restraint. The observed decrease in CO was attributed to reduced venous return through the IVC to the heart. 27 Likewise, in a study involving 14 healthy volunteers, Pump et al. reported an 18% decrease in stroke volume and an 11% decrease in CO among participants in an unrestrained prone position. 48 Furthermore, Ho et al. evaluated IVC diameters in 25 healthy subjects during standing, prone, prone restraint with an additional 45 kg (100 lb) placed on each participant’s back, and prone with an additional 67 kg (147 lb) placed on each participant’s back. 49 Compared to standing, prone with the addition of the 45 kg weight resulted in significant reductions of 42% and 68% in the minimal longitudinal and transverse diameters, respectively, while the maximal diameters were reduced by 31% and 35%, respectively. The addition of the 67 kg weight also resulted in significant 77% and 74% reductions in minimal longitudinal and transverse diameters, respectively, with maximal diameters reduced by 57% and 45%, respectively. 49 No CO values were reported. Finally, Krauskopf et al. studied responses to weights applied to the lower torsos of six healthy, non-obese volunteers, five of whom were noted to be athletic. Application of 15 lb to the lower torsos of each subject when in the prone position resulted in a 45% reduction in IVC diameter, a 69% reduction in maximal IVC blood flow, and an 11% decrease in CO. Application of 25 lb to the lower torso resulted in a 58% reduction in IVC diameter, an 80% reduction in maximal IVC blood flow, and a 16% reduction in CO. The results of this study revealed significant IVC compression and decreased CO among participants placed in the prone position with added weights. 50
CO during surgical procedures
Surgeons often perform procedures on patients placed in a prone position. This position has been evaluated in publications focused on anesthesia, and revealed decreases in CO that ranged from 17% to 26%.51–53 Diminished CO has been attributed to reduced venous return, direct effects on arterial filling, and reduced left ventricular compliance secondary to increased thoracic pressure. IVC compression is a recognized complication that can occur in patients placed in a prone position during surgery and has been reported to be exacerbated by abdominal compression. 54
Physical activity and metabolic acidosis
Basic physiology
Physical activity increases the metabolic rate in working muscles, increases ventilation, and augments CO. Oxygen consumption is measured in units of metabolic equivalents of task (METs), which defines the rate of oxygen consumption per minute. 55 For example, skipping rope at 84 times a minute, rowing a distance of 8 km/h, or ambulating at a rate of 3.4 mph with a 14% grade consume oxygen at 10 times the baseline rate (i.e., 10 METs). The relative maximum intensity and energy that can be used, a value known as the VO2 max, reflects the absolute intensity of METs. 38
During physical activity, ventilation, oxygen extraction, and CO all increase to meet the acute demand for oxygen consumption. In normal adults, the resting minute ventilation of 5–6 L/min can be increased 20- to 25-fold to 150 L/min during short periods of maximal exercise. 23 Likewise, respiratory rates can increase from 16–20 to 40–50 breaths per minute. Ventilation and CO both increase linearly with oxygen consumption during exercise. The increases in ventilation develop more rapidly to maintain physiologic pH under conditions that promote the production and release of lactic acid. CO does not increase to the same extent as ventilation and can undergo maximal increases of four- to sixfold over the resting CO level.23,34 The increase in venous return observed in response to deeper inspiratory efforts and extravascular compression by muscles used during exercise together with a decrease in venous capacitance all contribute to an increased stroke volume. Oxygen consumption (VO2) is the product of CO and the oxygen arteriovenous oxygen difference. Although increased oxygen use and extraction result in a significant drop in venous oxygen levels, arterial oxygen levels are maintained.
Conditions associated with metabolic acidosis
Psychotic or agitated behavior secondary to a psychiatric condition or illicit stimulant abuse may incite a state in which an individual may be unable to cooperate with LEOs or health-care workers. Individuals in these altered states are less likely to cease exertion due to fatigue and may resist and struggle while in restraint. These activities can result in a high-output state requiring significant increases in ventilation, CO, and oxygen extraction.
Metabolic acidosis can occur during intense exercise and can result from an increased reliance on non-mitochondrial ATP turnover. 56 Blood pH levels as low as 6.8 have been reported in association with exhausting exercise. 38 In a study of 12 subjects designed to simulate physical resistance to an LEO, Ho et al. found that just 45 seconds of heavy bag physical resistance exercise resulted in a reduction of blood pH from 7.36 (physiologic) to 7.04, together with a significant increase in epinephrine, norepinephrine, dopamine, and total catecholamine levels. 57 Interestingly, blood pH remained low (at 7.06) at 10 minutes post exercise. Hick et al. described five individuals who sustained cardiac arrest while in the custody of LEOs and were found to have severe acidosis (pH range 6.25–6.81). 58 Individuals in psychotic or delirious states may have altered sensation, and as such, they may continue to exert themselves beyond normal physiologic limits. While in this state, metabolic acidosis signals a significant compensatory increase in ventilation, thus resulting in a secondary respiratory alkalosis. Hick et al. theorized that prone placement and restraint may impede the development of the critical compensatory respiratory alkalosis—a problem that may ensue in response to a mere 20% reduction in ventilatory capacity. 58
During heavy physical activity, ventilation is no longer linked as tightly to oxygen demand. Instead, ventilation is connected directly to CO2, hydrogen ion (H+), and lactate anion concentrations that stimulate and regulate respiratory function and ventilation. 38
Post-exercise syncope
Muscle contraction during exercise is a critical factor that promotes venous return to the heart. 38 An individual who is held in restraint may result in a significant decrease in venous return, with pooling of blood in the extremities, resulting in reduced CO. Post-exercise syncope or loss of consciousness is a condition thought to be due to a sudden reduction in muscle activity resulting in decreased venous return. This may initiate a neurocardiogenic response and a drop in systemic blood pressure.59,60 This paradoxical response may contribute to deaths observed in individuals who have developed severe metabolic acidosis. However, there were no reports of a significant drop in blood pressure or syncope among any of the individuals who participated in studies involving exercise with prone restraint.24,28,30
Effects of prone restraint on the physiology of an individual with metabolic acidosis
Prone restraint has been shown to limit ventilation due to a decrease in pulmonary volumes in a restrictive pattern.24,27–31,33 As stated previously, decreased ventilation has no significant impact on arterial oxygen level. However, CO2 has a direct effect on this response to ventilation (Figure 3).
23
The process of the respiratory system responding to pH changes in peripheral circulation is known as respiratory regulation. Two specific mechanisms connect ventilation and pH via the partial pressure of CO2 (pCO2). The first relationship is based on the fact that PaCO2 (arterial partial pressure of CO2) is directly proportional to VCO2 ((CO2 production))/Va (alveolar ventilation)).23,34 If one assumes that CO2 production is constant, a decrease in ventilation will result in a net increase in arterial CO2. For example, a 20% decrease in ventilation will generate a 25% increase in PaCO2. The second relationship is based on the equilibrium between acids and bases as defined by the Henderson–Hasselbalch equation (below) and the fact that acidity or pH is directly related to pCO2:

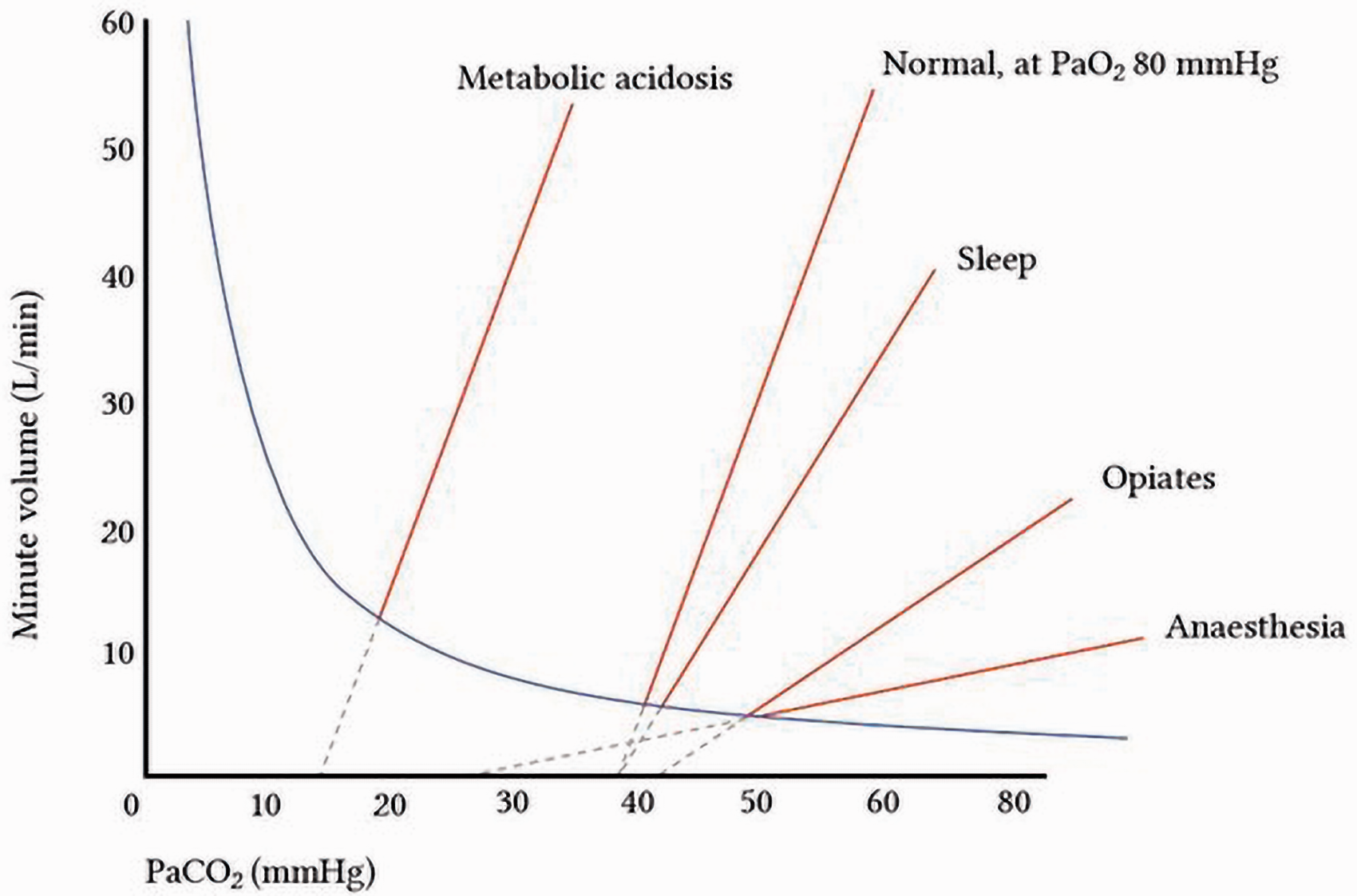
Direct relationship of minute volume ventilation to PaCO. (From Levitsky. 23 )
Given this relationship, a 25% increase in arterial pCO2 would (as per the Henderson–Hasselbalch equation) result in a decrease in pH by 0.1.23,34 As such, decreased ventilation in a person who may have already be in a state of severe metabolic acidosis can have a catastrophic outcome. Reduced ventilation will serve to exacerbate the acidosis and thereby promote autonomic instability with secondary PEA or asystole. 61
Reduced CO in an individual with preexisting severe metabolic acidosis may also result in severe negative outcomes due to decreased delivery of CO2 to the lungs. A decrease in CO will also reduce oxygen flow to the muscle tissue during a situation that requires significant oxygen demand and extraction. Given these observations, the decrease in CO observed among individuals held in prone restraint may be sufficient to cause death.
Reconsideration of current terminology
The terms “restraint asphyxia” and “prone asphyxia” do not provide a correct description of this condition because positional and/or restraint-associated limitations on breathing and gas exchange represent only part of the problem. This condition should be renamed “prone restraint cardiac arrest.” Cardiac arrest in this setting is due to a combination of factors, including a state of high oxygen demand, a need for increased CO2 removal, and significant metabolic acidosis, along with the significant decrease in both ventilation and CO. Indeed, restraint in the prone position added to preexisting metabolic acidosis represents a potential physiologic catastrophe.
Alternative theories
Alternative theories have been postulated to explain deaths occurring in individuals held in prone restraint. While many of these theories focus on cardiac conditions, there is usually no evidence of significant cardiac pathology reported on autopsy. 1,3,5,6,8 Individuals with normal cardiac structural anatomy do at times experience sudden cardiac death (SCD) during or immediately after a stressful event. 64 These events have been linked to various cardiac disorders.62,65–67 Among these disorders, channelopathies are a group of conditions associated with the dysfunction of ion channels located in the cardiac cell membranes, including prolonged QT interval, catecholaminergic ventricular tachycardia, and arrhythmogenic right ventricular dysplasia. Increased activity of catecholamines and adrenergic receptors that will occur during an altercation may provoke ventricular arrhythmias in these individuals. Stress-induced Takotsubo cardiomyopathy, a condition characterized by catecholamine-induced myocardial stunning and weakening of the heart muscle, may also predispose an affected individual to ventricular arrhythmias. Coronary artery spasm may lead to ventricular arrhythmias and subsequent death in individuals with structurally normal hearts. Some SCD events have been linked to psychiatric drugs, as the use of these medications can lead to a prolonged QT interval and ventricular arrhythmias called torsades de pointes. Sudden death has been associated with left ventricular hypertrophy on autopsy—a condition known to give a predisposition to ventricular arrhythmias. As a group, these potential underlying causes of SCD have been associated primarily with the induction of ventricular tachycardia or ventricular fibrillation and not with PEA or asystole, which are most often identified in cases of restraint cardiac arrest. Taken together, results from several case series revealed that <10% (3/38) of those studied experienced an initial ventricular arrhythmia that contributed to the etiology of cardiac arrest. By contrast, most individuals experienced either asystole (22/38) or PEA (13/38).5,6,58 These findings do not support the theory that primary cardiac mechanisms are the major etiologies of sudden death in restraint cardiac arrest.
While it is recognized that ventricular tachycardia and ventricular fibrillation will eventually deteriorate to asystole or PEA, the median time noted for this transition is estimated at 31 minutes. At 12 minutes, 90% of these cases had not undergone degradation to asystole. 68 In these cases, cardiac arrest was witnessed by LEOs, with emergency medical services arriving shortly thereafter. As such, it is safe to assume that asystole or PEA reported at the time of diagnosis most likely represented the initial rhythm disturbance. Of note, the delay associated with the need to release restraints and to place paddles or patches to assess cardiac rhythm has been estimated at 30–190 seconds. 6
Discussion
Asystole and PEA are the primary arrhythmias associated with the “4Hs and 4Ts,” including hypoxia, hypo-/hyperkalemia, hydrogen ion (acidosis), hypo-/hyperthermia, hypovolemia, tension pneumothorax, cardiac tamponade, thrombosis (coronary and pulmonary), and toxins (poisoning). 69 These conditions have reversible causes and require specific treatments. Asystole and PEA are commonly observed in cardiac arrests associated with asphyxia and metabolic acidosis. 61 Even with the application of cardiopulmonary resuscitation, advanced cardiovascular life support, and treatment of reversible causes, the probability of survival after asystole or a PEA-associated cardiac arrest is extremely low (currently estimated at 4.4%). 70 Lower pH values detected post-cardiac arrest have been associated with comparatively lower rates of survival. 71 As such, the best management practices focus on both prevention and treatment of the “4Hs and 4Ts” in an effort to avoid cardiac arrest. Put plainly, it is important to identify potentially vulnerable subjects who might present with metabolic acidosis and to refrain from the use of prone restraint. Multiple studies reviewed in this article revealed that the prone restraint position can decrease ventilation and CO, which together can lead to death in a subject who is at risk.
Physical restraint has been identified as a powerful contributor to death in subjects who are agitated and in excited states. 72 A recent article reviewed 38 sudden deaths during restraint by Dutch police over a 12-year period. The causes of death in these cases were deemed as multifactorial. However, 94.7% of subjects were noted in the prone body position, and 76.3% of subjects received thoracic pressure. 73 The clear association between the use of prone restraint and death has led to logical recommendations by physicians, paramedics, and the police in the UK.74–76 These recommendations include the use of sedation, de-escalation, minimal time in restraint, and avoidance of the prone position when called on to attend to individuals who are experiencing acute behavioral disturbances. One hopes that the USA will adopt similar recommendations so that catastrophic events, such as the recent death of George Floyd, might be prevented in the future.
Conclusion
Some authors have concluded incorrectly that prone restraint has no significant impact on respiratory or hemodynamic physiology and is not a mechanism underlying death. However, a careful review of all published findings suggests that sudden death in agitated individuals who are restrained in the prone position is most likely due to metabolic acidosis exacerbated by inadequate ventilation and a decrease in CO. These physiologic derangements can lead to a PEA or asystolic cardiac arrest. These deaths have been traditionally attributed to “positional asphyxia.” However, given the associated metabolic and physiologic changes, the findings reviewed here lead to the conclusion that death in this setting might be more aptly described as “prone restraint cardiac arrest.” Sedation, de-escalation, ensuring minimal time in restraint, and overall avoidance of the prone position in cases of acute behavioral disturbances may serve to prevent prone restraint cardiac arrest in highly vulnerable subjects.
Supplemental Material
sj-pdf-1-msl-10.1177_0025802420988370 - Supplemental material for Prone restraint cardiac arrest: A comprehensive review of the scientific literature and an explanation of the physiology
Supplemental material, sj-pdf-1-msl-10.1177_0025802420988370 for Prone restraint cardiac arrest: A comprehensive review of the scientific literature and an explanation of the physiology by Alon Steinberg in Medicine, Science and the Law
Supplemental Material
sj-pdf-2-msl-10.1177_0025802420988370 - Supplemental material for Prone restraint cardiac arrest: A comprehensive review of the scientific literature and an explanation of the physiology
Supplemental material, sj-pdf-2-msl-10.1177_0025802420988370 for Prone restraint cardiac arrest: A comprehensive review of the scientific literature and an explanation of the physiology by Alon Steinberg in Medicine, Science and the Law
Footnotes
Declaration of conflicting interests
The author has been a paid medicolegal consultant and expert witness in cases of prone restraint cardiac death. No other relevant potential financial conflicts of interest.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.