
Abstract
There is an on-going debate about the safety of prone restraint and the exact role of the prone position in physical restraint death. Cardiac arrest in prone restraint death is essentially the end-result of a violent physical altercation wherein a combative individual suddenly loses consciousness while trying to counteract an opposing force. The direct correlations of increased static weight force with decreased inferior vena cava diameter, decreased cardiac output, and decreased stroke volume in prone restraint studies suggest that decreased venous return and decreased cardiac output could have a significant role to play in prone restraint death. Although the degree of changes observed in those studies might not be sufficient to cause cardiac arrest, they could predispose people who instinctively try to free themselves of the restraints to severe complications. The Valsalva maneuver, or forceful expiration against a closed airway, is frequently performed spontaneously in daily activities involving straining and resistance exercise, but has never been considered in restraint death. Pre-existing diminished venous return could increase the risk of major complications in individuals performing the Valsalva maneuver. A substantial decrease in venous return and cardiac output could increase the risk of cerebral hypoperfusion, loss of consciousness, hypoventilation, and sudden death. By increasing the risk of increased intra-abdominal pressure and its negative effect on venous return, high body mass index may be a significant risk factor in prone restraint death. The Valsalva maneuver may have different roles in prone restraint cardiac arrest and might be overlooked in prone restraint death.
Keywords
Introduction
There is an on-going debate about the safety of prone restraint. Recently, two review articles on restraint physiology expressed very different viewpoints on the pathophysiology of prone restraint death.1,2
Although case series suggest that prone position, thoracic pressure, and high body mass index (BMI) may be relevant to restraint death,3–7 further study is needed to support that assumption, according to the first review article. 1 The second review article explains that prone restraint, by decreasing ventilation and cardiac output, increases the severity of the metabolic acidosis associated to the physical struggle of the restraint process. 2 According to the prone restraint cardiac arrest postulate (PRCA postulate), ventilation restriction during prolonged prone restraint would eventually result in increased carbon dioxide partial pressure, uncompensated metabolic acidosis, and cardiac arrest. 8 Indeed, the case series reported by Hick et al. 9 suggests that severe metabolic acidosis may be a major factor precipitating cardiac arrest in handcuffed individuals with acute psychosis who are continually struggling against restraints. However, George Floyd was not struggling against restraints and the struggle was not significant in the two cases described by Weedn et al. 8
On the basis of the clinical information and methods in multiple restraint studies, prone restraint death is likely not to be a single clinical entity. Prone restraint cardiac arrest has been found to occur very rapidly during the control phase, before the use of handcuffs, when pressure is applied on the upper back of the individual.4,5,7,10–12 Many restraint studies are reactive, with a focus on either dynamic weight forces, 13 when the pressure is applied with one or two knees on the upper back, or on static weight forces,14–16 when the restraint technique involves lying over a large surface of the individual's upper back.
Strong relationships are likely to exist among the individual's resistance, the restraint technique, and the struggle during the events leading to cardiac arrest in prone restraint death. 7 However, no robust cardiovascular physiological explanation exists for how cardiac arrest can occur within 60 s during the control phase 7,10,12 or within more than 20 min after the individual is handcuffed and restrained. 7
The Valsalva maneuver, or forceful expiration against a closed airway, is frequently performed spontaneously in daily activities involving straining and resistance exercise.17,18 The mechanical effect and the neurohormonal response associated to the Valsalva maneuver have been associated to different complications ranging from syncope19,20 to cardiac arrhythmias, some of which have eventuated in death.21–23 The purpose of this article is to explore the possible role of the Valsalva maneuver in prone restraint death.
Restraint studies
The study by Roeggla et al.
As the degree of change in heart rate (−21.3%), mean arterial blood pressure (−28.9%), and cardiac output (−37.4%) is much greater with respect to those in other studies in which a static weight force is used in resting subjects,14–16 the first review article 1 questions the validity of the study by Roeggla et al. 24
The study by Roeggla et al. 24 suggests indeed that a sudden increase in intrathoracic pressure in the prone hobble position can predispose individuals to significant complications. To explain the decrease in mean arterial blood pressure/cardiac output and the decrease in heart rate, Roeggla et al. mention an increase in intrathoracic pressure and the Bezold-Jarisch reflex, respectively. 24 Although the discussion does not indicate whether spirometry may have played a role in their findings, all cardiorespiratory parameters, including forced vital capacity measurement by spirometry, were assessed after 3 min of prone hobble. 24 Spirometry test implies a significant increase in intrathoracic pressure. The most frequent safety incident involving spirometry is syncope. 25
The studies by Cary et al. and Sloane et al.
The restraint asphyxia theory 26 left an indelible footprint on restraint studies. Although the discussion in the studies by Cary et al. 27 and Sloane et al. 28 is focused on respiratory impairment, their results suggest indeed that one of the main issues in prone restraint death may be related to decreased venous return and decreased cardiac output.
PETCO2, cardiac output, and transition from exercise to rest (recovery period)
In the studies by Cary et al. and Sloane et al. monitoring post-exercise end-tidal carbon dioxide partial pressure (PETCO2) in three positions (Table 1),27,28 the interdependence between the respiratory and cardiovascular systems 29 might have been minimized. In both studies, the negative effects of the sitting position on venous return were not considered. In the sitting position, flexion of the lower extremities and gravity negatively affect venous return, 30 whereas these effects are absent in the prone position.
Cardiorespiratory variables post-exercise in three different positions.

PETCO2: end-tidal carbon dioxide partial pressure; VM (l min−1): minute ventilation.
a Significant statistical difference with seated position.
b Significant statistical difference with the prone position.
c Cary et al. J Physiol 2000;525(Suppl):30–31. 27
d Sloane et al. Forensic Sci Int 2014;237:86–89. 28
PETCO2 depends on two physiological determinants: pulmonary blood flow (cardiac output) and CO2 production (VCO2). 31 PETCO2 can be a useful marker of cardiac output under constant ventilation, 31 in cardiopulmonary resuscitation (CPR) 32 and under spontaneous ventilation. 33 Two factors explain how a decrease in cardiac output lowers PETCO2. Decreases in pulmonary perfusion decrease CO2 delivery to the lungs.31,32 Decreases in pulmonary perfusion increase the alveolar dead space when the superior part of the lungs becomes under perfused. The CO2 content exiting from the alveoli located in the superior part of the lungs is thus lower.31,32
During the recovery period, VCO2 is not the only ventilation stimulus. 34 Although VCO2 returns to its basal resting value within 15 min (Figure 1), PETCO2 remains lower than its basal resting value (Figure 2) until metabolic acidosis from exercise is corrected. 34 In a study by O’Neill et al., bicarbonate, lactate, and pH have been found to return to baseline levels 45 min post-exercise. 34 In each study,27,28 at the same time interval, VCO2 should essentially have the same value regardless of the position.

Oxygen uptake (VO2), carbon dioxide output (VCO2), and gas exchange ratio (R) during progressive incremental bicycle exercise to peak exercise (P) and for 15 min of recovery.

End-tidal PCO2 and arterial PCO2 during progressive incremental bicycle exercise to peak exercise (P) and for 15 min of recovery.
The study by Cary et al
When the prone and sitting positions are compared (Table 1), the statistically lower PETCO2 in the sitting position (−2.6 mmHg) cannot be attributed to ventilation: minute ventilation is lower in the sitting position. The statistically higher post-exercise heart rate (+10 bpm) strengthens the assumption that the lower PETCO2 in the sitting position is likely to be a marker of a lower cardiac output.
When the sitting position and the prone restraint position are compared, the significant increase in minute ventilation (+25%) may explain the lower PETCO2. However, the decrease in PETCO2 in the prone restraint position appears disproportionally low (
In the immediate recovery period, when VCO2 is higher than its basal resting value (Figure 1), PETCO2 could paradoxically have a higher value if a significant decrease in cardiac output occurs suddenly. By causing a marked decrease in venous blood flow transit time in the peripheral tissues, the effect of a sudden decrease in cardiac output should be an increase in CO2 venous partial pressure. 32 After a 10-min interval, when VCO2 returns to its basal resting value (Figure 1), the paradoxical effect on PETCO2 should disappear, as indicated in Table 1 in the prone maximal restraint position (PMRP) in a study by Sloane et al. 28
The study by Sloane et al
Several findings reported by Sloane et al. 28 suggest that one of the main issues with the PMRP in individuals with high BMI might be decreased venous return and decreased cardiac output. At time 0, the decrease in heart rate in the prone position suggests a higher venous return, thus potentially explaining some of the discrepancies with respect to the other two positions. The statistically significant increase in heart rate and decreased PETCO2 at the 15-min interval suggest a decreased venous return and a decreased cardiac output in the sitting position and the PMRP (Table 1).
The most notable findings in that study 28 may be associated with PETCO2 trends (Table 1). Normally, the lowest PETCO2 value is in a 5-min interval; PETCO2 should increase and stabilize in a 10-min interval; after a 15-min interval, PETCO2 should slowly increase with the correction of metabolic acidosis 34 (Figure 2). The progressive decrease in PETCO2 between the 10-min and 15-min intervals in the PMRP, a time period in which VCO2 should normally have returned to its basal resting value (Figure 1), does not suggest “just the opposite of diminution of ventilation” 28 ; but that the cardiac output is significantly decreased in the PMRP. More specific markers of tissue hypoperfusion, such as lactate and base excess, were not assessed in that study.
The Valsalva maneuver
Cardiac arrest in prone restraint death is essentially the end-result of a violent physical altercation wherein a combative individual suddenly loses consciousness while instinctively trying to counteract an opposing force. Prior experimental studies have not truly been able to mimic real-life events, which may involve significantly greater stress.
The Valsalva maneuver has never been considered in restraint studies. The Valsalva maneuver is frequently performed spontaneously in several sporting activities involving resistance exercises, such as weight lifting 35 and rowing. 36 By increasing intra-abdominal and intrathoracic pressure, the Valsalva maneuver increases trunk stability 37 and isometric contraction force. 38 The Valsalva maneuver has substantial effects on venous return, stroke volume, heart rate, cardiac output, blood pressure and catecholamines (Table 2).18,39 The Valsalva maneuver increases the blood pressure response associated with resistance exercises. 40
Mechanical effects-Neurohormonal response during the Valsalva maneuver. a
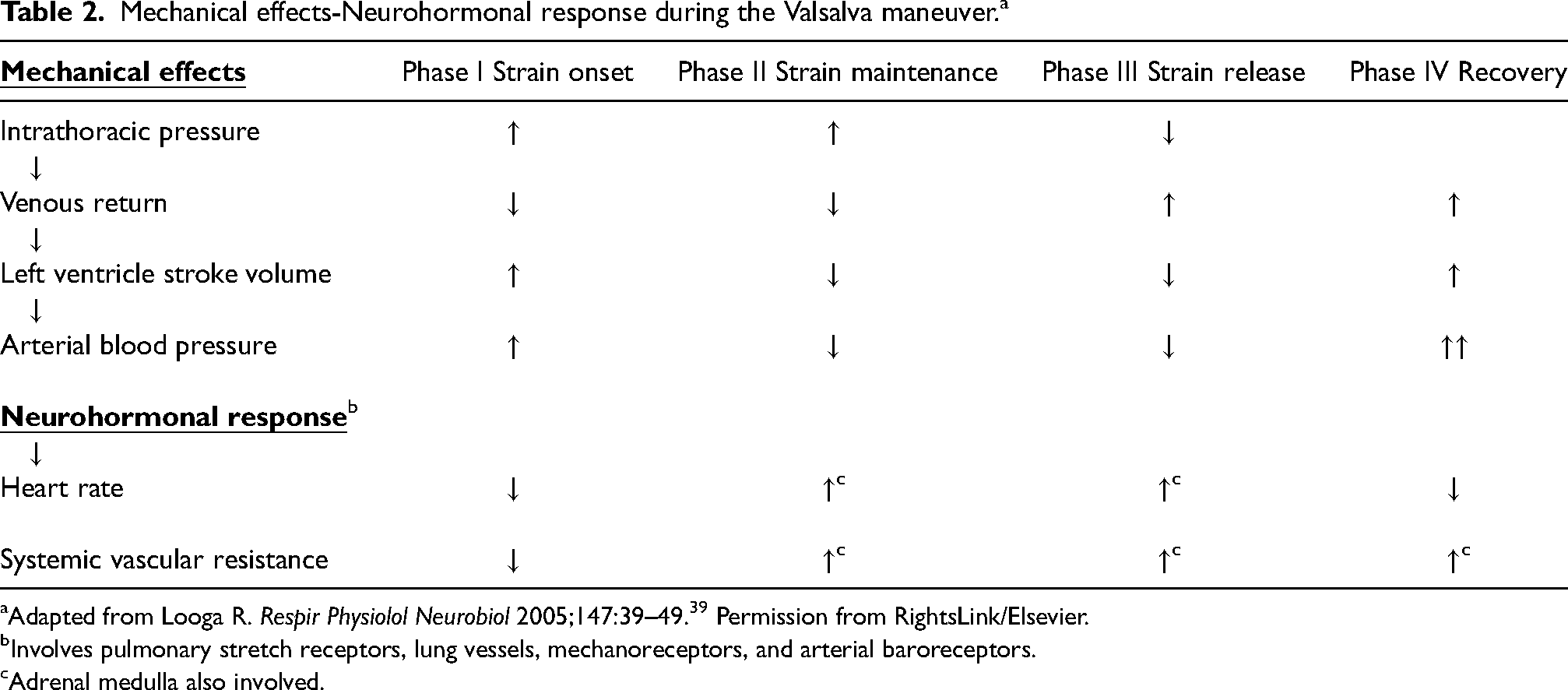
Adapted from Looga R. Respir Physiolol Neurobiol 2005;147:39–49. 39 Permission from RightsLink/Elsevier.
Involves pulmonary stretch receptors, lung vessels, mechanoreceptors, and arterial baroreceptors.
Adrenal medulla also involved.
Decreased plasma volume and repetitive Valsalva maneuvers can affect the cardiovascular response to the Valsalva maneuver. Repetitive Valsalva maneuvers have been shown to cause significant decreases in arterial blood pressure in early and late phase II and phase III. 41 By causing incremental accumulation of blood in the lower extremities, each maneuver could result in a progressive decrease in the blood volume available for venous return. 41 Decreased plasma volume can also decrease the systolic blood pressure, particularly during phase II and phase III. 42 Repetitive Valsalva maneuvers could also decrease catecholamine reserves. 41
Factors predisposing individuals to syncope during the restraint process
Loss of consciousness from situational syncope has not previously been considered in prone restraint death. Situational syncope is a reflex-mediated syncope occurring in clinical conditions associated to increased intrathoracic pressure.43,44
In situational syncope, the respiration may be shallow and slow 45 and can even stop. 46 On the basis of the study by Cummin et al., 47 situational syncope should be considered a life-threatening complication during the restraint process. Hypothesizing that respiration could stop for brief periods through compression of the trunk or breath holding during the restraint process, Cummin et al. 47 have assessed the effect of breath holding during and after a short period of exercise. The authors have depicted very rapid blood O2 desaturation, particularly at low lung volumes. They also observed “hypoxia-associated dysrhythmias” in two participants and stressed the possibility of cardiac arrest if “cessation of breathing for short periods” occurs “during vigorous restraint, particularly if the thorax and abdomen are compressed.” 47
In resistance exercise, the main factor at the origin of post-exercise hypotension and syncope is decreased cardiac output caused by decreased stroke volume. 48 High BMI, prone restraint techniques, and the individual's reaction when he is instinctively trying to counteract an opposing force can increase the risk of syncope during the restraint process.
High BMI
High BMI influences intra-abdominal pressure. 49 By increasing the risk of significant decreased venous return in the prone position, high BMI could be an independent risk factor in prone restraint death.
Prone position and high BMI, which have repeatedly been associated with restraint death,5–8,10,11 are two independent predisposing factors for the abdominal compartment syndrome. 50 Abdominal compartment syndrome refers to organ dysfunction caused by intra-abdominal hypertension. 51 In the abdominal compartment syndrome, decreased abdominal compliance by mechanical restriction of the abdominal wall can result in intra-abdominal hypertension. Increasing intra-abdominal hypertension consequently increases intrathoracic pressure by causing cephalad movement of the diaphragm.51,52 Intra-abdominal hypertension can impair cardiac output by decreasing venous return and altering cardiac function.51,52 Decreased venous return is caused by a functional obstruction of the inferior vena cava. The cephalad movement of the diaphragm can result in cardiac compression, decreased ventricular compliance, and contractility.51,52 Decreased intravascular volume predisposes individuals to a decrease in cardiac output at lower levels of increased intra-abdominal pressure. 52 Systemic vascular resistance, through compression of systemic vasculature and the aorta, is increased in the abdominal compartment syndrome. 52 In individuals with impairment of cardiac contractility or decreased intravascular volume, such increases in systemic vascular resistance may be poorly tolerated. 52 In the abdominal compartment syndrome, any intervention that increases intrathoracic pressure can increase the negative effects of intra-abdominal hypertension on cardiac output. 52
Prone restraint techniques
Smaller blood volume predisposes to syncope.43,53,54 Prone restraint studies depict direct correlations among increased static weight forces on the upper back of resting individuals and decreased inferior vena cava diameter, stroke volume, and cardiac output.14–16
The individual's reaction to the restraint technique
At least four situational syncopal syndromes associated to an increase in intrathoracic pressure43,44,55 can be associated to an individual's instinctive reaction during the restraint process.
Weight lifter's syncope
In weight lifting competitions, a strenuous Valsalva maneuver can increase intrathoracic pressure up to 260 mm Hg; abruptly decrease venous return, cardiac output, and cerebral blood flow; and result in loss of consciousness. 35
Mess trick and fainting lark syncope
Mess trick syncope 46 and the fainting lark syncope46,56 are two variants involving hyperventilation and a sudden increase in intrathoracic pressure. In mess trick syncope, the participant hyperventilates for approximatively 1 min. Thereafter, the chest is suddenly compressed by an individual standing behind the participant. Instinctively, the participant counters the pressure on the ribs by closing the glottis and contracting the abdominal muscles. 46 In fainting lark syncope, orthostatic stress is added, and the Valsalva maneuver is voluntary.46,56 In a study in which the authors were also participants, Howard et al. have described a fainting lark syncope involving a “moderate” Valsalva maneuver of 5 s resulting in generalized clonic convulsions and apnea lasting approximatively 30 s. 46 In contrast to weight lifter's syncope, the Valsalva maneuver in fainting lark may be unnoticeable, even by highly knowledgeable individuals. 57
Wind instrument player's syncope
A single deep inspiration followed by breath holding can also lead to syncope. In one study in an otherwise healthy individual who had two episodes of life-threatening syncope while apnea diving, 58 the only finding was a pathological decrease in systolic blood pressure during early phase II of the Valsalva maneuver. In that case, in which hyperventilation was excluded as a precipitating factor, mechanical factors, possibly compression of the inferior vena cava resulting in severe venous return impairment, were considered the most likely cause of syncope. 58
Laughter induced syncope
In this subtype of situational syncope, the Bezold-Jarisch reflex may have a role. 44 By causing episodes of prolonged forced expiration against a closed glottis, vigorous laughter results in an increase in intrathoracic pressure. The decreased venous return to the heart that follows activates baroreceptors: the sympathetic activity is reduced and the parasympathetic cardiovascular tone is increased. Syncope is the end-result of sudden cerebrovascular hypoperfusion caused by hypotension and bradycardia. 44
Precipitating factor of loss of consciousness in prone restraint
In two case reports of prone restraint cardiac arrest , loss of consciousness may have been precipitated by a sudden increase in intra-abdominal and intrathoracic pressure. In the first case report, 59 loss of consciousness occurred when the individual (BMI: 23.3 kg/m2) began vomiting. Retching and vomiting may be associated to a substantial increase in intra-abdominal and intrathoracic pressure. 60 In the second case report, 61 loss of consciousness occurred when the individual (BMI: 35.6 kg/m2) used his hands and his arms to push his chest off the ground. According to the coroner's public inquiry, a dynamic weight force was being applied to the individual's right upper back/shoulder with one knee at that moment. By trying “to push himself up,” the individual probably underwent one or more than one strenuous Valsalva maneuvers, as in weight-lifting.
Sudden cardiovascular collapse during chest compression in the prone position
Static weight force restraint technique
In the case report (BMI: 42 kg/m2) by Nissen et al., two persons (about 80 kg each) were lying on the individual's torso while the individual was prone restrained. 10 The individual's arms and legs were being held restrained against the floor. Cyanosis, respiratory arrest, and spontaneous micturition occurred within about 2 min from the start of the “take down.” The restraint process was stopped almost immediately. After 1–2 min of CPR (external chest compression and mouth to mouth respiration) in the supine position, the individual regained respiration and consciousness. Interviewed later, the individual could recall that he could not breath while being prone restrained.
Considering the high BMI and the fact that the abdominal cavity was trapped against a rigid surface, 10 the static weight force used to restrain that individual likely caused substantial venous return impairment through inferior vena cava compression and increased intrathoracic pressure.14–16,52 The loss of consciousness may have been precipitated by a sudden increase in intrathoracic pressure when the individual felt that he could not breath. The instinct to fight restraint is typical in restraint death. 62 If a weight force is suddenly compressing an individual's chest to the point that he “cannot breathe,” and that the individual is unable to use his arms and his hands to free himself from restraints, the most likely instinctive reaction to counter that weight force in the opposite direction is by closing the glottis, contracting the abdominal muscles, and use the chest to push away the weight force.
In the two case reports of prone restraint death described by Weedn et al., 8 the loss of consciousness may also have been precipitated by a Valsalva maneuver. By raising forcefully his head and shoulders once prone restrained, the individual in case #1 (BMI; 39.7 kg/m2) was possibly performing repetitive Valsalva maneuvers. In case #2 (BMI: 32.7 kg/m2), loss of consciousness occurred apparently 9 s after a 190 pounds law enforcement officer (LEO) sat suddenly on the top of a rigid spine board. The clinical information immediately preceding the loss of consciousness in that second case is similar to the case report by Nissen et al. 10 In the two case reports by Weedn et al. 8 however, there were substantial delays before CPR initiation.
Dynamic weight force restraint technique
A dynamic weight force restraint technique has the potential to create a hyperacute or acute abdominal compartment syndrome. In the only dynamic weight force restraint study performed on a CPR training mannequin, the dynamic weight force applied by a single knee is as high as 650 N. 13 In CPR, approximately 500 N applied on the chest in the prone position is sufficient for adequate blood perfusion.63–66 Moreover, in CPR, complete chest decompression between compressions is essential to allow adequate venous return back to the right ventricle for the next compression to be efficient. 67
Immobilized in the prone position, Robert Dziekanski (BMI: 27.5 kg/m2) was fiercely resisting the restraint process by holding his arms tightly under his body. After a period of approximatively 50 s in which pressure was being applied “across his shoulder blades” by the right knee of one of two LEOs, loss of consciousness occurred very rapidly once Robert Dziekanski's chest came in direct contact with the floor. 12 At that moment, the pressure resulting from the dynamic weight force applied by the LEO's right knee might have been inadvertently increased. That LEO, located on the individual's left side, was then helping his colleague located on Robert Dziekanski's right side to handcuff Robert Dziekanski's right wrist. 12
At least three different mechanisms associated to a sudden increase in intrathoracic pressure could have caused a sudden loss of consciousness followed by a lethal arrhythmia in Robert Dziekanski's case. A severe and sustained increase in intrathoracic pressure caused by the dynamic weight force restraint technique could have resulted in a critical decrease in venous return, followed by severe bradycardia and loss of consciousness.68,69 The dynamic weight force restraint technique could have led to direct compression of a vital structure.70,71 Robert Dziekanski could also have performed a Valsalva maneuver immediately after his chest was suddenly compressed against the floor. The Valsalva maneuver could have been performed either instinctively, as in the pathophysiology in the mess trick syncope, or voluntarily, to counter the dynamic weight force in the opposite direction. The standing position is not a prerequisite for syncope.72,73 Pre-existing venous return impairment caused by chest and abdominal compression might have had the same effects of gravity on venous return as those in a fainting lark syncope.46,56
In the case report by Kunz et al. (BMI: 27.2 kg/m2), 74 the individual's pre-existing clinical condition (psychostimulants; severe physical exhaustion) before the restraint process was at odds with Robert Dziekanski's. On the basis of the study by Kroll et al., 13 the sudden increase in intrathoracic pressure caused by the double-knee restraint technique, rather than situational syncope, appears as the most likely factor precipitating the malignant arrhythmia clinically.
Potential effects of syncope and chest compression during the restraint process
The potential effects of syncope during the restraint process can be substantial (Figure 3). The Bezold-Jarisch reflex 75 may also have a role after loss of consciousness. In response to a severe decrease in central blood volume, substantial bradycardia, a decrease in systemic vascular resistance and negative inotropy have been reported. 75
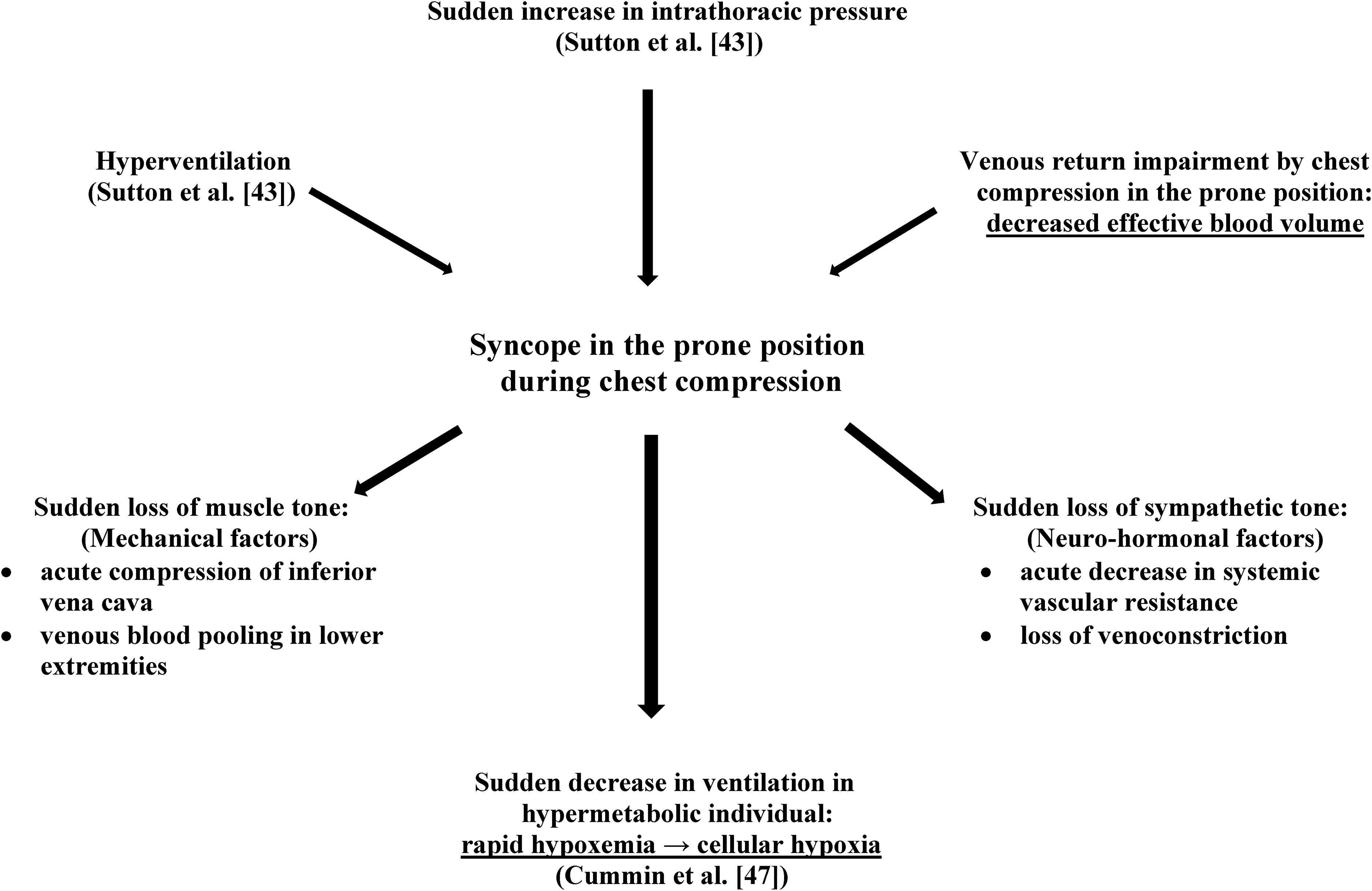
Potential effects of syncope occurring during chest compression in the prone position during the restraint process.
Prone maximal restraint position
In one prospective study, the authors explained that, in their cohort, in contrast to other cohorts, the “hogtie” or the “position of maximal restraint” was never used. 76 The authors did not describe why a restraint technique so commonly used in the past was abruptly discarded. 76
By trapping the abdominal cavity against a rigid surface, certain restraint techniques in the prone position, through causing intra-abdominal hypertension, can predispose individuals to venous return impairment during both inspiration (Table 1) and expiration (Table 2). Inspiration, by increasing intra-abdominal pressure, should increase inferior vena cava functional obstruction and decrease venous return.51,52 During expiration, straining and repetitive Valsalva maneuvers, through increasing intra-abdominal and intrathoracic pressure, should also negatively affect venous return (Table 2). According to studies on rowing, in which unimpeded venous return during the recovery phase of the stroke is essential to maintain adequate cardiac output, 77 decreased venous return during inspiration should increase the risk of progressively decreased venous return and cardiac output during the restraint process.
By apparently impeding the struggle and physical exertion, the PMRP might give a false sense of security. In a psychotic individual tightly restrained in the prone position against a hard surface, the only remaining option to oppose the restraint process, particularly in a situation of breathlessness, might be repetitive isometric contractions and repetitive Valsalva maneuvers. Over a certain period, decreased venous return during inspiration (Table 1) and the adverse physiological effects of the Valsalva maneuver18,39 (Table 2) should lead to progressive metabolic acidosis 78 and, eventually, myocardial dysfunction. In those circumstances, pulseless electrical activity could be the result of either a sudden bradycardia coupled to a sudden increase in systemic vascular resistance caused by a Valsalva maneuver, progressive hypoventilation caused by ventilation restriction as suggested in the PRCA postulate, or progressive hypoventilation caused by progressive cerebral hypoperfusion.
Summary
By causing severe mechanical limitation of the abdominal wall, certain prone restraint techniques predispose individuals to decreased venous return and decreased cardiac output. In individuals with a high BMI, there is a greater risk of substantial increase in intra-abdominal hypertension and its negative effects on venous return and cardiac output.
Although a few case reports suggest that cardiac arrest in prone restraint may have been precipitated by a sudden increase in intrathoracic and intra-abdominal pressure, the Valsalva maneuver has never been considered in prone restraint death. Pre-existing diminished venous return and cardiac output can increase the risk of major complications in individuals performing the Valsalva maneuver.
The Valsalva maneuver may have different roles in prone restraint death. A sudden and substantial increase in intrathoracic and intra-abdominal pressure can result in sudden cerebral hypoperfusion, syncope, hypoventilation, and cardiac arrest. After syncope, continuous chest compression in the prone position increases the risk of hypoventilation, asphyxia, and cardiac arrest. In individuals struggling almost continuously against restraints, the adverse physiological effects of repetitive Valsalva maneuvers can contribute to progressive metabolic acidosis and progressive myocardial dysfunction. In a clinical situation of severe physical exhaustion and severe metabolic acidosis, the triad consisting of decreased venous return, decreased cardiac output, and the Valsalva maneuver can precipitate a malignant arrhythmia. The Valsalva maneuver may be overlooked in restraint death.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.