
Abstract
There is a debate over whether the effect of prone restraint on respiration can lead to cardiac arrest. In itself, the prone or prone restrained posture does not likely compromise ventilation to any clinically significant degree for a detainee who is passive and calm, as a number of prone restraint studies have shown. However, these studies were not able to replicate an anxious, distressed or intoxicated (alcohol or drugs) detainee who is struggling and being actively held down. This review examines the physiology and biomechanics of respiration, highlighting the differences between upright position respiration and prone respiration and the effect of restraint on respiration. In addition, the findings of research on the effects of struggling, obesity, anxiety or panic and drug intoxication on the consequent carbon dioxide (CO2) production and the work of breathing are presented. The limitations which each of these factors place on the ability to remove CO2 from the blood are discussed. The evidence suggests that severe respiratory or metabolic acidosis could arise as the result of the combined effects of several factors and that cardiac arrest, if it occurs, would be more likely due to hypercapnia than hypoxia.
Introduction
In recent years, there have been a number of reports in the news of deaths of agitated individuals restrained in the prone position, e.g., Edward Bronstein, 1 Mario Gonzalez Arenales 2 and George Floyd. 3 One hypothesis is that asphyxia, referred to as “positional asphyxia” or “restraint asphyxia,” is a primary factor in the cause of death, although the results of some scientific studies appear to dispute the validity of this hypothesis. 4 Arguments for the hypothesis that cardiac arrest during prone restraint can be attributed to uncompensated metabolic acidosis have been made in comprehensive reviews by Steinberg.5,6 The authors suggest that “prone restraint cardiac arrest” is a more accurate designation of the phenomenon than “positional asphyxia” or “restraint asphyxia” since death is theorized as being due to uncompensated acidosis from decreased ventilation and cardiac output observed in subjects under prone restraint. Our objective is to review the physiology relevant to respiration in the prone restrained posture and relevant empirical data, with a focus on the factors contributing to CO2 and lactate production during prone restraint. This includes an assessment of the work being done by the musculature under conditions of prone restraint and the ability of the cardiopulmonary system to eliminate CO2 and lactate from the cardiovascular system in order to avoid uncompensated respiratory or metabolic acidosis.
Upright respiration mechanics
The outer surface of the lung and the inner surface of the chest wall are lined with smooth pleural membranes. The pressure in the space between the pleural membranes is usually 4 mm Hg at rest, i.e., the pressure in the intrapleural space is lower than inside the alveoli of the lungs, keeping the alveoli from collapsing. At rest, the pressure difference between the intrapleural space and the atmosphere is equal and opposite to the pressure in the intrapleural space, such that the inward elastic recoil of the lung (elastic force acting to collapse the alveoli) exactly opposes the outward-acting elastic recoil of the chest wall (elastic force acting to expand the chest wall), such that there is no net airflow. For air to enter the lungs (inspiration), the pressure of the thoracic cavity must decrease to reduce alveolar pressure below atmospheric pressure (Figure 1).
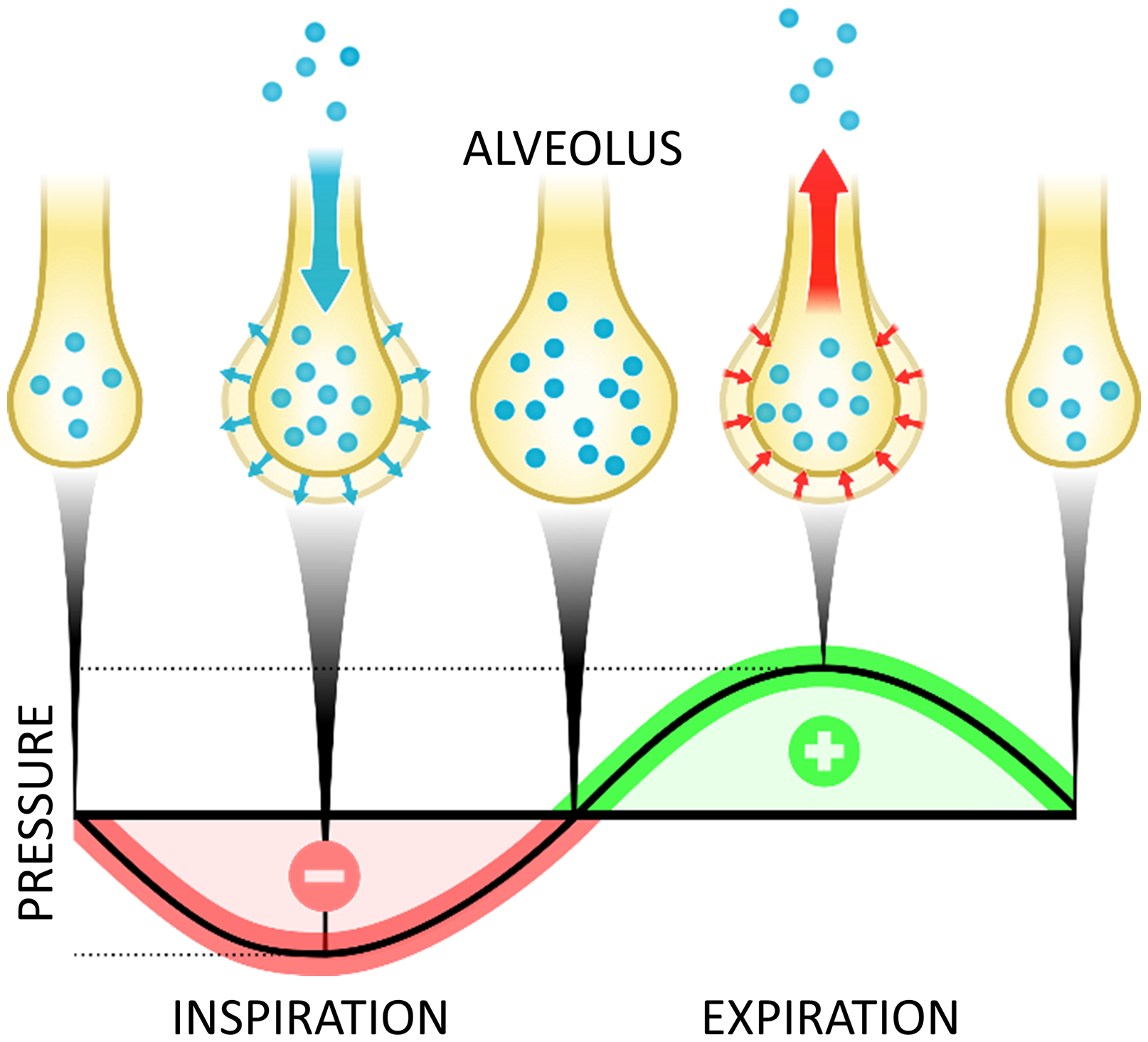
Changes in intrapleural pressure during respiration.
Inspiration in the upright posture is achieved by contraction of the diaphragm, contraction of the scalene and sternocleidomastoid muscles attached to the sternum and contraction of the external intercostal muscles attached to the ribs. Contraction of the diaphragm causes it to move downward in the abdomen. Contraction of the scalene and sternocleidomastoid muscles lift the upper ribs in a combined cranial and anterior direction, similar to lifting a pump handle, which moves upward and away from the pump. The diaphragm and external intercostal muscles act to expand the lower ribs, both in the anterior and lateral directions as they lift, similar to lifting a bucket handle, causing the thoracic cross-sectional area to increase as it moves upward (Figure 2). The resulting increase in volume of the thoracic cavity reduces airway pressure pushing atmospheric air into the lungs. The alveoli inflate because the intrapleural pressure decreases due to the increase in volume of the thoracic cavity. Contraction of the diaphragm is responsible for approximately 70% of lung displacement during breathing at rest. 7 However, as exercise intensity increases, the ribcage contributes a larger proportion to the change in volume. 8 Expiration in the upright posture is achieved by relaxation of the diaphragm and rib cage muscles, which causes the diaphragm and rib cage to move back to their rest positions, reducing the volume of the thoracic cavity, and thereby increasing airway pressure, pushing air from the lungs back to the atmosphere. During exercise, abdominal muscles contribute to the reduction in thoracic volume by displacing the abdomen. 8
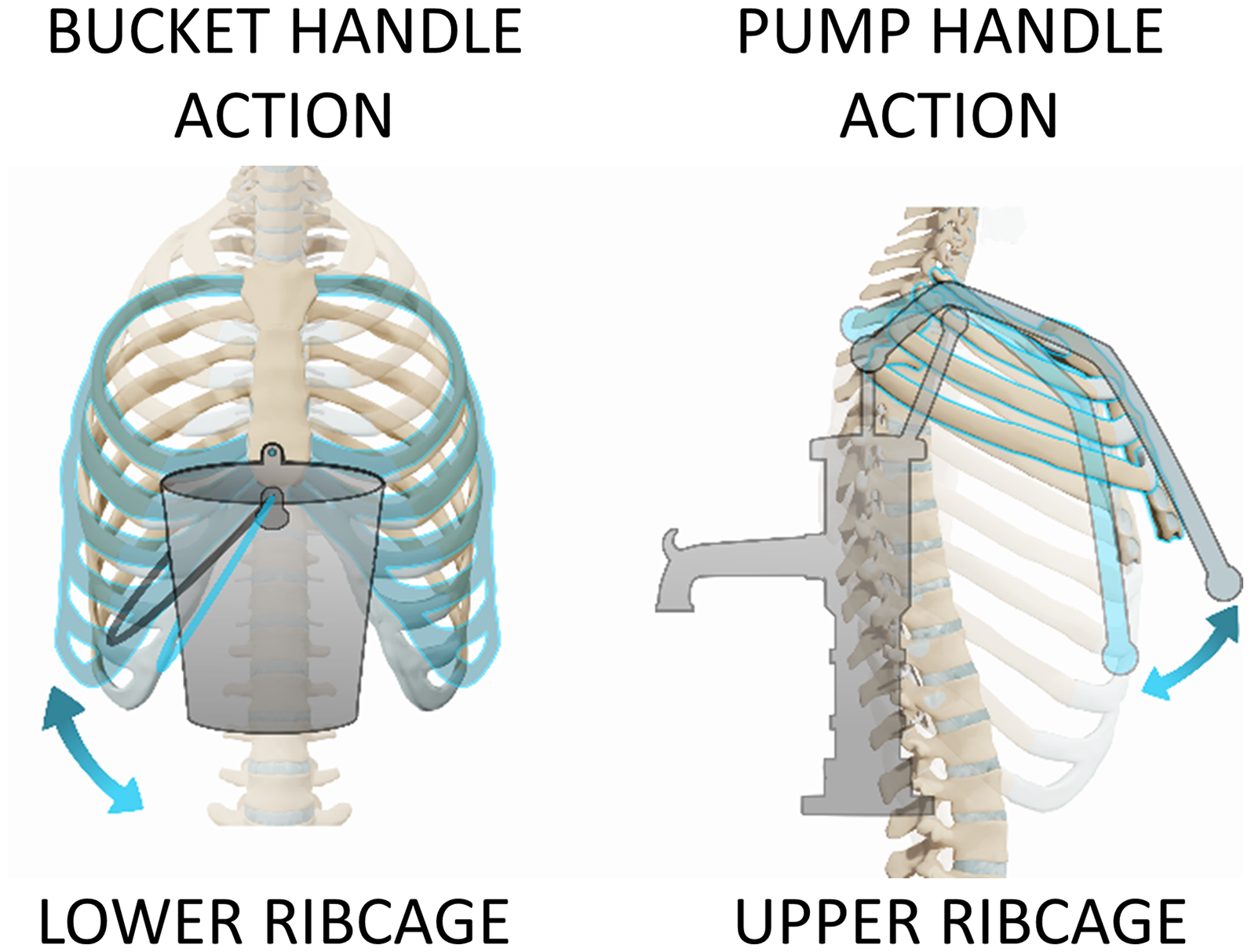
(A) Bucket handle action in moving lower ribcage. (B) Pump handle action in moving upper ribcage.
Work of breathing
The work of breathing is the work that the respiratory muscles perform in moving air in and out of the lungs. There are two components to the work of breathing: Elastic work which moves or deforms the mechanical structures (skeleton and soft tissue) and resistive work which overcomes the resistance to air flow in the airways. Resistive work increases as the rate of air flow increases. A simple way to conceptualize how the work of breathing changes is to represent it as being modulated in the manner similar to the product of the pressure and volume during respiration, e.g., at higher pressures more work must be done to produce the same change in volume. The pressure is affected by factors such as the compliance of the lungs and airways. The lower the compliance, the greater the change in pressure necessary to produce a given change in volume because there is more resistance to increasing the volume of the lungs and more work must be done by the respiratory muscles to achieve the same airflow. To produce greater airflow more work must be done since this requires a greater change in the volume of air.
Increasing ventilation, either by increasing ventilatory rate (breathing frequency) or ventilatory volume (tidal volume) will increase the work of breathing. Clearly, the work of breathing will increase with exercise intensity since airflow must increase. It is perhaps less obvious that the work of breathing will be minimized at moderate lung volumes. However, this is where lung compliance is highest, therefore, requiring less work to produce a change in lung volume than at high or low lung volumes. 9 High abdominal pressure can also increase the work of breathing since the diaphragm must work against the resistance of abdominal pressure during inspiration. 10
The byproducts of muscular work depend on whether muscle fibers use aerobic metabolism (oxidative fibers) or anaerobic metabolism (glycolytic fibers) to produce the ATP necessary for muscle contraction. Most skeletal muscles are composed of both types of fibers. Aerobic metabolism produces CO2 as a byproduct whereas anaerobic metabolism produces lactic acid (lactate) and hydrogen ions, which can increase blood acidity. The predominant byproduct of muscular work will be CO2 since glycolytic fibers are used less frequently than oxidative fibers, i.e., glycolytic fibers are principally activated only for short forceful contractions. However, the diaphragm does contain a relatively high percentage of glycolytic fibers 11 so lactate can be produced by respiratory muscles during respiration, particularly under conditions where the work of breathing increases due to an increase in ventilatory rate or when forceful contraction of the diaphragm is required to overcome loading or low lung compliance.
Gas exchange
In the context of the present review, the term respiration will be used to encompass the process of gas exchange within the cardiopulmonary system. The inspired air entering the alveoli in the lungs during respiration has O2 partial pressure of approximately 149 mm Hg compared to an O2 partial pressure of approximately 40 mm Hg in the mixed venous blood entering the alveolar capillaries. This partial pressure difference results in passive diffusion of O2 from the alveoli to the blood of the alveolar capillaries. The CO2 partial pressure in the mixed venous blood is approximately 45 mm Hg whereas the CO2 partial pressure of freshly inspired air in the alveoli is approximately 0 mm Hg. Therefore, the partial pressure difference results in CO2 being eliminated from the mixed venous blood of the alveolar capillaries by passive diffusion into the alveoli. An important factor in efficient gas exchange is the large blood volume within the alveolar capillaries which slows blood flow, allowing more time for gas exchange. In addition, different relations between partial pressure and molecular content (concentration) for O2 versus CO2 result in an increase in O2 partial pressure in end capillary blood of approximately 60 mm Hg compared to a decrease of only about 5 mm Hg in CO2 partial pressure during gas exchange. 12 As a result, the concentration gradient for moving O2 from the alveoli into the blood is much greater than the concentration gradient for moving CO2 from the blood into the alveoli, suggesting that the risk of hypercapnia is greater than the risk of hypoxia if CO2 begins to accumulate in the blood.
Respiratory acidosis
In general, an increase in the force produced by contracting muscles results in increased metabolism and, hence, increased CO2 and production of hydrogen ions associated with glycolysis. The CO2 readily diffuses into the blood where the vast majority combines with water to form carbonic acid in a reaction catalyzed by carbonic anhydrase (Figure 3). Carbonic acid rapidly dissociates to form bicarbonate and hydrogen ions. Much of the remaining CO2 binds to hemoglobin with a small percentage retained as dissolved gas. The concentration of hydrogen ions in the blood determines its acidity (pH). In the alveolar capillaries, bicarbonate is converted back to CO2 and together with CO2 that dissociates from hemoglobin, can diffuse into the alveoli and be removed from the body through expiration of air from the lungs. Under normal conditions, minute ventilation (volume of air flow in and out of the lungs per minute) is regulated to maintain blood homeostasis, keeping O2 partial pressure, CO2 partial pressure and blood pH within a narrow range. Hyperventilation increases CO2 removal and, thus, pushes the bicarbonate buffer system towards forming CO2 and water while decreasing the concentration of hydrogen ions, thereby increasing blood pH. If CO2 removal from the body cannot keep up with CO2 production then the CO2 partial pressure of arterial blood will increase, resulting in less CO2 being buffered by bicarbonate production, increasing blood acidity, i.e., lowering blood pH. This condition is known as respiratory acidosis. Respiratory acidosis is observed within the first minute of moderate and intense exercise but normalizes after relatively small reductions in blood pH due to effective bicarbonate buffering. During more intensive exercise, muscle metabolism results in sufficient excess production of CO2 and hydrogen ions produced during glycolysis to cause metabolic acidosis. 13 Although blood acidity increases during exercise, arterial CO2 partial pressure decreases. 14 End tidal CO2 partial pressure initially increases as exercise intensity increases and then decreases at high levels of exercise intensity. 15 Since minute ventilation increases in proportion to exercise intensity, the reductions in end tidal CO2 partial pressure indicates that ventilation cannot keep up with the production of CO2, i.e., the molecular content of CO2 in a given volume of expired air is reduced when exercise intensity is high. The increase in blood acidity, despite reduced arterial CO2 partial pressure, indicates that CO2 is being buffered and that the acidosis is metabolic rather than respiratory. Nevertheless, either respiratory or metabolic acidosis can lead to cardiac arrest if bicarbonate buffering cannot keep up with CO2 or hydrogen ion production. 16
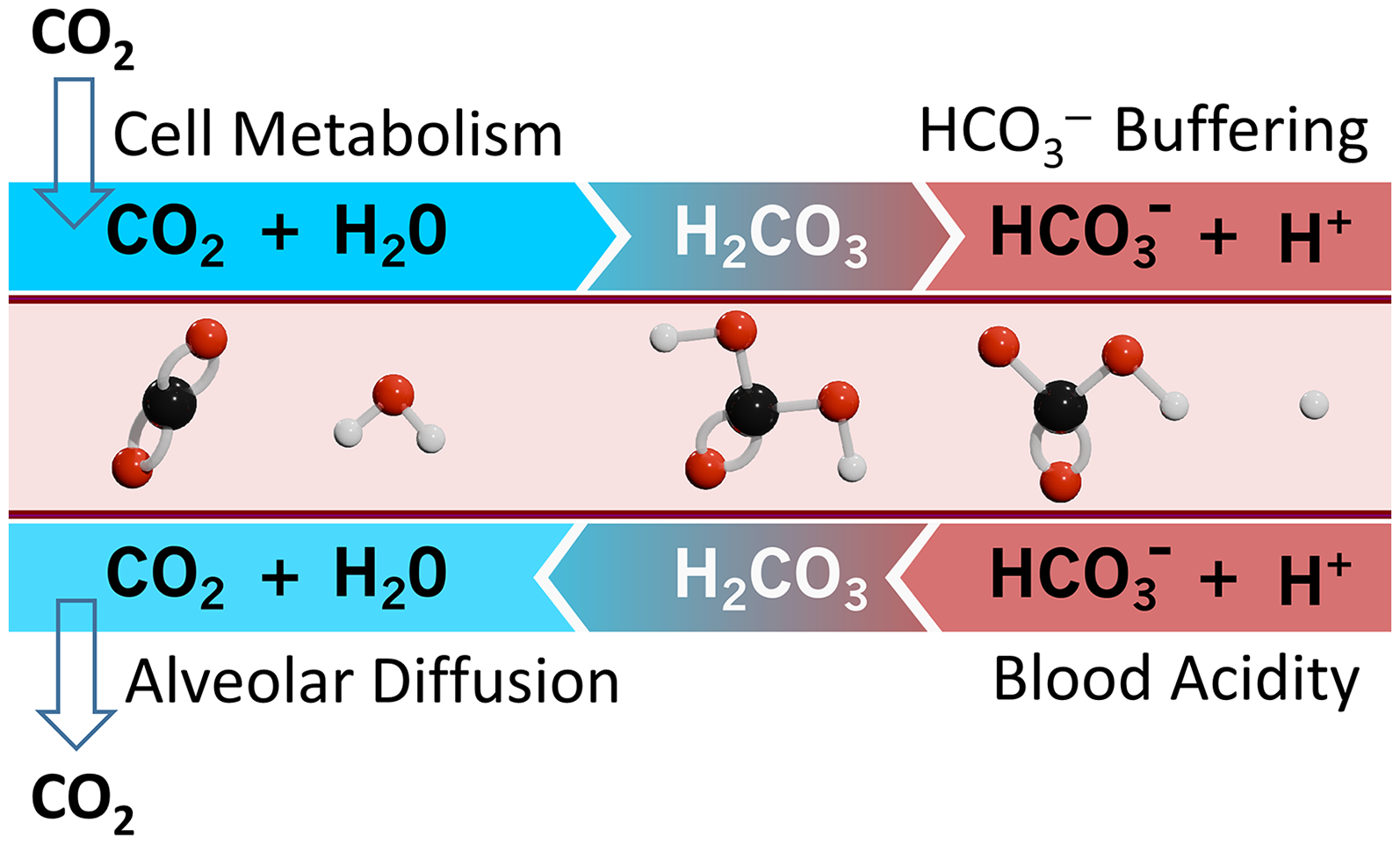
Metabolic production, blood buffering, transport and removal of CO2.
A major function of the kidneys is to prevent metabolic acidosis by removing hydrogen ions from the blood, although this normally occurs over a period of hours or days. A study which examined hydrogen ion concentration in the kidneys during intense exercise did not find any significant change in hydrogen ion concentration in the urine as the blood became more acidic, 17 although hydrogen ion concentration in the urine did increase significantly during recovery following exercise. This suggests that renal function would not contribute significantly to alleviating metabolic acidosis under conditions of prone restraint where the increased work of breathing and muscle activity involved in struggling are more akin to exercise than recovery.
Effect of prone position on gas exchange
The efficiency of alveolar O2 exchange is dependent on the ratio of ventilation (volume of air per unit time moving into the alveoli) to perfusion (volume of blood per unit time moving through the alveolar capillaries). There is evidence that in the prone position, compared to the supine position, there is a more uniform distribution of ventilation and perfusion along with improved matching of ventilation and blood flow and reduction in regions with low ventilation/perfusion ratios. 18 This may also be the case, but to a lesser extent, in comparing the prone position to upright standing or sitting positions. Although these effects of the prone position appear to improve alveolar O2 exchange, it is not clear that they have a significant effect on alveolar CO2 exchange, given the lower sensitivity of CO2 molecular content to CO2 partial pressure. Furthermore, although the prone position has been shown to reduce mortality in patients with respiratory disease, the mortality benefit is more likely related to reduced stress and strain on lung tissue leading to less lung injury rather than its effects on gas exchange. 18 Furthermore, there is no clear evidence that the prone position, itself, either positively or negatively impacts alveolar gas exchange, nor would it be expected in healthy individuals.
Effect of prone restraint on respiration
There has been considerable debate about restraint in the prone position on respiration. As suggested above, for a healthy individual, there is no evidence that the prone position is either beneficial or detrimental to gas exchange during respiration in a relaxed state. However, increased external pressure, such as that created by ground reaction force in the prone position, i.e., the reaction force exerted by the ground on the individual's body due to their weight, requires that the respiratory muscles perform more work than for respiration in a seated posture. In addition, the work that must be done by respiratory muscles increases because the torso is lifted upward by movement of the rib cage during inspiration. This adds to the work of breathing based on the amount of weight being lifted and the distance through which it is lifted, i.e., the amount of anterior expansion of chest wall. This added work of breathing will increase with respiration rate and respiration volume since work is done with each breath and increasing respiration volume requires greater movement of the rib cage. As an aside, it should be noted that the work of breathing in the prone position is less on a soft mattress than on solid ground (Appendix).
When a detainee is restrained in the prone position, the legs are frequently held down. One effect of holding down the legs, is that it prevents the detainee from lifting the pelvis and abdomen from the ground by preventing knee or hip flexion. Consequently, the detainee cannot reduce the ground reaction force on the thorax or abdomen, created by body weight and any downward force applied to the back. The ground reaction force creates internal pressure in the thoracic cavity against which the diaphragm must work during inspiration. This is in addition to the work that must be done to raise the center of mass of the upper body and any applied load. Therefore, even assuming that the detainee does not struggle, the work of breathing in the restrained prone position and, hence, the amount of CO2 being produced will be significantly higher than for a detainee restrained in a seated position.
A number of studies have been performed with the objective of determining whether or not restraint in the prone position has a detrimental effect on ventilation. Three of these studies examined the prone position,19–21 three examined the prone and prone restrained positions22–24 and the remaining studies examined the prone restrained position.25–28 Generally, these studies found that forced vital capacity (FVC), the volume of air that can be forcefully exhaled after maximum inspiration, was significantly reduced in the prone position without or with prone restraint. Furthermore, the amount by which FVC was reduced was greater when weight was applied to the back. This suggests that the total lung capacity is reduced in the prone position and the reduction increases with the load applied to the back.
In three of these studies21,23,28 recovery from exercise was compared in the prone or prone restrained position to the seated position. One of the measures which these studies included was either end tidal or arterial CO2 partial pressure during the recovery period. Cary et al. 21 found that end-tidal CO2 partial pressure was significantly higher in the prone than the seated position after two minutes of recovery. Although Chan et al. 28 examined arterial CO2 partial pressure during recovery from exercise, it cannot be assumed to represent a valid comparison between recovery in the prone restrained and seated restrained positions because the recovery began from statistically significant different baseline values of CO2 partial pressure. Sloane et al. 23 did not find any significant differences in end-tidal CO2 partial pressure between seated, prone or prone restrained positions during recovery from exercise. Roeggla et al. 27 measured end-tidal CO2 partial pressure while seated at rest and after 3 min of having been placed in the prone restrained position and found a significant increase in CO2 partial pressure after prone restraint. It should be noted that during submaximal exercise, changes in blood pH and CO2 partial pressure act to increase respiratory rate which tends to prevent CO2 partial pressure from increasing. The same regulatory mechanisms would be expected to continue to prevent CO2 partial pressure from increasing during recovery from exercise in prone or prone restrained positions. However, when subjects are placed in the prone restrained position without having performed any prior exercise, such as in the study of Roeggla et al., 27 blood pH and CO2 partial pressure are initially at resting-state levels. Consequently, an increase in CO2 production due to increased work of breathing could initially result in an increase in end tidal CO2 partial pressure since the regulatory mechanisms triggered by exercise would not be functional. Overall, the results of these studies suggest that in non-elderly healthy subjects at rest, the work of breathing is higher in the prone restrained position than sitting and that during relaxed recovery from exercise, CO2 partial pressure is similarly regulated whether sitting, prone or prone restrained, despite increased work of breathing when prone or prone restrained.
Campbell et al. 24 also investigated recovery after exercise, but under three different prone conditions. In two of the conditions, the subjects were restrained by a load of 35% their body weight placed on the upper back, either with their hands behind their back or behind their head. In the other condition, the subjects recovered in prone posture without a load and with their hands at their sides. This study focused only on changes in lung volume, i.e., it did not involve chemical measurements such as blood pH or gas partial pressure. Minute ventilation and difference in functional reserve capacity (ΔFRC) were estimated from reconstruction of lung volumes using electrical impedance tomography. FRC is the volume of air remaining in the lungs following expiration and ΔFRC, in this study, represented the difference in FRC under each condition compared to the relaxed prone position, i.e., prior to exercise or any load having been placed on the back. Minute ventilation increased in the prone position compared to upright standing, but decreased slightly when the load was placed on the back, although still greater than during upright standing. Following exercise, minute ventilation was much higher but decreased during recovery at a similar rate for all prone conditions. ΔFRC increased slightly when the load was placed on the back, prior to exercise, relative to the relaxed prone position, but was substantially reduced during recovery from exercise under all conditions. With the hands behind the back or the head and the load on the back, ΔFRC continued to decrease over the 5 min recovery period following exercise, whereas it remained constant in the prone recovery position without restraint (Figure 4).
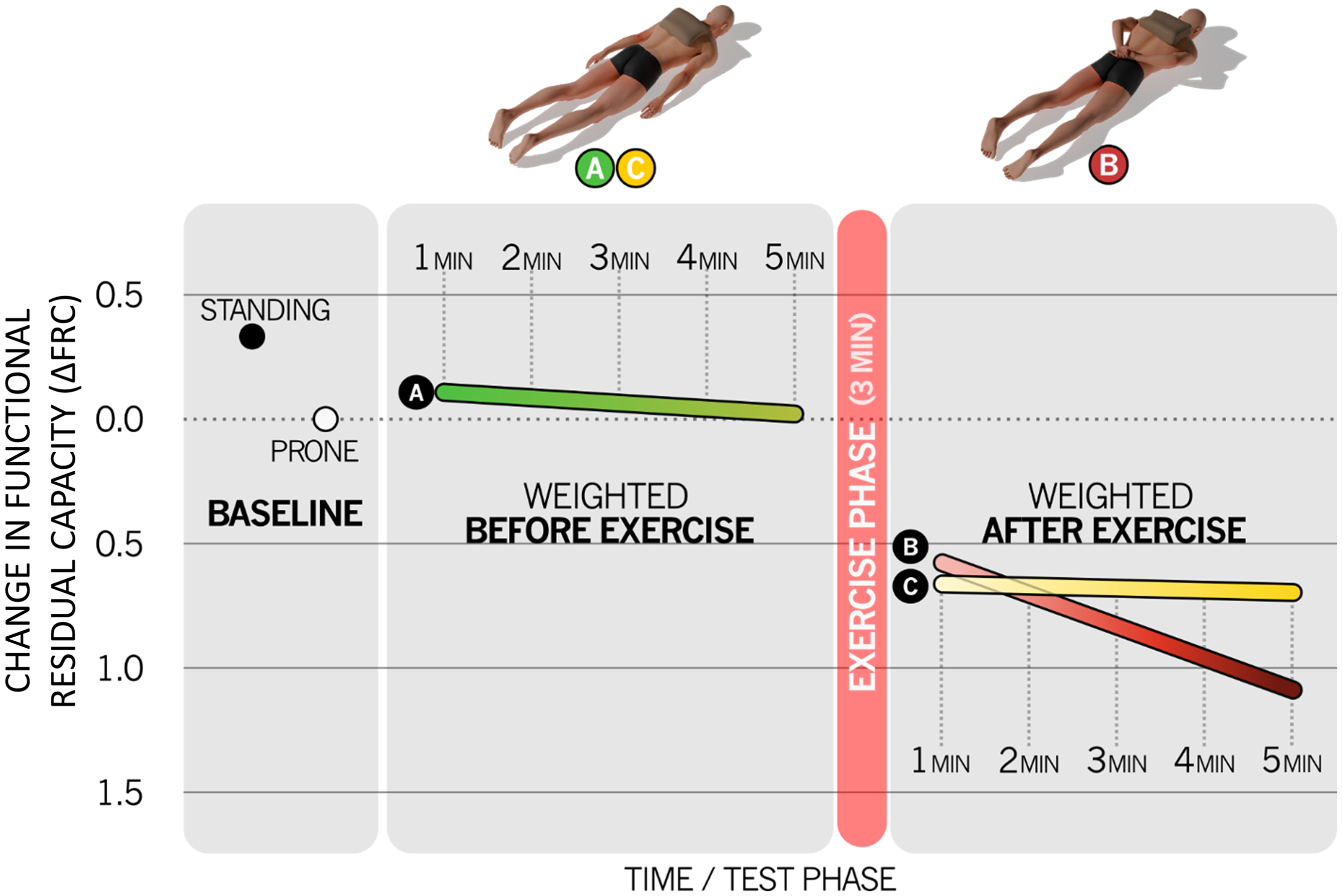
Effect of prone restraint on change in functional residual capacity.
The changes in minute ventilation were consistent with previous findings by Michalewicz et al. 26 on the effect of the prone position and load on maximum voluntary ventilation. The small reduction in ΔFRC in the prone position compared to upright standing was consistent with previous research that found lower FRC in the prone than sitting position. 29 The most significant finding of the study was the large initial reduction in ΔFRC under the combined effects of the load, exercise and prone positioning, which continued to decrease throughout exercise recovery when a load was placed on the back but not when there was no load on the back. This indicated that the work of breathing was higher in the restraint postures. Campbell et al. 24 suggested that this FRC reduction was due to an abdominal muscle recruitment strategy that decreases end expiratory lung volume to increase the efficiency of the diaphragm when more work must be done by inspiratory muscles. In addition, they suggested that the reason for the FRC decline seen during exercise recovery with the load and hands behind the back or head, but not in the unloaded recovery posture with the hands at the sides, was because the need for abdominal muscles to assist the diaphragm increased over time in a simulated prone restrained posture. Greater abdominal muscle activation during respiration would increase CO2 and hydrogen ion production, creating a greater risk of metabolic acidosis.
Sharp et al. 30 measured thoracic compliance (volume pressure curve) in the supine position with weights placed on the thorax or abdomen to increase external pressure. They found that the compliance remained the same when the weight was placed on the thorax but decreased when weight was placed on the abdomen. The effect of added weight would be expected to be similar to prone positioning where the ground reaction force rather than an added weight increases external pressure. Therefore, the work of breathing in the prone position should be higher than for a seated position because the respiratory muscles would be working against lower thoracic compliance, i.e., greater elastic resistance.
The work done by the muscles of a detainee restrained in the prone position while resting during recovery from exercise will be less than if the detainee is struggling. Struggling requires skeletal muscle activity, in addition to greater respiratory and cardiac muscle activity than during resting-state recovery. Consequently, CO2 and lactate production will increase and tax the capacity of physiologic mechanisms to counteract their effects on cardiac function to a greater extent than during resting-state recovery. Michalewicz et al. 26 simulated the scenario of a struggling detainee by having subjects perform a 60-s maximal struggle as an attempt to escape a hobble restraint while in the prone position. They measured minute ventilation, oxygen uptake and heart rate during the struggle and during an ensuing recovery period. During the struggle, minute ventilation, oxygen uptake, and heart rate all increased and subjects were reported to be hyperventilating by the end of the struggle. Values were expressed as percentages of peak values achieved during a treadmill test in which the incline was progressively incremented until the subject reached volitional fatigue. Group mean peak values for minute ventilation, oxygen uptake and heart rate during the struggle and ensuing recovery were 42%, 40%, and 84%, respectively, of the maxima achieved in the treadmill test. Michalewicz et al. 26 concluded that their subjects had adequate ventilatory reserve while struggling. However, there are several limitations to the study and how accurately it could replicate the scenario of a struggling detainee. First, the struggle was limited to 60 s, whereas prone restraint by law enforcement personnel may often exceed 60 s. Given that minute ventilation, oxygen uptake and heart rate were increasing up to or beyond the end of the 60 s struggle, it is likely that the peak values of these measures would be higher for a longer duration struggle. Furthermore, if an individual is detained after a pursuit, the detainee may already be physically exhausted prior to the onset of prone restraint. If, in addition, the detainee is in distress and already breathing rapidly after a struggle, it might not be possible for the detainee to increase respiratory rate sufficiently to compensate for the additional work of breathing and CO2 production, leading to worsening acidosis. Such conditions could not be simulated in the study. Second, although verbal encouragement was given to subjects, there was no objective measure to determine whether or not a subject was producing maximal effort. Third, the restraint was passive and provided some freedom of movement of the torso. This is in contrast to prone restraint where several law enforcement personnel actively respond to any movement which the detainee attempts, holding down the legs, arms and torso such that there is almost no freedom of movement. Fourth, the subjects were not experiencing distress. As the authors admitted, their simulated scenario “could not reproduce the psychological or other physiologic stresses associated with a field pursuit, struggle, or trauma.” Fifth, the study could not account for physiological effects of substance abuse or drug intoxication. A fundamental limitation of their study, is that their subjects were physically fit drug-free young adults, whose demographics are unlikely to be well matched to the demographics of the detainees who would be most susceptible to prone restraint cardiac arrest.
The research reviewed to this point indicates that a struggling young healthy individual, restrained in the prone position with a load on the back, will be performing more work to breathe than in an unrestrained seated or standing posture. The prone position, the position of the arms, the load on the back, the effort of struggling and the duration of the restraint contribute additively to the work of breathing. Furthermore, the research findings point to the work necessary for expiration having a greater impact on the added work of breathing than the work necessary for inspiration, i.e., the cardiopulmonary system is working harder because there is a greater need to remove excess CO2 (hypercapnia) as opposed to inspiring more O2 (hypoxia). Because of the large difference in O2 partial pressure between inspired air and mixed venous blood in the alveolar capillaries, O2 readily binds to deoxygenated hemoglobin as it diffuses into the alveolar capillaries. Any increase in CO2 partial pressure or blood acidity will reduce the affinity of hemoglobin for O2 which will enhance the unloading of O2 from the circulating blood into tissues to meet their O2 demand. Thus, even when excess CO2 accumulates in the blood (hypercapnia), O2 demand can still be met, preventing hypoxia.
Effect of obesity on prone restrained respiration
It has been shown that obesity reduces lung volumes, including total lung capacity, FRC and expiratory residual volume, measured while seated.31–33 The amount by which these lung volumes are reduced increases with the degree of obesity. It would, therefore, be expected that the effects of prone restraint on respiration would be more pronounced in obese than non-obese individuals. With the exception of the study by Sloane et al., 23 research on the effect of prone restraint on respiration has been conducted with subjects who were not identified as being obese. As in many of the other studies, Sloane et al. 23 compared the effect of the prone position and prone restraint on recovery from exercise. Their study investigated respiration under conditions of prone restraint in subjects with a mean BMI of 35.4 kg/m2, bordering on Class 2 obesity. They measured heart rate, minute ventilation, O2 saturation and end tidal CO2 partial pressure, but found no significant differences between recovery from exercise while seated compared to prone or prone restrained. However, since they did not report respiratory rates it is unclear whether recovery in the seated and prone positions was achieved with the same tidal volume. The study did not address the issue of respiration with a load on the back or respiration while struggling while prone restrained.
In order to compensate for the increased production of CO2 during exercise, minute ventilation increases. Increases in tidal volume and respiration rate occur in response to increasing production of CO2 by working muscles during exercise. During mild exercise minute ventilation increases predominantly by increasing tidal volume with modest increases in respiration rate whereas during more strenuous exercise, tidal volume plateaus when it reaches approximately 50%–60% of vital capacity and additional increases in minute ventilation are achieved solely by increases in respiration rate. 9 Therefore, any reduction in tidal volume of a struggling prone restrained detainee would have to be compensated by a higher than normal respiration rate in order to achieve the minute ventilation necessary to remove sufficient CO2 from the mixed venous blood to prevent respiratory acidosis. The results of the study by Littleton and Tulaimat, 33 which found reduction in total lung capacity with obesity, combined with the previous findings of reduction of FVC in the prone position, imply that struggling, prone restrained obese individuals will require a higher respiration rate than non-obese individuals in order to prevent respiratory acidosis. In addition to the higher respiration rate, the increased work of expiratory muscles inferred by Campbell et al. 24 from the reduced FRC under prone restraint, implies that struggling obese individuals, under prone restraint, must perform more work to breathe than non-obese individuals. Furthermore, the higher respiration rate reduces the efficiency of gas exchange because it effectively increases the total anatomical dead space, i.e., the volume of inspired air which is not available for gas exchange. 12
A potential aggravating factor with obesity is that intra-abdominal pressure tends to increase with the degree of obesity and becomes higher in the prone position.10,34 Although there is no clear consensus of the effect of increased intra-abdominal pressure on resting respiration in the prone position, 34 it is likely that under conditions of high respiratory demand, such as struggling, the workload on the diaphragm would be higher while prone-restrained than while seated.
Both lung compliance and chest wall compliance are reduced in morbidly obese individuals compared to non-obese individuals. 35 During exercise, obese subjects preferentially increase their respiration rate more, and tidal volumes less, than non-obese subjects. 36 This compounds the effect of lower overall lung compliance by breathing in a lung volume range where the already lower compliance is even farther from optimal. The lower the lung compliance the greater the work of breathing, which likely exacerbated in the prone position where the ground reaction force on the abdomen will have a similar effect to a weight placed on the abdomen, reducing thoracic compliance. 30 Consequently, CO2 production will be significantly higher for an obese than non-obese detainee who is restrained and struggling.
Effect of panic on prone restrained respiration
Prone restrained detainees are frequently in distress and may panic if they begin to experience difficulty breathing. The respiratory response to panic itself may affect respiration, independent of any other physical reaction that it might elicit. It is important to note that a physical reaction, such as struggling, does not necessarily constitute an attempt to escape. A physical reaction may be an attempt to achieve a posture that is more favorable for respiration. Although it may not be ethically permissible to design a study that investigates the the effect of true panic on respiration, studies have examined the effect of stressful situations on respiration. Psychophysiological stress-induced respiratory reactions produce changes in ventilation which often precede changes in metabolic processes. 37 The most consistent respiratory response to laboratory-induced panic attacks is hyperventilation. 38 An increase in respiration rate is seen with anxiety produced by breathlessness and mechanical discomfort 39 and is particularly prevalent in individuals with high baseline levels of anxiety. Severe anxiety or panic can be induced by a state of paralysis, such as that experienced by patients during awareness under general anesthesia.40,41 Being actively held down during prone restraint without the ability to move the legs, arms or torso is in a way analogous to paralysis and may trigger a reaction of panic similar to that reported by the patients in the studies of Moerman et al. 40 and Schwender et al. 41 The effect of increasing respiration rate has been previously discussed. It reduces the efficiency of gas exchange by effectively increasing the anatomical dead space, i.e., the volume of air not available for gas exchange, as well as increasing the work of breathing.
Effect of drug intoxication on prone restrained respiration
Substance use can also contribute to the accumulation of CO2 in the blood. Opioids, such as oxycodone and fentanyl can depress respiration, reducing the volume of air moving in and out of the lungs. 42 Methamphetamine, on the other hand, increases heart rate and reduces the capacity of the cardiovascular system to appropriately respond to increased levels of CO2 in the blood. 43 In particular, the cardiac baroreflex range is significantly reduced with methamphetamine intoxication. One function of the cardiac baroreflex is to regulate the heart rate in response to changes in blood pressure which increases with increases in CO2 partial pressure. 44 Reduction in the range over which the cardiac baroreflex can operate implies a reduction in the heart rate response to increased CO2 partial pressure. Furthermore, chronic substance use may result in lung or heart disease45–48 which could limit the ability of the detainee's cardiopulmonary system to respond effectively to increases in the work of breathing or CO2 production during prone restraint. Overall, substance use can reduce the ability to remove CO2 from the blood, increasing the risk of respiratory acidosis. Furthermore, chronic substance use, including heavy alcohol consumption, is an important risk factor for cardiac arrhythmia.49,50 Therefore, detainees with a history of substance use are likely to be at greater risk of cardiac complications while prone restrained, which could be exacerbated by elevated blood potassium levels, as plasma potassium concentration is known to increase during exercise.17,51 High systemic potassium concentration can lead to heart block, asystole and ventricular tachycardia and ventricular fibrillation. 52
Summary
The two primary effects of the prone position, relevant to respiration, are a decrease in ventilation, including a decrease in maximal voluntary volume, which is exacerbated by restraint, and reduced thoracic compliance due to increased abdominal pressure. These factors together with the added work of raising the upper body during respiration increase the work of breathing relative to a seated or upright posture and reduce the ability to expire CO2. Empirical studies indicate that the cardiopulmonary system is able to effectively compensate for this added work under conditions of passive prone restraint with an added load or during recovery from exercise, although no study on prone restraint has reported its effect on blood pH. Physical exertion, while passively prone restrained has been investigated in one study which found effects similar to incrementally increasing exercise intensity, i.e., monotonically increasing heart rate, oxygen consumption and minute ventilation. It can, therefore, be assumed that a detainee, struggling while prone restrained, will exhibit similar physiological changes as during incrementally increasing exercise, e.g., reduced blood pH. However, the study examined only a 60-s struggle so it is not clear whether physiological changes would continue to parallel the same trends as for incremental exercise during a longer duration struggle.
All of the studies that investigated respiration under conditions of prone restraint, to date, lack key features that preclude accurate replication of a scenario in which a detainee would be at risk of cardiac arrest. All of the cited studies involved passive restraint. Active restraint in which law enforcement personnel are shifting their positions and varying the magnitude and direction of the load which they are applying to the detainee in order to prevent any movement of the legs, arms or torso is very different from being hobbled but free to roll the body and the difference is likely aggravated with obesity. Recovering from exercise, while relaxed with a passive restraint, is very different from struggling against unpredictably varying loads applied to the body. None of the cited studies involved any form of psychological distress and subjects were drug-free younger healthy individuals.
In reviewing the physiology of the cardiopulmonary system in response to exercise and prone positioning, it is apparent that struggling, obesity, anxiety or panic, and drug intoxication represent risk factors for accumulation of CO2 in the blood, possibly taxing the ability of the bicarbonate buffer system to adequately neutralize carbonic acid and lactate, resulting in increasing blood acidity (Figure 5). The rate of CO2 production because of increased work of breathing, together with the production of CO2 and hydrogen ions as the result of struggling, resistive loads and high respiration rate may overwhelm the physiological processes responsible for maintaining blood homeostasis, particularly if these processes are impaired by obesity or drug intoxication. In such situations, it is possible that blood pH falls to levels of severe respiratory or metabolic acidosis, resulting in irregular cardiac function and cardiac arrest.

Contrast between respiration demands under simulated prone restraint conditions in a lab setting (left) and under realistic true life prone restraint conditions (right).
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix
The work, W, which the respiratory muscles perform to expand the chest by an amount, d, in the anterior direction, during inspiration in the prone position, is equal to the weight of the upper body together with any downward load applied to the upper body, F, multiplied by the distance which it must be raised
On a mattress, the work to move the chest in the anterior direction involves a combination of compressing the mattress and raising the upper body. The equation for the work now becomes
Therefore, the work of breathing in the prone position on a mattress, compared to solid ground, would be reduced by 0.5Fx. The greater the compliance of the mattress, i.e., the softer the mattress, the more it will be compressed. Hence, the greater the value of x, the greater the reduction in the work of breathing in the prone position.