
Abstract
Objective
Individuals vary in response to sleep loss: some individuals are “vulnerable” and demonstrate cognitive decrements following insufficient sleep, while others are “resistant” and maintain baseline cognitive capability. Physiological markers (e.g., genetic polymorphisms) have been identified that can predict relative vulnerability. However, a quick, cost-effective, and feasible subjective predictor tool has not been developed. The objective of the present study was to determine whether two factors—“subjective sleep need” and “subjective resilience”—predict cognitive performance following sleep deprivation.
Methods
Twenty-seven healthy, sleep-satiated young adults participated. These individuals were screened for sleep disorders, comorbidities, and erratic sleep schedules. Prior to 40 hours of in-laboratory total sleep deprivation, participants were questioned on their subjective sleep need and completed a validated resilience scale. During and after sleep deprivation, participants completed a 5-minute psychomotor vigilance test every 2 hours.
Results
Both subjective resilience and subjective sleep need individually failed to predict performance during sleep loss. However, these two measures interacted to predict performance. Individuals with low resilience and low sleep need had poorer cognitive performance during sleep loss. However, in individuals with medium or high resilience, psychomotor vigilance test performance was not predicted by subjective sleep need. Higher resilience may be protective against sleep loss-related neurobehavioral impairments in the context of subjective sleep need.
Conclusions
Following sleep loss (and recovery sleep), trait resilient individuals may outperform those with lower resiliency on real-world tasks that require continuous attention. Future studies should determine whether the present findings generalize to other, operationally relevant tasks and additional cognitive domains.
Introduction
Sleep loss is ubiquitous in modern society (Bixler, 2009) and is especially prevalent in certain occupations, including night shift workers, emergency workers, and military personnel. Such occupations often require long hours of work—sometimes during the night—when alertness and performance decrements result from the combined effects of sleep loss and circadian misalignment (Arendt, 2010; Caruso, Hitchcock, Dick, Russo, & Schmit, 2004). Sleep subserves waking functioning, and sleep loss has a well-documented negative effect on cognitive performance, especially on tasks requiring sustained attention and vigilance (Basner & Dinges, 2011; Dinges, Rogers, & Dorrian, 2004). However, the extent to which sleep loss impacts cognitive performance varies across individuals (Rupp, Wesensten, & Balkin, 2012; Van Dongen, Baynard, Maislin, & Dinges, 2004). These interindividual differences can be considerable, and potentially consequential, as they could, in some operational environments, constitute the margin between success and catastrophic failure.
Factors associated with relative “resistance” to the effects of sleep loss include longer habitual sleep duration (Rupp, Wesensten, Bliese, & Balkin, 2009), better executive functioning at baseline (i.e., without sleep loss) (Killgore, Grugle, Reichardt, Killgore, & Balkin, 2009), and extraversion (Killgore, Richards, Killgore, Kamimori, & Balkin, 2007). Additionally, several studies have shown genetic polymorphisms, such as PER3, predict vulnerability to sleep loss (Groeger et al., 2008; Lo et al., 2012; Viola et al., 2007). Although these studies diverge in methodology and outcome measures, each suggests that vulnerability to the effects of sleep loss is a stable, and identifiable, “trait” within individuals.
In most studies to date, vulnerability to sleep loss has been determined in a post hoc manner. That is, study participants have typically been exposed to sleep loss (e.g., restriction or deprivation) and categorized as sleep loss vulnerable or resistant on the basis of their relative ability to sustain performance or avoid falling asleep in sleep-conducive conditions (e.g., Killgore et al., 2009). However, in some studies, prospective prediction of subsequent vulnerability to sleep loss has been achieved using genetic markers (i.e., PER3, Viola et al., 2007). Yet the extent to which vulnerability to sleep loss can be predicted based on ad hoc subjective measures remains largely unknown and untested. Accordingly, the purpose of the present study was to determine the relationship between two factors—“subjective sleep need” and “subjective resilience”—and cognitive performance during and after sleep deprivation.
Resilience
Subjective resilience was selected as a candidate measure that could potentially predict vulnerability to the effects of sleep loss. Several definitions of resilience have been proposed. Johnston et al. (2015) posited that “resilience involves maintaining healthy levels of functioning following adversity and that it is a dynamic process, not a personality trait” (Johnston et al., 2015), while Windle (2011) defines resilience as “. . . the process of effectively negotiating, adapting to, or managing significant sources of stress or trauma” with this construct providing the capacity for “adaptation and ‘bouncing back’ in the face of adversity.” In addition, and more succinctly, Connor and Davidson (2003) consider resilience to be the broad capacity to successfully adapt to risk and adversity (Connor & Davidson, 2003).
Although these definitions diverge somewhat, in each of these conceptualizations—resilience is considered a “strength” that is manifest only during exposure to conditions/events characterized by extraordinary physical and/or psychological threat or adversity, and its manifestation effectively prevents or reduces harmful consequences of such exposures (Fergus & Zimmerman, 2005). Sleep loss, which is a physiological, emotional, and cognitive stressor, constitutes a condition in which it is reasonable to hypothesize that individual differences in trait resilience might predict vulnerability or resistance to how an individual is impacted by sleep loss. In support of this notion, in a recent study in Veterans, a strong relationship was detected between subjective sleep quality and psychological distress, but the relationship was buffered by high resilience (Hughes et al., 2018). The authors suggested that negative outcomes caused by poor sleep may be less severe in individuals with high trait resilience. Based on these data, we surmise that resilience may be predictive of performance under conditions of sleep loss.
Subjective sleep need
Subjective sleep need is another factor that may underlie individual differences in sensitivity to sleep loss. It is thought that physiological sleep need—which could be defined as the amount of sleep time one needs to sustain functioning within normal limits—is largely under genetic control (Franken, Chollet, & Tafti, 2001). However, although physiological sleep need might reasonably be inferred from habitual total sleep times (i.e., by having an individual sleep until they no longer can), subjective sleep need is a more difficult construct to define.
Subjective sleep need is often confounded with sleepiness, which is the propensity to fall asleep at a given time. In his review, Horne (2010) suggested that subjective sleepiness does not necessarily reflect a basal need to sleep. Instead, sleepiness is a volatile state that can be reduced or reversed, whereas sleep need is a relatively stable trait (Horne, 2010). Nevertheless, it is reasonable to hypothesize that subjective sleep need is dependent upon, and thus more or less reflects, physiological sleep need (in normal, non-sleep-disordered individuals). Therefore, simply asking an individual how much sleep they need to function properly may be predictive of performance during subsequent sleep loss.
The current study
Here, we aimed to assess the extent to which subjective resilience and subjective sleep need predict performance on psychomotor vigilance test (PVT) after total sleep deprivation and following recovery sleep. We also tested, in an exploratory manner, whether subjective sleep need and resilience interact to predict performance outcomes. It was hypothesized that high resilience would predict better performance after sleep loss and after a period of recovery sleep. It was further hypothesized that low subjective sleep need would predict better performance following sleep loss and recovery sleep. Lastly, it was hypothesized that resilience would interact with subjective sleep need: individuals with low subjective sleep need and high subjective resilience would best be able to sustain performance during sleep deprivation, whereas, conversely, the performance of individuals with high subjective sleep need and low subjective resilience would be poor during sleep deprivation.
Methods
This study was approved by the Walter Reed Army Institute of Research Human Use Review Committee and the United States Army Medical Research and Materiel Command Human Subjects Research Review Board and was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki.
Participants
Men and women, 18 to 39 years of age (mean 24.37 ± 5.41), were recruited via flyers posted at local colleges, universities, and military installations. Twenty-seven adults (40.7% (11 of 27) females) participated.
After providing informed consent, volunteers underwent a physical examination, and evaluation of blood and urine samples was conducted to determine general health status (including pregnancy and drug use status). Volunteers additionally completed a screening for sleep disorders in the laboratory using a portable home sleep testing equipment before starting the study.
Volunteers were excluded if they reported any of the following for the preceding month: (1) habitual nightly sleep amounts outside the range of 6–9 hours on weeknights, (2) average morning wake-up times later than 9:00 a.m. Monday through Friday, (3) average nighttime lights-out times earlier than 9:00 p.m. Sunday through Thursday, or (4) average habitual napping of greater than three times a week. Additional exclusionary criteria included cardiovascular disease; hypertension; past/present neurologic or sleep disorder; psychiatric disorder within the past three years, an Apnea/Hypopnea Index of ≥5 during a diagnostic sleep test conducted during the screening phase, present/past use of over-the-counter substances with purported psychoactive properties; use of sleep-aids within the last two years; regular nicotine use within the last year; current heavy alcohol use (>14 drinks per week); current use of other drugs (including benzodiazepines, amphetamines, cocaine, and marijuana); medication use during in-laboratory challenge phases (including use of vitamins/supplements; not including oral contraceptives); liver and kidney disease/abnormalities; underlying pulmonary disease requiring daily inhaler use; clinically significant values for any screening hematology or chemistry parameter, body mass index ≥30; self-reported history of caffeine use >400 mg (eight caffeinated sodas or three to four cups of coffee) per day on average; score ≥14 on the Beck Depression Inventory; score ≥41 on the Speilberger State-Trait Anxiety Inventory, score <31 or >61 on the Horne–Ostberg morningness–eveningness questionnaire, or current breast feeding or pregnancy. Additionally, subjects who screened positive for nicotine, alcohol, or illicit drugs at the screening visit were excluded from participation. Subjects who were unable to read and sign the informed consent document were excluded as well.
Experimental design
This study was part of a larger experiment aimed at testing the impact of sleep extension and subsequent sleep deprivation on inflammatory markers. Data from the sleep extension phase of the study are presented elsewhere (Devine et al., 2019; Mantua et al., 2019; Simonelli et al., 2019) and were not within the scope of the current investigation. Therefore, limited data from this phase are presented here. The full study consisted of one at-home 14-day phase with wrist actigraphy followed by three consecutive in-laboratory within-subject phases. During the first phase, subjects wore wrist actigraphs continuously for 14 days and were instructed to maintain their typical sleep/wake schedules. This phase was included to ensure participants slept “normally” (i.e., did not have an erratic circadian rhythm or short/long sleep time). During the second phase, in the laboratory, participants were provided a baseline sleep opportunity (“Baseline”; 23:00 to 07:00, 8 hours of time in bed (TIB)) for two nights to facilitate adaptation to the laboratory. Subsequently, participants underwent seven nights of sleep extension (“Extension”; 21:00 to 07:00, 10 hours TIB) followed by one night of total sleep deprivation (“Deprivation”; 40 hours of continuous wakefulness) and a 10-hour TIB recovery sleep period (“Recovery”).
Measures
The Connor–Davidson Resilience Scale (CD-RISC) was used to measure subjective resilience. This measure has 25 items, each with a five-point scale (ranging from 0 to 4). Participants were asked to rate themselves on hardiness-focused items, such as “how easily are you discouraged by failure?” A higher number indicates greater resilience. This measure has a Cronbach’s alpha of .89, test–retest reliability (intraclass correlation) of 0.87 and is correlated with measures of levels of hardiness and vulnerability to stress (Connor & Davidson, 2003). Participants were also asked an open-ended question about their sleep need. Specifically, participants were asked to complete this statement: “If you get less than __x__ hours of sleep, you notice an impairment in your ability to function at work/school.”
Neurobehavioral performance was measured with a computer-based 5-minute PVT repeatedly throughout in-laboratory portions of the study. PVT data were collected at multiple time points during Baseline (at 07:00, 09:00, 11:00, 13:00, 15:00, 17:00, 19:00, and 21:00 hours) and twice per day during the Extension period (07:00 and 20:00 hours). PVT data presented in this study were obtained during the last 20 hours of the 40-hour sleep deprivation period, across 20 continuous hours of wakefulness (at 01:00, 03:00, 05:00, 07:00, 09:00, 11:00, 13:00, 15:00, 17:00, 19:00, and 21:00 hours). These data were averaged to create a single PVT value (to remove variation from circadian factors). Additionally, a single PVT was administered following recovery sleep (at 09:00 hours). Measures of interest included PVT speed (defined as 1/reaction time × 1000) and PVT lapses (the number of responses >500 milliseconds).
Statistical analyses
SPSS 23 software (Armonk, NY) was used to conduct statistical analyses. Results with a p value <.05 were considered statistically significant.
Given that subjective sleep need is an unvalidated measure, we used Pearson’s correlations to determine whether this variable correlated with objective sleep data from the 14-day at-home phase. Subjective sleep need (hours) was correlated with average nightly sleep duration, weeknight sleep duration, and weekend sleep duration.
A repeated-measures analysis of variance (ANOVA) was used to test whether PVT performance differed as a function of Condition (Baseline, Extension, Deprivation, and Recovery). If the omnibus ANOVA was significant, post hoc tests were conducted using the Least Significant Difference test. Because our hypotheses focused on response to Deprivation and Recovery, information outside the scope of these questions (e.g., PVT during Baseline and Extension) are only presented descriptively and are not a part of the main regression analyses.
Linear regression was used to determine whether resilience (CD-RISC scores) and sleep need (hours) predicted PVT performance. Outcome measures were (1) PVT speed after sleep Deprivation, (2) speed after Recovery, (3) number of lapses after Deprivation, and (4) number of lapses after Recovery. Moderation analyses were conducted to determine whether resilience moderates the relationship between subjective minimum sleep need hours and PVT performance during and after sleep loss. These analyses were conducted using the SPSS PROCESS macro (Model 1, as shown in Hayes, 2012). In this model, X = subjective minimum sleep need (hours), Y = PVT performance (the four aforementioned outcome measures), and M = resilience (CD-RISC scores).
PROCESS calculates statistical significance using 95% confidence intervals to determine the effect of the predictor on the outcome measure. PROCESS also calculates the interaction effects of the moderators by testing the predictive effect of each factor at different levels (e.g., in this case, low resilience and low subjective sleep need, or low resilience and high subjective sleep need). Each predictor level was determined by values plus or minus 1 standard deviation from the centered mean. To eliminate possible statistical assumption violations, 5000 bootstrap iterations were used (at least 2000 bootstrap iterations are recommended (DiCiccio & Efron, 1996). Effect size (B), standard error (SE), and 95% confidence intervals (95%CI) are reported.
Results
Questionnaires
By design, per the screening criteria, on the MEQ, there were no participants in the “definite morning” (score 70–89) or “definite evening” (score 16–30) range. Seven participants (26%) were “moderate morning” types (score 59–69), 19 participants (70%) were “neither,” and 1 participant (4%) was a “moderate evening” type. All the participants had an apnea–hypopnea index of less than 5.
Participants had CD-RISC scores of 79.56 ± 10.61 (range 60–97), comparable to a previously studied healthy population (Connor & Davidson, 2003). Participants reported a mean subjective sleep need of 4.6 ± 1.3 hours (range 2–7) hours of sleep.
Sleep
In the 14-day at-home phase, participants averaged 452.32 ± 53.11 minutes (7.53 hours) of sleep per night, consistent with a “healthy” sleep duration (according to the American Academy of Sleep Medicine and the Sleep Research Society; Panel et al., 2015). Subjective sleep need was not correlated with habitual nightly sleep time (r = .08, p = .70) or habitual weeknight duration (r = .22, p = .28). However, subjective sleep need was positively correlated with weekend sleep duration (r = .40, p = .04), indicating individuals who feel they need more sleep obtained more sleep during the weekend.
During the in-laboratory baseline night, participants slept 465.92 ± 35.59 minutes (7.75 hours), which was not significantly different from the at-home phase. During the sleep extension phase, however, participants slept an average of 561.67 ± 33.87 minutes (9.36 hours) per night, significantly more than during the at-home phase (p < .001). All participants successfully remained awake during the 40-hour sleep deprivation period. Subsequently, participants slept 580.57 ± 37.54 minutes (9.68 hours) during the recovery sleep period.
Neurobehavioral performance
Performance on the PVT is listed in Table 1. The omnibus ANOVAs revealed a main effect of Condition for speed (F(3,78) = 51.65, p < .001). Post hoc tests showed that speed was significantly faster during Extension than during Baseline. Speed was significantly slower during Deprivation than at Baseline. Speed did not differ between Baseline and Recovery, indicating performance had normalized to Baseline (but remained slower than speed during Extension) following Recovery.
Psychomotor vigilance test performance (mean ± standard deviation) and statistical results testing differences from baseline.
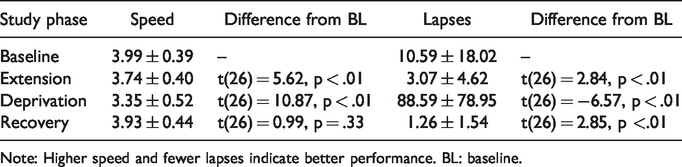
Note: Higher speed and fewer lapses indicate better performance. BL: baseline.
Similar to speed, number of lapses varied significantly by Condition (F(3,78) = 34.65, p < .001), and post hoc tests revealed that all conditions differed significantly from each other. There were significantly fewer lapses during the Extension and Recovery phases than during Baseline, and there were significantly more lapses during Deprivation than during Baseline.
Resilience, subjective sleep need, and performance
Linear regressions were performed to determine whether resilience and subjective sleep need predicted performance after sleep loss and after recovery sleep. Contrary to predictions, subjective resilience did not predict speed after sleep loss (p = .94) or recovery sleep (p = .96). Nor did subjective resilience predict number of lapses after sleep loss (p = .48) or recovery sleep (p = .15). Therefore, overall, resilience, in isolation, was not a predictor of PVT performance after sleep loss or recovery sleep.
Similar results were obtained for subjective sleep need. Sleep need did not predict speed after sleep loss (p = .22) or recovery sleep (p = .29). Additionally, sleep need did not predict lapses after sleep loss (p = .16) or after recovery sleep (p = .89). Taken together, these results indicate that subjective sleep need alone does not predict PVT performance after sleep loss or recovery sleep.
We next assessed whether resilience moderates the relationship between minimum subjective sleep need hours and PVT performance. We first tested whether a moderation was present for PVT speed. After sleep deprivation, resilience was a significant moderator, as indicated by a statistically significant increase in R2 as a result of the interaction (Table 2). Post hoc analyses revealed that at low levels of resilience (but not at medium or high levels of resilience), sleep need significantly predicted speed. As shown in Figure 1, in individuals with low resilience, low sleep need predicted lower PVT speed (poorer performance). On the other hand, in individuals with high resilience, there was no relationship between sleep need and PVT performance. The moderation was not significant for speed following recovery sleep.
Interaction statistics, with each row representing a separate model.
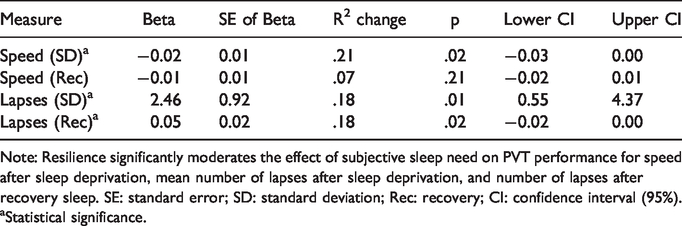
Note: Resilience significantly moderates the effect of subjective sleep need on PVT performance for speed after sleep deprivation, mean number of lapses after sleep deprivation, and number of lapses after recovery sleep. SE: standard error; SD: standard deviation; Rec: recovery; CI: confidence interval (95%).
Statistical significance.
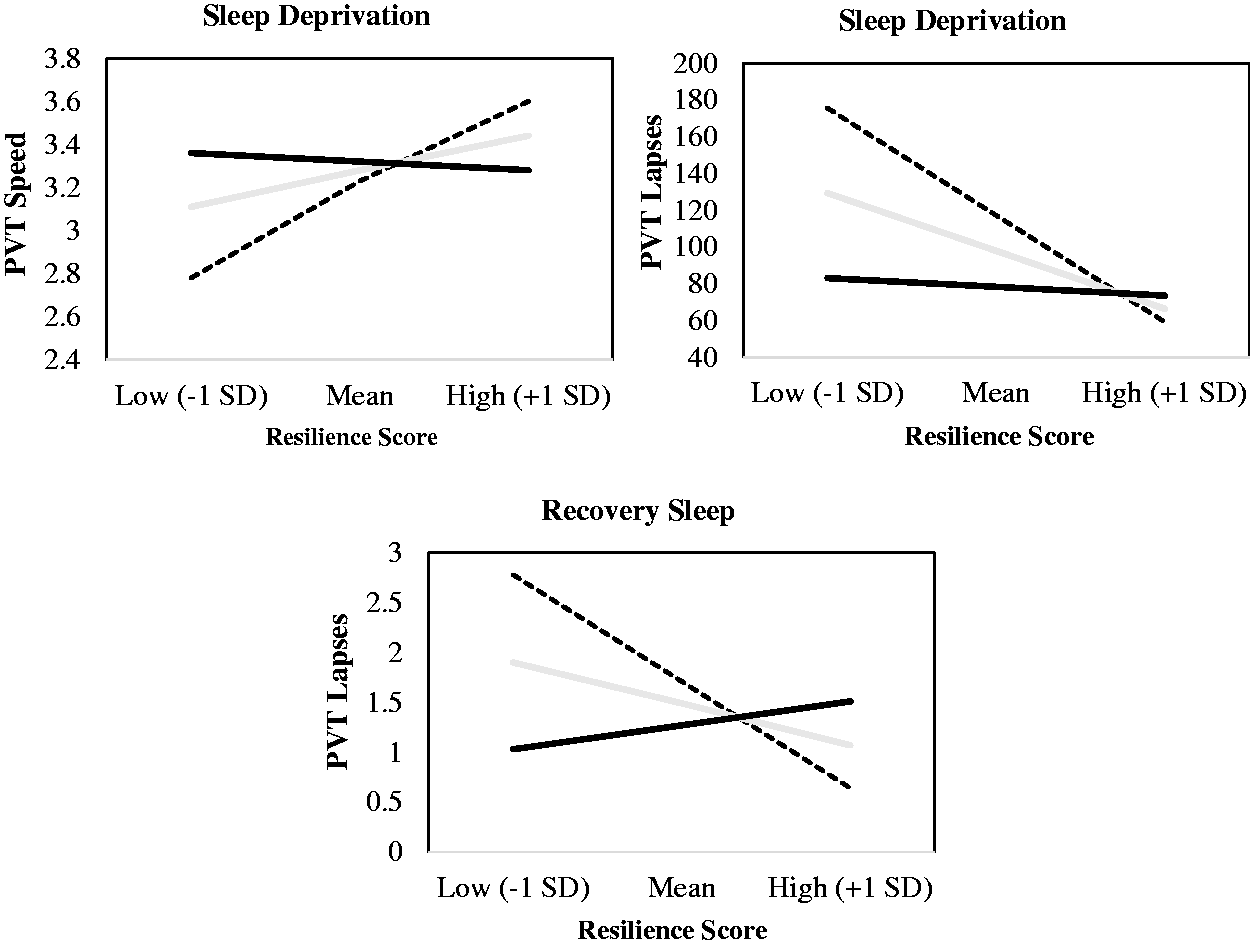
Graphical representation of the moderation analysis. The dashed line represents low sleep need, the gray line represents the mean sleep need, and the black line represents high sleep need. Higher speed (1/reaction time × 1000) and fewer lapses indicate better performance. SD: standard deviation; PVT: psychomotor vigilance test.
Similarly, for PVT lapses, resilience significantly moderated the relationship after sleep deprivation and recovery (Table 2). Similar to what was reported above, at low levels of resilience, sleep need significantly predicted lapses after deprivation, and recovery, but not at medium or high levels of resilience. Consistent with the reported previous results, in individuals with low subjective resilience, low sleep need predicted a higher number of PVT lapses (poorer performance), but there was no significant relationship between sleep need and lapses in more resilient individuals.
Discussion
Interindividual differences in responsivity to sleep loss appear to be trait-like, as some individuals are measurably impacted by sleep loss, while others are not (Rupp et al., 2012; Van Dongen et al., 2004). In the current study, we attempted to predict cognitive performance (i.e., vigilance/attention) after sleep loss and after subsequent recovery sleep using two ad hoc subjective measures: resilience and sleep need, with mixed results. First, contrary to our hypothesis, we found that resilience alone was not a significant predictor of PVT performance after sleep deprivation or recovery sleep. High resilience is predictive of a number of positive outcomes, including fewer symptoms after traumatic brain injury (McCauley et al., 2013), better post-war psychological outcomes in soldiers (Elliott et al., 2015), and the ability to thrive psychologically in the face of adversity (Jackson, Firtko, & Edenborough, 2007). Consequently, much effort has been put into increasing trait resilience with the rationale that increased resilience will lead to positive downstream benefits (Fitzwater, Arthur, & Hardy, 2018; Nindl et al., 2018). The results presented here indicate that the CD-RISC resiliency questionnaire, in isolation, is not sufficient to identify individuals who are cognitively resistant to sleep loss.
Similarly, subjective sleep need alone was not found to be a significant predictor of PVT performance. Previous studies on the utility of subjective sleep need as a construct have been inconsistent. Several studies have linked self-reported sleep need with functional outcomes. For instance, in a large sample of young adults, a greater discrepancy between objective sleep duration and subjective sleep need was related to lower feelings of restoration (Kalak, Brand, Beck, Holsboer-Trachsler, & Wollmer, 2015). Furthermore, a separate study found that “sleep credit”—a composite measure of subjective sleep need and subjective recent sleep duration—is linked with better mental health symptoms (Weber et al., 2013). However, contrary to the studies described above, in two studies, sleep need was not associated to feelings of fatigue nor to sleep insufficiency (Anderson & Horne, 2008; Oginska & Pokorski, 2006).
As mentioned, little work has been done to link subjective sleep need with physiological sleep need. In the current study, we found that subjective sleep need was positively correlated with the objective amount of sleep participants obtained during the weekends prior to beginning the study. This finding indicates that individuals who report higher sleep need obtain more “catch up” sleep on the weekend in order to make up for low-grade sleep debt of accrued on weekdays when their schedule may be more rigid. This leads us to believe that the measure of subjective sleep need used in the current study is at least partially predictive of physiological sleep need. Nevertheless, we did not find that subjective sleep need was an independent predictor of resistance or vulnerability to sleep loss.
However, we found that subjective resilience and subjective sleep need interacted to predict performance following both sleep deprivation and recovery sleep—a finding that suggests the possibility that measures of subjective resilience and subjective sleep may prove useful for (1) screening individuals who are resistant to sleep deprivation and (2) identifying individuals who recover from sleep deprivation relatively quickly. Interestingly, we found that in individuals with normal and high levels of subjective resilience, there was no significant relationship between subjective sleep need and PVT performance. This suggests the possibility that moderate and high subjective resilience masks negative (or positive) outcomes linked to sleep need. As mentioned, others have similarly shown that high levels of resilience obscures negative psychological effects under conditions of poor sleep (Hughes et al., 2018). The present study extends these findings to the realm of neurocognitive performance and suggests that high resilience buffers cognitive performance against the effects of sleep loss, at least in those whose sleep need is low.
There are several theoretical implications for this study. Interestingly, to date, empirical studies have only shown sleep loss results in reduced resilience, not vice versa. For example, we have shown that insomnia symptoms predict several deleterious behaviors that could be considered indicators of low resilience (e.g., less likely to complete military service term, lost work days) in a large Soldier population (Seelig et al., 2016). Similar work showed poorer subjective sleep and circadian misalignment negatively impacted team resilience (Shattuck, Matsangas, & Powley, 2015). The current findings suggest that subjective resilience is a trait that, in combination with high sleep need, predicts the effects of sleep loss and recovery sleep. If, as suggested by the present findings (and those of others), resilience impacts response to sleep loss, and response to sleep loss subsequently impacts resilience, there could be a deleterious cycle between these factors. Future work, as suggested most recently by Pedersen et al. (2015), should be undertaken to determine whether, and the extent to which, improving sleep quality (e.g., via hypnotic medications, cognitive behavioral therapy for insomnia) increases resilience, and vice versa.
Furthermore, it was hypothesized that having low sleep need would predict better performance—i.e., that those with low subjective sleep need would be relatively resistant to the effects of sleep loss. However, we found in individuals with low resilience, low sleep need predicted poorer neurobehavioral performance. Our speculation is that individuals who reported a low sleep need may, as a group, tend to underestimate the amount of sleep that they need, and as a result, carry a greater level of sleep debt than those who report needing (and habitually obtain) more sleep. This hypothesis is supported by findings of a previous study that show individuals reporting low sleep need carry a larger sleep debt (Klerman & Dijk, 2005). Theoretically, years (or a lifetime) of shortened sleep—due to a subjective feeling of low sleep need—could have resultant detrimental effects on performance, which were identified here. Adding to this literature, we found individuals with higher subjective sleep need obtained more sleep during the weekends (presumably when they could sleep ad libitum), potentially as a way to “pay off” low-grade sleep debt accrued on weekdays. Individuals with low subjective sleep need may have felt sleep satiated with less sleep, and thus did not eliminate accrued sleep debt during the weekend—even though it was present—thereby beginning the study with more sleep debt than individuals with higher subjective sleep need. Incredibly, this sleep debt may have still been present even after a period of sleep extension. Future work should aim to further explore the construct of subjective sleep need and whether it may motivate individuals to obtain an adequate amount of sleep (or not).
The results of this study should be interpreted in the context of the study limitations. We had a relatively small sample size, which may have limited our ability to detect certain relationships that exist in larger populations (e.g., a direct link between resilience and performance after sleep deprivation). However, the repeated-measures study design allowed us to paint a preliminary picture of the relationship between resilience, subjective sleep need, and performance that future studies should look to replicate and expand in a larger sample. We were also limited in drawing more conclusions about subjective sleep need and performance measures because we used a single item of inquiry to assess subjective sleep need. Had we used multiple items and inquired about subjective sleep need in different contexts, we could have gained greater insight into what subjective sleep need means to these individuals and how it relates to objective sleep and objective performance. Future studies should aim to incorporate multiple items of this nature so the construct of subjective sleep need can be explored to a greater extent.
Conclusion
To date, there have been few subjective measures that predict interindividual differences in the cognitive response to sleep loss. We tested whether subjective resilience and subjective sleep need predicted how individuals performed on a PVT after sleep deprivation and during a recovery period. These tests were performed after a sleep extension period, during which, theoretically, any existent low-grade sleep debt was dissipated. We did not find resilience and subjective sleep need were independent predictors of PVT performance. However, these factors interacted to reveal individuals with low resilience and low subjective sleep need performed the worst during sleep deprivation and during a recovery period. Although this directionality was expected for resilience, it was not expected for subjective sleep need, as we believed individuals who claimed they need more sleep would fare worse after sleep loss because they would be at a greater sleep deficit. Based on these results, we surmise individuals with low subjective sleep need may habitually obtain less sleep and therefore may have entered the study with more sleep debt that could not be dissipated by sleep extension. Overall, these items could be used to create a screener to detect individuals who may not perform well cognitively under conditions of sleep loss.
Footnotes
Author’s note
Lillian Skeiky is now affiliated with Sleep and Performance Research Center, and Elson S. Floyd College of Medicine, Washington State University, Spokane, WA, United States.
Acknowledgements
This manuscript was written while J. M. and G. S. held a National Research Council fellowship from the National Academies of Science, Engineering, and Medicine. Material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the author and are not to be construed as official or as reflecting true views of the Department of the Army or the Department of Defense. The investigators have adhered to the policies for the protection of human subjects as prescribed in AR 70–25.