
Abstract
There is considerable need to identify effective service provision models to support adults on the autism spectrum as they seek to lead independent lives. This study outlines an individualized life skills coaching program for adults with autism, “LifeMAP”, and the experiences and perspectives of the coaches. Responses on a tailored questionnaire provided detailed insight into how the coaches were performing their job, the strategies they utilized, reasons for client success and difficulty, challenges faced by the coaches, and ways they were supported by program staff. Coaches’ job self-efficacy and satisfaction were also examined. This study serves as a preliminary examination of individualized coaching for adults with autism from the coaches’ perspective.
Introduction
Autism spectrum disorder (ASD) currently affects 1 in 54 children in the United States (Maenner et al., 2020). As a spectrum disorder symptoms and strengths can vary widely with the specific needs of each individual dependent on the degree of impairment, co-occurring conditions (Hollander et al., 2011), and chronological age and developmental stage of the individual. Often thought of in the context of childhood, much attention and energy has been directed at developing empirically supported interventions for children with autism, such as Applied Behavior Analysis (ABA) and TEAACH (Koegel et al., 2009). Considerably less research has focused on how to best serve adolescents and adults (Shattuck et al., 2012), and gaps in transition-related service provision create barriers to access and confusion among family members trying to make sense of different options and varying eligibility criteria (Shogren & Wittenburg, 2020). Accordingly, it is vitally important to consider comprehensive intervention approaches which address a broad range of needs autistic adults may face as they transition to and navigate adulthood.
This manuscript overviews a program which aims to serve the needs of autistic adults: the Life Management Assistance Program (LifeMAP). This program uses one-on-one life skills coaching to help clients achieve a wide variety of goals, from finding employment to living independently. Given the centrality of the coaches to the program model, gaining further insight into strategies they implement in working with clients, and their experiences is important. This work is also timely as the field considers best practices for this population.
Adults with autism
Like their peers without autism, many individuals with autism have post-secondary educational and vocational aspirations and desire to live independently. However, common symptoms of autism can present major obstacles in adult life and outcomes in adulthood have been shown to be relatively poor compared to other populations (Edelson et al., 2020; Shattuck et al., 2012). Poor social, self-advocacy and executive functioning skills can increase the demands associated with major life transitions such as finding and maintaining employment, building meaningful relationships, or living independently from caregivers (Cheak-Zamora et al., 2019; Hillier & Galizzi, 2014; Hillier et al., 2020; Myers et al., 2015).
Using a large national sample of young adults within 6 years of leaving high school, Shattuck et al. (2012) found that only 34.7% had attended college and 55.1% held paid employment. Compared to youth with a speech language impairment, learning disability, or intellectual disability, youth with autism had a lower rate of employment. Autistic adults attended college at a lower rate than those with SLI or learning disability, and 50% of the adults who had left high school in the previous two years had no participation in employment or education (Shattuck et al., 2012). It is estimated that roughly 50–75% of adults with autism are unemployed (Howlin & Moss, 2012; Shattuck et al., 2012; Solomon, 2020). Autistic adults have reported feeling inadequately supported in both college and vocational settings (VanBergeijk et al., 2008), as well as difficulty engaging with peers (Mason et al., 2020). Largely due to these and related difficulties, quality of life for autistic adults is generally lower than their neurotypical peers (Beck et al., 2020; Erez & Gal, 2020; Mason et al., 2020).
Increasing independence in adulthood among those with autism would reduce demands on parents and caregivers, many of whom sacrifice work hours and free time to support their child throughout adulthood (Kinnear et al., 2016). With the drop-off in supports following high-school graduation (Taylor & Mailick, 2014), parents are concerned about their child needing continued support to lead successful adult lives (Cribb et al., 2019). Siblings of children with autism share many of the personal and fiscal worries of their parents; as parents age the role of caretaker often falls to siblings who worry about the impact on them, their families, and their careers (Moss et al., 2019). Costs to society are also significant. Buescher et al. (2014) found that the average lifetime cost to support an individual with autism is $2.44 million, while Leigh and Du (2015) forecast the annual cost of medical and productivity costs of autism to be $461 billion by 2025.
Many individuals with autism can accomplish their goals and reach their potential to become independent, actively contributing members of society (Smith, 1995). Supportive services should take a holistic approach and consider communication, social, independent living, and executive functioning skills, as well as needs in psychosocial, educational, and vocational domains. There is also a need to ensure programs in place are using evidence-based practices (Mazzotti et al., 2016), generalize to other settings (Lecheler et al., 2021), are empirically evaluated, and, if effective, disseminated to other organizations (VanBergeijk et al., 2008).
Coaching adults with autism
One potential solution to help meet the needs of those with autism are coaching or mentoring programs. Coaching typically involves a coach meeting with a client to target various goals to improve outcomes for that individual, and has been associated with improved behavioral, social, health-related, motivational, and career outcomes (Eby et al., 2008). These meetings can occur one-on-one or in small groups, through personal meetings, email exchanges, over the phone, or online. Among those on the autism spectrum, mentoring and coaching have most frequently been implemented in high school or college settings. Mitchell and Beresford (2014) interviewed individuals with autism to identify their feelings towards supports they received as they transitioned from high school. To the student, coaching was perceived to be an especially important type of support. “Good” coaches provided a wide array of supports, from emotional to decision-making and goal-reaching, and displayed knowledge of autism and an understanding of each participant’s unique needs and abilities. Mitchell and Beresford (2014) cautioned against parents taking on the role as coach and recommended schools, autism support networks, peers, and/or other virtual networks be considered as more appropriate options. Bradley (2016) reviewed a peer coaching program for students with autism in the UK which indicated improved self-esteem, social satisfaction, and a reduction in bullying. Students reported feeling included in their school community and increasingly saw their peers as being a potential source of support. Other mentoring programs focused on high-schoolers with autism also report positive outcomes (Curtin et al., 2016; Hillier et al., 2019b). Cook et al. (2017) extended these results to higher education where a facilitated mentoring program was implemented for students at Southern Connecticut State University. Following participation, students indicated increased knowledge of social communication concepts and campus offerings, and felt more comfortable registering for future courses (Cook et al., 2017). Other studies examining similar college mentoring programs support these findings (Barnhill, 2016; Hillier et al., 2019a; Lucas & James, 2018; Rando et al., 2016; Thompson et al., 2020).
Based on these findings, several points of interest may apply to coaching outside of education settings. First, the dynamic seems to be more successful when coaches are not individuals with family ties or vested interests, such as parents or guardians (Mitchell & Beresford, 2014). These coaches should provide “support” which is focused on self-actualization rather than doing things for the students (Mitchell & Beresford, 2014). The use of good coaches can lead to a variety of positive outcomes for the coached students, from improved social knowledge (Cook et al., 2017) to an improvement in self-esteem (Bradley, 2016).
Coaching strategies and perspectives
Both the coach-client relationship and the techniques used while coaching are important pillars of successful coaching and are largely interconnected. First, developing a bond between coach and client that includes mutuality and trust is critical for an effective coaching relationship (Rhodes, 2005). The role of the coach is dependent on the specific needs of the client, and that flexibility is at the core of the coaching relationship (Daughtry et al., 2009). In order to help clients achieve autonomy, the coach provides guidance, expectations, emotional support, access to community resources, and support (Britner et al., 2006). Coaching benefits not only clients, but coaches as well (Hillier et al., 2018), with feelings of accomplishment and personal improvement such as increased patience, a sense of effectiveness, and acquiring new skills or knowledge as potential benefits for coaches (Sword & Hill, 2002). Coach job satisfaction and self-efficacy are crucial for a successful coaching program. Coaches should feel supported and receive periodic training, as well as opportunities to communicate with program managers regarding their progress or challenges faced throughout the coaching process (Sword & Hill, 2002).
LifeMAP program model
This study focused on coaches who participated in a life-skills coaching program run by the Asperger/Autism Network (AANE, n.d.) based in Watertown, Massachusetts. AANE was one of the first ASD-focused organizations in the United States and was founded by parents and practitioners in 1996. The organization seeks to help individuals with autism and related conditions build meaningful and connected lives by providing information, education, community, support, and advocacy in a respectful manner (www.aane.org). Recognizing a need for life skills coaching, AANE developed LifeMAP in 2008 and has since served around 2,600 adults. This program provides practical assistance through “intensive, highly individualized coaching by professionals with expertise in both ASD and specific content areas” (www.aane.org). The program has a staff of three full-time employees, six part-time employees, around 50–60 coaches, and an annual budget of $1 M in revenue.
The Program Director has a Masters’ degree in Community Social Psychology and established and subsequently led the LifeMAP program since its inception. Program staff include a Coach Supervisor who has a background in speech pathology and is the first point of contact for coaches when questions arise. Other staff include an Operations Manager who has a background in business, a Clinical Supervisor and a Clinician with backgrounds in social work, a Program Accountant with a background in accountancy, a Director of Partnerships with a background in law, an Administrative Assistant, and a Data Specialist.
LifeMAP processes an average of 250 new intakes each year with around 350–380 active clients at any given time. Around 80% of LifeMAP clients identify as white with the next largest group identifying as Hispanic (4%). 75% of clients identify as male, with an average age of 26 years (range 15–69 years). Potential clients complete an application process prior to enrollment in LifeMAP and provide demographic, college, and employment history. Some also provide neuropsychological reports but it is not required for enrollment. Exclusion criteria include: 1) refusing to attend the intake interview; 2) during the intake interview client is unable to converse about their goals for coaching; 3) client is known to have intellectual disability (IQ < 70); 4) client has experienced a recent psychiatric hospitalization and currently has no mental health supports in place; 5) client is currently in prison; 6) client has homicidal thoughts. Other factors clients might present with which require further discussion between the Program Director, the Coach Supervisor and the Clinical Supervisor include: 1) client has been convicted of a criminal offense; 2) client has been convicted of a predatory sex offense; 3) client has a history of stalking; 4) client has a substance abuse disorder.
The coaches themselves come from a variety of backgrounds and areas of expertise including personal experience such as having a family member on the autism spectrum, academic expertise in the field of autism research or treatment, individuals with coaching experience, and professionals from a variety of therapeutic backgrounds. LifeMAP employs a rigorous screening process for coaches, all have a bachelor’s level degree and most (around 90%) have a master’s-level degree or higher. Coaches receive initial and ongoing training and professional development. Upon recruitment, coaches are given introductory reading about autism spectrum disorder and the LifeMAP program, requiring around 10 hours to complete. They then complete a four hour orientation and initial training session where the program model is described in more detail, their role is outlined, initial strategies for coaching are discussed, the online database and data collection methodology are explained, and background information on their client(s) is provided, including education and employment history, demographic information, and any neuropsychological or similar reports available. While this training is done individually as coaches are recruited, the content and structure presented to each coach is the same. Coaches then meet with the “Coach Supervisor” on a weekly basis to check in and receive additional supports and guidance. This schedule progresses to a biweekly, then bi-monthly as the new coach progresses. In addition, coaches have a monthly online “clinical hour” where they meet with other coaches and the LifeMAP clinical staff to share resources, exchange ideas and advice for any challenging situations. Professional development continues with their complementary membership to the Asperger/Autism Professional Coaching Association (AAPCA) whose members include experts in the field, coaches working with other organizations, and previous LifeMAP coaches. The AAPCA meets on a monthly basis and provides educational/enrichment opportunities, community and peer support, as well as confidence building and validation for their coaching work. Finally, coaches are able to attend a wide range of frequent workshops and conferences hosted by AANE at no cost.
Coaches are matched with clients based on location and scheduling, as well as areas of need for the client and strengths of particular coaches. These assignments fluctuate as clients enter and leave the program and coaches typically have from one to four clients at a given time. These coach-client pairs meet on a regular basis, typically once a week for an hour. LifeMAP does not provide a standard “curriculum” because each client’s experience is totally unique and tailored to them. However, in all cases, coaches aim to guide clients through the process of identifying concrete, measurable, and achievable goals and then reaching them. They also hope to increase self-confidence in their clients and reduce anxiety around achieving goals.
The goal of this exploratory study was to examine the strategies and approaches coaches utilized when supporting an adult with autism in reaching their goals. The coaches’ experiences, perspectives, job satisfaction and job self-efficacy were also examined to further understand the components of the LifeMAP program.
The specific aims for the study were as follows: To understand the strategies coaches use in their work with adults on the autism spectrum. For example, how do coaches work with clients to help them reach their goals? Are there consistent strategies utilized by coaches? How do they consider their clients’ success? To examine the experiences of coaches in relation to their job and the LifeMAP program itself. What challenges do they face in their role as coach? How does involvement from parents/family members impact their work? Do they feel supported by the LifeMAP team? What is their level of job satisfaction and self-efficacy?
Method
Participants
This study included 24 participants (all female) who were employed as life skills coaches in the LifeMAP program. Their ages ranged from 25 years to 71 years with an average age of 38 years. Twenty-three identified as European-American or White and one identified as Asian. Coaches came from a variety of vocational backgrounds, but all had been screened and hired to work with adults with autism based on some area of expertise or experience. Areas of expertise ranged from personal experience (such as having a family member with autism), to academic expertise in the field of autism research or treatment, to individuals with coaching experience, to professionals from a variety of therapeutic backgrounds.
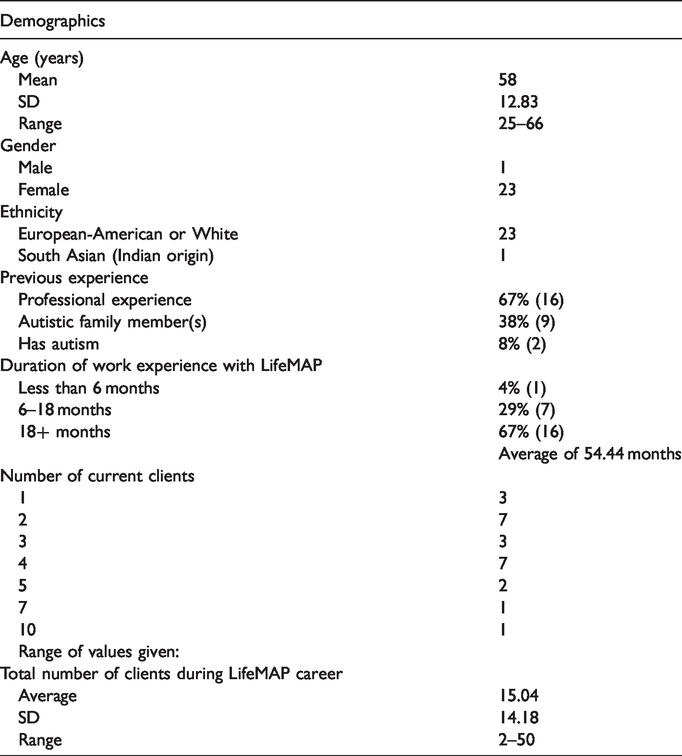
One coach had been in the program for less than 6 months, seven for 6–18 months, and the remainder (16) for over 18 months, with the most veteran having coached for 11 years. The majority worked with between two to four clients at a time and over their tenure with LifeMAP had worked with anywhere from two to 50 clients. Thanks to this heterogeneity in experience, tenure, and number of clients, there was a range of differing experiences whilst working for the program, and the sample was considered to be representative of the larger pool of LifeMAP coaches (see Table 1).
Coaches demographic and background information.
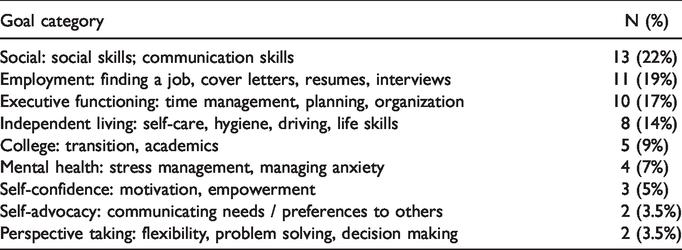
Coaches mostly met with clients in the community such as at a library or coffee shop (n = 21) and/or at their clients’ home (n = 13), but some reported meeting at school (n = 3), at AANE (n = 3), via Skype (n = 4), or other locations (n = 2). These locations sometimes varied whilst working with a client and coaches could report multiple meeting locations. Coaches reported mostly working on one or two goals at a time. Table 2 shows the goals coaches reported working on with clients.
Number of goals reported by coaches in each category.
Procedures
An email invitation was sent out to 55 LifeMAP coaches and included a link to the questionnaires using Qualtrics software (Qualtrics, Provo, UT). Twenty-four coaches responded to the invitation resulting in a 44% response rate. Following the informed consent statement where participants indicated consent by checking a box, participants completed three measures: The “LifeMap Coach Questionnaire” which was prepared by the authors and tailored to the LifeMap program, and two standardized questionnaires: the Occupational Self-Efficacy Scale – short version (Rigotti et al., 2008) and the Minnesota Satisfaction Questionnaire (Weiss et al., 1967).
The “LifeMap Coach Questionnaire” consisted of rating scale questions and open-ended questions with 13 questions in total. Eight questions examined how coaches structure a typical coaching session, strategies and approaches that seem to work best, and how they consider their clients’ success. An additional five questions examined the challenges coaches faced in their role, the training they received, and whether they felt supported by the LifeMAP team. Questions and responses can be seen in Tables 3 and 4.
Coaching strategies.
Experiences of coaches.
The two standardized measures focused on specific aim two and examined levels of job satisfaction and self-efficacy: The Minnesota Satisfaction Questionnaire (Weiss et al., 1967) assessed the coaches’ job satisfaction. Coaches answered 20 questions about what aspects about their work they were satisfied with and things they were not satisfied with in response to the prompt “On my present job, this is how I feel about:” with responses including “Being able to keep busy all the time,” “The chance to work alone on the job,” and “The chance to do different things from time to time.” Responses were on a five-point scale from “very dissatisfied” (score 1) to “very satisfied” (score 5). This measure has good psychometric properties with reliability coefficients varying from .87 to .92 on the General Satisfaction scale (Weiss et al., 1967). Construct validity is supported by studies indicating significant differences on the scale between individuals from different occupational groups (F(6, 1716 = 38.01; p = .001), where electronic assemblers had the lowest and salesmen the highest mean satisfaction score.
The Occupational Self-Efficacy Scale – short version (Rigotti et al., 2008) included six items. Questions took the form of “I” statements, which participants rated on accuracy when considering themselves. Sample questions included “I can remain calm when facing difficulties in my job because I can rely on my abilities”, and “When I am confronted with a problem in my job, I can usually find several solutions.” Responses were on a 6-point scale from “not at all true” (score 1) to “completely true” (score 6). The scale has satisfactory psychometric properties with reliability coefficients of .85 and .90 and good internal consistency with item–total correlations greater than .50 for all items (Rigotti et al., 2008). In evaluating construct validity Rigotti et al. (2008) compared responses on the scale to measures of four other variables: job satisfaction, job insecurity, commitment and performance across participants from five countries (Germany, Sweden, Belgium, UK, and Spain). Correlations between responses on the Occupational Self-Efficacy Scale were significant with all four variables for all participant groups except the UK sample where significant correlations were not found for commitment or job insecurity. Overall, construct validity was deemed as satisfactory.
Data analysis
LifeMAP coach questionnaire
Quantitative data from the LifeMAP Coach Questionnaire was summarized and averaged, and coding categories were developed for the qualitative data from the open-ended responses. This began with examination of verbatim responses to the open-ended questions. The responses were repeatedly reviewed in their entirety by two authors (blinded for review) to achieve immersion and obtain a sense of the whole (Tesch, 1990). Next, specific words, sentences, and portions of the text that appeared to capture key concepts and thoughts were highlighted using a Directed Content Analysis (Hsieh & Shannon, 2005; Morgan, 1993). The coders made notes on their impressions and initial analysis, and as this process continued, labels for codes emerged from the text and were sorted into coding categories. Depending upon the content of a coach’s reply, a single answer could be coded into multiple categories. Once the categories had been agreed upon, the first coder (initials blinded) independently coded the open-ended responses. A randomly selected sample of seven questionnaires (25%) were then coded by the second coder (initials blinded) to ensure consistency in coding. Inter-rater reliability for coding was achieved with 91% agreement.
Job satisfaction and self-efficacy
The Minnesota Satisfaction Questionnaire (Weiss et al.,1967) and the Occupational Self-Efficacy Scale – short version (Rigotti et al., 2008) were both examined by summing items for a total score and calculating the average.
Results
Coaching strategies
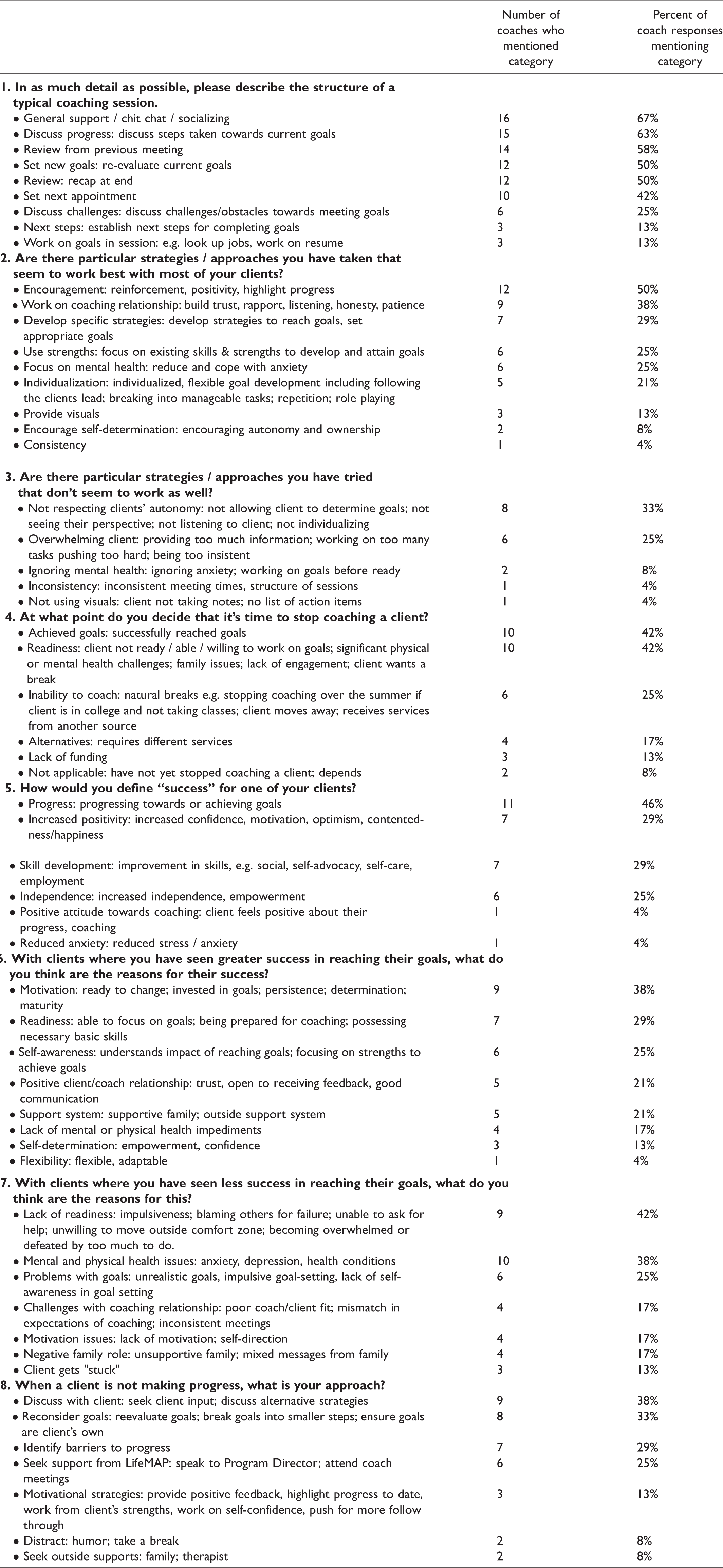
To examine the strategies coaches used in their work, how they worked with clients to help them reach their goals, and how they considered their clients’ success, the open-ended data was coded to the identified categories. Table 3 shows how many coaches’ responses were coded to each category (where some responses mentioned more than one category), and the percentage of responses coded to each category.
Table 3 outlines the strategies coaches used in their work with adults on the autism spectrum. During sessions, coaches most commonly included chit chat and socializing (n = 16 coaches), discussing progress towards goals (n = 15), review from the previous meeting (n = 14), setting new goals and reevaluating current goals (n = 12), and review and recap at the end of the session (n = 12). Only three coaches reported directly assisting clients in performing goals during the meetings. Coaches utilized a variety of strategies most commonly including encouragement, reinforcement, positivity and highlighting progress (n = 12). Coaches also mentioned working on their relationship with the client (n = 9), developing specific strategies to reach goals (n = 7), focusing on mental health (n = 6), and utilizing strengths (n = 6). Ineffective strategies included not respecting the client’s autonomy (n = 8) and overwhelming the client (n = 6).
Mostly coaches decided to stop coaching a client either when they had reached their goals or when it became apparent that the client was not ready/willing/able to work on their goals. Success was primarily defined by coaches as progress towards goals, improvement in skills, increased positivity, and increased independence. Coaches identified reasons for success including client motivation, readiness, self-awareness among other factors. Primary reasons identified for clients who experienced less success in reaching goals were mental and physical health issues, lack of readiness, and problems with goals such as unrealistic goals. When clients were not making progress coaches typically addressed this directly with the client, reconsidered the goals, identified the barriers to making progress, and reached out to LifeMAP staff for support.
Experiences of coaches
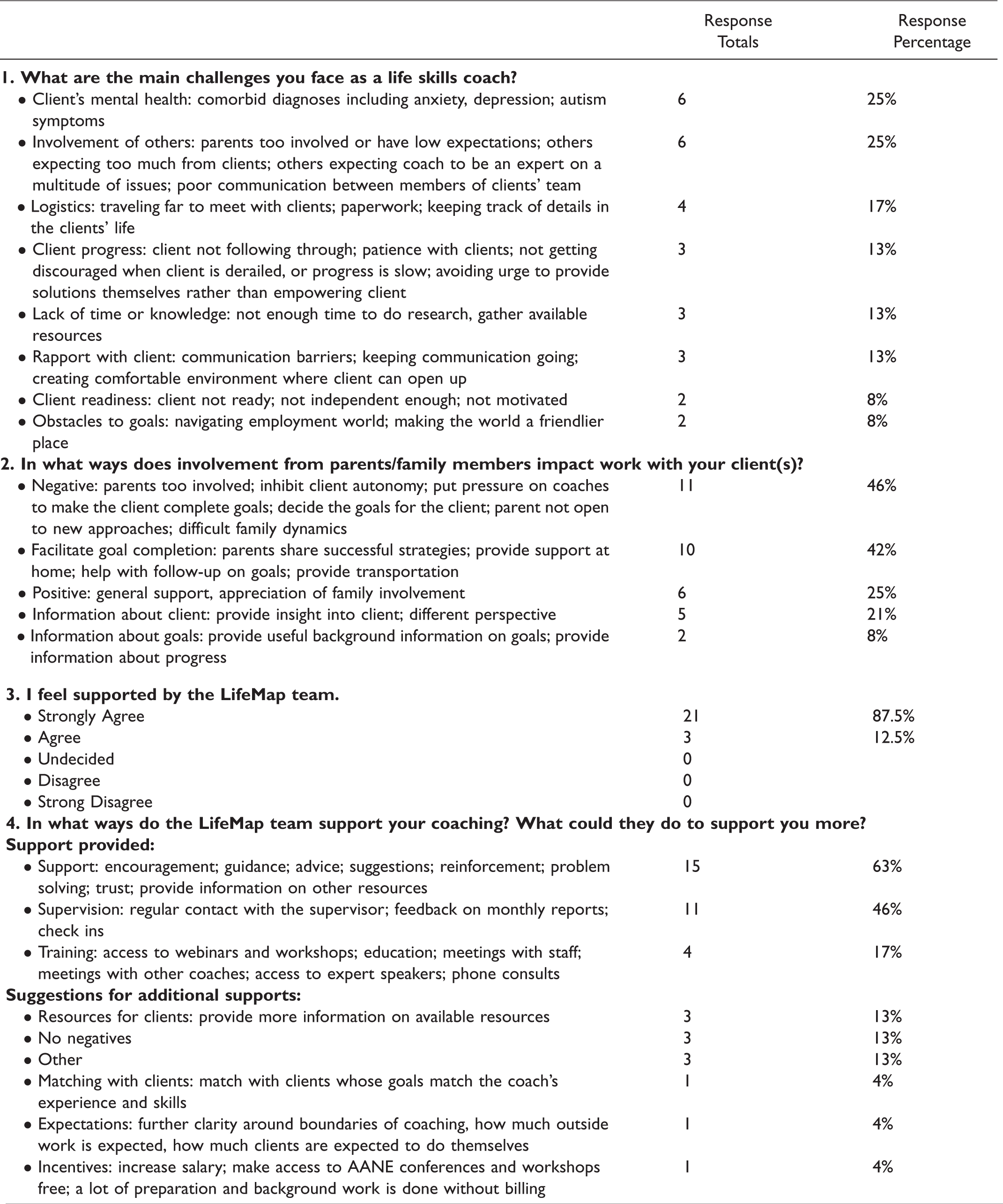
To examine the experiences of coaches in relation to their job and the LifeMAP program itself, the open-ended data was again coded to the identified categories. Table 4 shows how many coaches’ responses were coded to each category (where some responses were coded to more than one category), and the percentage of total responses coded to each category.
Coaches identified a number of challenges inherent to their role with the most common responses relating to the client’s mental health, the involvement of others, and logistics such as traveling to meet with clients, paperwork and keeping track of details in the client’s life. Coaches identified some negative aspects of parent/family member involvement such as being too involved, inhibiting client autonomy, and putting pressure on coaches to make the client complete goals. However, they also reported that parents/family members facilitated goal completion, shared successful strategies, and provided support and follow-up at home. All coaches agreed or strongly agreed that they felt supported by LifeMAP and cited supervision, training, and various other support strategies. They also provided some suggestions for additional supports such as providing coaches with more information on resources available to clients.
Job satisfaction and self-efficacy
To examine coaches’ reported levels of job satisfaction we utilized the Minnesota Satisfaction Questionnaire (Weiss et al., 1967). Responses were given on a 5-point scale with higher scores indicating greater satisfaction). Total scores averaged 83 out of 100 possible points (SD = 7) and ranged from 70–95 indicating a high level of job satisfaction.
To examine coaches’ reported levels of job self-efficacy we utilized the Occupational Self-Efficacy Scale – short version (Rigotti et al., 2008). Responses were on a 6-point scale with higher scores indicating higher occupational self-efficacy. Total scores averaged 31 out of 36 possible points (SD = 3) and ranged from 20–36 indicating a high level of job self-efficacy
Discussion
Given the critical need to find effective strategies to support autistic individuals in adulthood we explored a life-skills coaching program, and in particular, examined how coaches conducted their sessions, and the strategies they utilized when supporting an autistic adult working towards their goals. The study is unique in its focus on the autistic adult population and life skills coaching focused on a broad range of goals. The findings indicated apparent consistency in how coaches implemented their sessions with the bulk of time spent discussing progress towards goals, setting new goals and reevaluating current goals, rather than directly working together with clients on the goals. Key strategies coaches utilized included individualized, flexible goal setting, establishing rapport based on individualized needs, respecting their client’s autonomy, targeting specific skill gaps, focusing on mental health, and providing positive feedback and praise. These findings mirror those identified in previous research with other populations, in particular establishing a collaborative and mutual relationship based on trust, respect and care (Daughtry et al., 2009; Rhodes, 2005), and further consolidate ideas for best practices when working with this and related populations.
Those clients who achieved greater success were those reported by coaches as more motivated, ready to make changes, and more self-aware. Clients who experienced less success were those reported as having poorer mental or physical health, those with unrealistic goals, and those who were not ready to work on goals independently. Difficulties with awareness, theory of mind, and executive functioning are common among those with autism (Demetriou et al., 2019; Velikonja et al., 2019), and without specifically measuring these skills, the accuracy of the coach’s perspectives on what resulted in more or less success may be biased and/or correlated with clients’ cognitive ability. For future work it would be helpful if more information on clients’ abilities and functioning levels were available. When LifeMAP clients were not experiencing success, coaches engaged in a number of strategies including directly addressing the client, seeking outside supports, assessing other barriers to goals, and re-evaluating goals.
At the core of the program was the coaches’ ability to provide a truly individualized approach to their work with each client. While there was consistency in how sessions were conducted, there was considerable diversity in strategies used to support success and to address problems in making progress. This diversity suggests that coaches were skilled in their ability to tailor their ideas and approaches to each individual client based on their specific goals as well as their strengths and challenges. Behavioral intervention research has demonstrated the effectiveness of one-on-one approaches with children with autism and tailoring a program to meet the individual needs of each child (Yu et al., 2020). These components may be critical ingredients in work with adults as well.
Across multiple questions coaches emphasized their client’s active role in the coaching process and the importance of respecting their autonomy. Coaches also indicated that failure to achieve goals, and failure with the overall coaching process, came from not respecting the clients’ autonomy and limits, and failure to respect client independence. Only three coaches described directly helping a client complete a goal (such as serving as a daily accountability partner via text) during or outside the sessions, while none described taking charge or becoming the driving force behind goal completion. It was key that clients either independently or in close collaboration with the coaches defined their own goals and worked closely with the coach to achieve progress towards those goals. Attempting to prescribe goals on behalf of clients, utilize strategies the client was not ready for or which were not a good match for them, or in any other way insist the client did things the way the coach or parents felt best, was reported as unsuccessful. Therefore, the person-centered focus of the program was an underlying philosophy adopted across coaches and may be important to positive client outcomes. Person-centered approaches are central to current service provision models for individuals with disabilities (Friedman, 2019), and respecting the client’s agency is indicative of optimal outcomes for most types of therapy and services. Previous mentoring research highlights the importance of encouraging and facilitating autonomy among clients, such that the coach should provide guidance, expectations, emotional support, access to community resources, and positive reinforcement for their clients as they work towards independence (Britner et al., 2006).
Our findings extend the existing work on coaching with autistic adults which has largely focused on mentoring programs in school and university settings (e.g. Bradley, 2016; Hillier et al., 2019a, 2019b; Thompson et al., 2020). Our findings are similar to this previous work with regards to the positive outcomes found with one-on-one supports, but LifeMAP implements a very different approach. Programs focused on high school transition and/or higher education are often short-term and designed to specifically address employment or education related challenges and goals, whereas the LifeMAP program is focused on a broad range of goals and is unlimited in length of time coaching may continue. LifeMAP is also on a much larger scale than has been previously reported in the literature both with regards to number of clients served, coaches and supervisors involved, and resources and supports provided to coaches.
The coaches’ experiences, perspectives, job satisfaction and job self-efficacy were also examined to further understand the components of the LifeMAP program. Coaches reported several challenges in their work including client mental health where comorbid diagnoses such as anxiety and depression presented significant barriers to client progress towards goals. Previous research has established that autistic adults are more likely to receive a diagnosis of anxiety or depression than their neurotypical peers (e.g. Kirsch et al., 2020). Coaches identified addressing mental health barriers and improving confidence as priorities and pre-requisites before progress towards other goals could be realized.
Coaches described navigating the coaching process with parents who often served as important allies in providing additional follow-up and supports at home which facilitated goal completion, as well as background on the client and previously successful strategies. Challenges arose when parents were too involved, had unrealistic expectations, applied undue pressure on the coach to make the client complete goals, inhibited client autonomy, or were not open to new approaches. This highlights the necessity of clear communication between members of the clients’ team, another challenge coaches reported. Other challenges included logistics, lack of time or knowledge, establishing rapport with the client, and handling lack of client progress. Coaching draws on a considerable skill set including effective communication, relationship building, realistic goal setting, patience, empathy, how to empower a client to develop and reach their own goals, and an overall understanding of what supports the client needs from them. Others considering implementing a similar program must appreciate how recruiting the right coaches is central to program success and is an art in itself which takes considerable experience.
Coaches felt very positive about the support they received from the LifeMAP program, with over 50% describing strong positive feelings of support from other coaches and LifeMAP staff. Particularly well-noted were “brainstorming” communiques with supervisors about how to approach a client, as well as discussion during meetings between coaches. Training and ongoing supervision of coaches is reflective of best practices in the existing literature (Rhodes, 2005). Coaches also reported high job satisfaction and occupational self-efficacy, which are extremely important for retention of skilled coaches. The feedback coaches provided about how LifeMAP could further support them might be useful to others providing similar services and included providing more information on available resources clients could access, and compensation for the preparation and background work that is done without billing.
Limitations and future directions
We hoped to examine how coaches implemented their sessions, the strategies they utilized when supporting an adult with autism in reaching their goals, and their experiences in their role. The richness of results provided by our qualitative data helped meet this aim. However, there was a wide range of response content and length. Future research could consider a more active role in shaping responses, such as through a minimum word count. While beyond the scope of this study, data pertaining to client success in reaching goals and qualitative data on client perspectives, would be an important next step for future work and is currently underway. Additional background information on clients such as measures of cognitive functioning would also be helpful in further understanding what factors ultimately contributed to success in reaching goals. Specific information on the educational and vocational background of coaches would also be important to gather in future work. Finally, relying on coaches to volunteer to participate rather than being able to randomly select coaches may have resulted in bias. It is possible that coaches who feel positively towards the LifeMAP program or those who had been with the program for longer, were more likely to choose to participate, and more likely to have higher job satisfaction and self-efficacy than those choosing not to participate.
Despite these limitations, our findings provide valuable information about community coaches and preliminary data on implementation factors that is helpful for other researchers and clinicians. Our findings also build on the current literature which almost exclusively focuses on education settings. The LifeMAP model is timely as new ways to access funding for services become available, such as health insurance. Coaching can also be provided virtually, a need which seems likely to continue to grow.
Identifying successful strategies and common obstacles for coaches yielded a list of skills and areas which could shape future trainings for coaches in similar programs. Information on how to conduct sessions, core strategies for success, and what to do if a client is not making progress shared by our sample provides a window into what effective coaching might look like. Based on the coaches’ reports, individualized approaches are key to successful service provision for autistic adults.
Footnotes
Authors’ note
We have chosen to use person-first language “those with autism” and identity-first language “autistic” interchangeably to reflect the preferences of multiple stakeholders.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LifeMAP receives funding from the Massachusetts Department of Developmental Services.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.