
Abstract
The purpose of this research was to benchmark the importance and use of labor market survey (LMS) among U.S. certified rehabilitation counselors (CRCs). A secondary post hoc analysis of data collected via the Rehabilitation Skills Inventory–Revised for the 2011 Commission on Rehabilitation Counselor Certification job analysis resulted in importance and use ratings across 11 content items and 11 demographic variables. This research suggests that labor market analyses, of which LMS could be a component, were considered to be along a continuum of important or extremely important by CRCs and performed along a range of very infrequent to very frequent. Data suggest that those CRCs reporting the highest frequency of use of labor market analyses were older and male, possessed education in rehabilitation-orientated areas of study, had more than 20 years of post-CRC experience, were in the private/proprietary rehabilitation or private practice practitioner professional settings, and held the title of forensic/expert witness or rehabilitation consultant/specialist. For all survey items studied, employment setting and job title were found to be significant in the frequency of use of labor market analyses. Limitations, delimitations, and areas for further study were discussed.
Keywords
Labor market survey (LMS) as used in rehabilitation and disability services has been defined as “a survey methods strategy to collect qualitative and/or quantitative data for a small population census or sample about an identified labor market in order to draw inferences to the client/evaluee (N = 1)” (Barros-Bailey, 2011, in press). There are generally three phases in the rehabilitation counseling process where LMS is used—vocational exploration, plan development, and job placement. In vocational exploration and plan development, inferences from LMSs might be distal from the client and involve examining a variety of potential occupations and their relevant labor market factors important to establishing a vocational goal and developing a rehabilitation plan and justification. In this instance, the inference is how the occupation(s) or job classification meet(s) an assessment of the needs, skills, and/or interests of the individual. The intended outcome at these phases is typically a plan. For the job placement phase, the LMS information may be used more for establishing relationships with employers or identifying job opportunities within the labor market. For this phase, the immediate inference is very proximal to the client; that is, the information is used in the direct match between the abilities of a single individual and the work activities, requirements, and demands of a single or small pool of available positions. The intended outcome at this phase is placement and integration of an individual with a disability into the world of work. It has been established by Neulicht, Gann, Berg, and Taylor (2007) and confirmed by Barros-Bailey (2011, in press) that there exists little in the literature on the use and practice of LMS in rehabilitation and disability services; thus, LMS may arguably depict a professional area of rehabilitation counseling that is mainly carried forth by oral tradition in education, training, and practice.
Use of Labor Market and Occupational Information in Rehabilitation Counseling: Historical Perspective
Wright, Leahy, and Shapson (1987) first documented the use of labor market and occupational data as an essential competency in the role and function of rehabilitation counselors. Over the last 25 years, this minimal competency was confirmed in follow-up job analyses reported by Leahy, Chan, and Saunders (2003) and Leahy, Muenzen, Saunders, and Strauser (2008). The occupational and labor market information competency’s importance and use to certified rehabilitation counselors (CRCs) is a broad term that could contain a variety of data types, not just LMS. Recently, Neulicht et al. (2007) and Barros-Bailey and Heitzman (2011) documented the broad use of LMS in private and forensic practice and case law across most state and all federal courts. However, there has never been a comprehensive examination among a national sample of rehabilitation counselors in all practice settings and demographics that benchmarks the use of LMS. Given that the competency of methods and techniques of conducting LMS is included in credentialing standards (Commission on Rehabilitation Counselor Certification [CRCC], 2011c), obtaining a broader perspective of its importance and use to assist educators, rehabilitation counselors, and researchers in honing in on those techniques and methods becomes important pedagogically.
Benchmarking is defined by Merriam-Webster as “a point of reference from which measurements may be made” as well as “something that serves as a standard by which others may be measured or judged” (http://www.merriam-webster.com/dictionary/benchmark). Therefore, the purpose of this research is to benchmark the use of LMS among CRCs using the CRCC data from a national sample to serve as a point of reference in rehabilitation counseling. The following research questions were addressed by this study:
Research Question 1: What is the use of LMS by CRCs by demographic variable (age, gender, education, type of disability, geographical location, job title, work experience, area of study, credentials, professional membership, and employment setting)?
Research Question 2: Are there differences in the use of LMS by CRCs between these demographic variables?
CRCC Job Analysis Study: Instrumentation
The CRCC is the largest and only credentialing organization in the world providing certification to more than 16,500 rehabilitation counselors residing in the United States, Canada, and other countries. To maintain its credential as a certifying body by the Institute for Credentialing Excellence, CRCC must perform a professional job analysis—also referred to as a “role and function study”—every 5 years. The results of the job analysis are used not only to establish the competencies needed in rehabilitation counseling, but also by the Council on Rehabilitation Education (CORE) to determine corresponding accreditation standards for graduate education (CORE, 2011).
The most recent job analysis was performed in 2011 (Leahy, Chan, Sung, & Kim, 2011). 1 This LMS benchmarking study consists of a secondary quantitative analysis of the CRCC 2011 job analysis database (Leahy et al., 2011) for items and constructs specific to LMS and related occupational information. This is the first time in CRCC’s existence that a subset of its job analysis raw data has been examined for a specific competency area required in rehabilitation counseling practice by a credentialing body.
The CRCC 2011 job analysis study (Leahy et al., 2011) revised two instruments to collect data about the functions and knowledge requirements of CRCs: the Knowledge Validation Inventory–Revised (KVI-R) instrument (CRCC, 2011b; Leahy et al., 2008; Leahy et al., 2011) and the Rehabilitation Skills Inventory–Revised (RSI-R; CRCC, 2011b; Leahy et al., 2011; Leahy, Shapson, & Wright, 1987; Wright et al., 1987). The RSI-R was “designed to assess the importance of specific job tasks and professional functions in relation to the respondent’s role as a rehabilitation counselor in his or her work setting” (Leahy et al., 2003, p. 69). Because the purpose of this research is to examine LMS’s use as a specific job task and professional function, this benchmarking study examined data collected exclusively by the RSI-R. Leahy et al. (1987) documented the validation of the original RSI and Wright et al. (1987) reported on the results of the first administration of the instrument. The second revision of the RSI was created for the 2001 CRCC job analysis (Leahy et al., 2003). The 2011 job analysis (Leahy et al., 2011) constitutes the third revision of the RSI.
The RSI-R instrument instructs respondents to answer the task and function competency items as follows:
Use the importance scale to indicate the degree of importance of the job function described in the statement to your role as a rehabilitation counselor in the setting in which you work.
Use the frequency scale to indicate the frequency that you perform these tasks taking into account all of the things you do over the course of a year in the setting in which you work.
The instrument is designed with a 5-point Likert-type scale along the following continuum for the corresponding importance and frequency queries, respectively (0 = not important/not at all; 1 = somewhat important/very infrequently; 2 = important/somewhat frequently; 3 = very important/very frequently; and 4 = extremely important/most of the time).
Method
The researchers who performed this study were doctoral-level CRCs who had chaired CRCC, served on or chaired its Exam & Research Committee that oversees the job analysis study, and had cumulatively more than 48 years of experience as practitioners, 20 years in forensic rehabilitation, 20 years in rehabilitation education, 28 years in rehabilitation research, and 26 years performing LMSs and using occupational data in rehabilitation counseling. Both researchers had also been formally involved in analyzing data from past CRCC job analyses and publishing these results for the two studies immediately preceding the 2011 study (Leahy et al., 2011).
Given the combined and complementary rehabilitation counseling experiences of the researchers, each one independently examined the 2011 RSI-R instrument to determine which items should be included in this benchmarking study. Also adopted as a conceptual framework on occupational information and LMS was the Neulicht et al. (2007) Labor Market Search (LMSea) model, as modified by Barros-Bailey (in press). This model consists of two data components: labor market research (LMR) involving secondary data, which is generally more econometric, and LMS containing primary data, which is principally ergometric and ergonometric. As identified in other literature (Barros-Bailey, 2011, in press), LMSea can contain either LMR or LMS, or it can contain both components such that LMSea = LMR (secondary data) ± LMS (primary data). The concept of LMSea is consistent with the definition of labor market analysis (LMA) that has been described as “the measurement and evaluation of economic forces as they relate to the employment process” (State of Massachusetts Labor and Workforce Development, para. 66). That measurement could come from data that are collected by the rehabilitation counselor (thus, LMS) or come from data collected by other public or private entities (thus, LMR). Because the LMSea and LMA terms are synonymous, LMA will be used in this study for consistency with the manner in which it is used in credentialing (CRCC, 2011a) and accreditation (CORE, 2011) publications to constitute the inclusion of primary and secondary data.
The selection criteria for inclusion of survey questions from the RSI-R in the final database were as follows:
Did the item specifically indicate “LMS”?
Did the item fall broadly into the Barros-Bailey (2011, in press) definition of LMS?
Did the item conceptually fall into the Neulicht et al. (2007) LMSea framework for primary and secondary labor market and occupational data (also called LMA)?
Did the item include actions of how LMS and occupational data could be used in practice as consistent with the data’s application in vocational exploration, development, and job placement phases?
Once each researcher arrived at a list of survey items, the results were shared with the other researcher resulting in above 90% concurrence. Of the items that had been selected by one researcher or not another, review of the differences resulted in 100% consensus as to the final 11 RSI-R items across the importance and frequency domains included in this study. An alphabetized list of the selected items and their resulting means and standard deviations per importance and frequency are detailed in Table 1.
CRCC Job Analysis Study: Labor Market Survey Items.
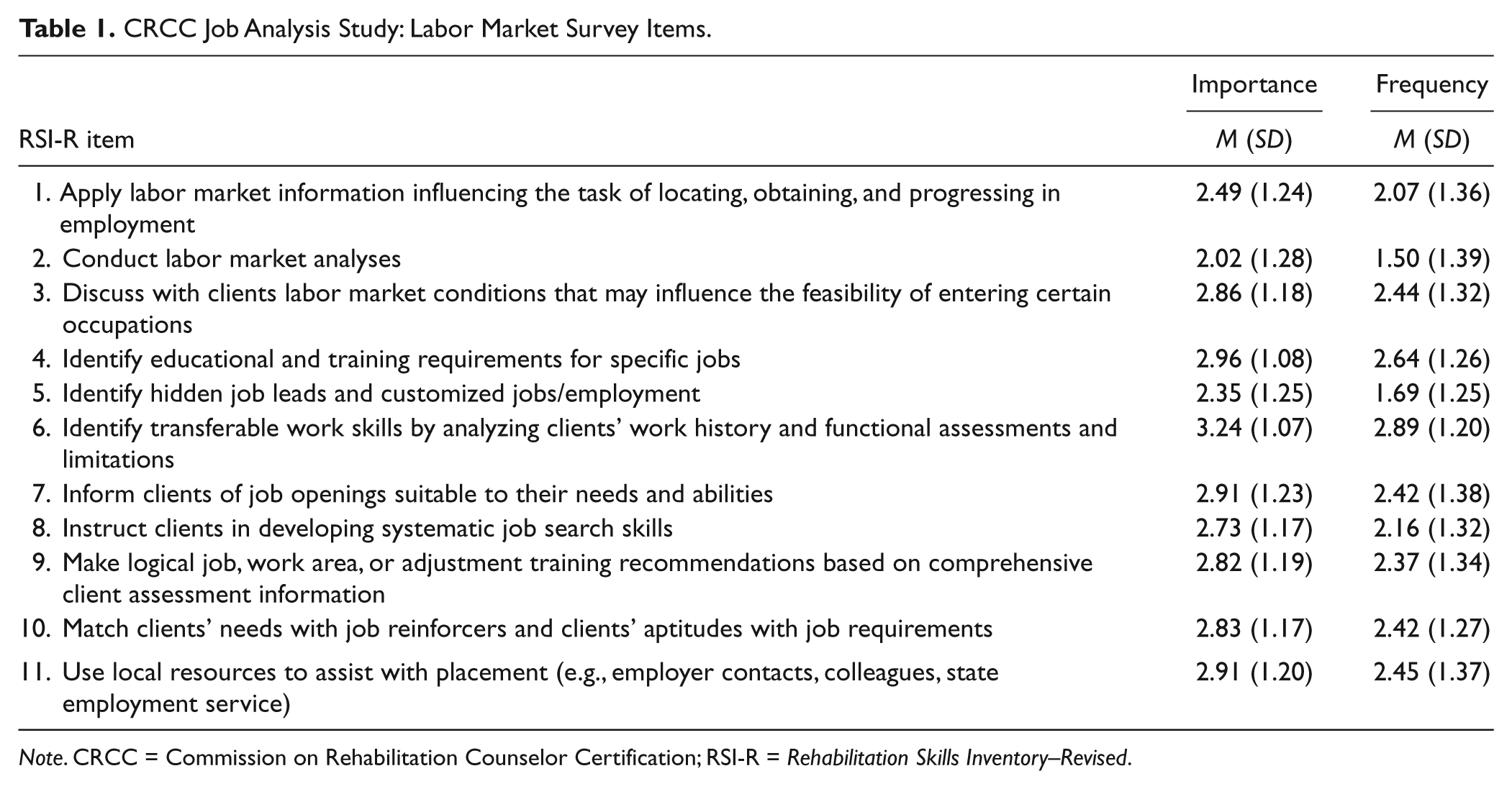
Note. CRCC = Commission on Rehabilitation Counselor Certification; RSI-R = Rehabilitation Skills Inventory–Revised.
None of the 11 survey questions on the RSI-R directly address the importance or frequency of use of LMS by CRCs. However, given the Barros-Bailey (2011, in press) definition of LMS and how the data are inferred to the client at the various stages of the rehabilitation counseling process, three of the survey questions on the 2011 instrument directly relate to the use of labor market data for inference in vocational exploration (3, 4, and 9), five relate to inference as applied in the job placement process (1, 5, 7, 8, and 11), and three questions could apply to vocational exploration or placement (2, 6, and 10).
With respect to the unit of analysis being a person- or work-centered orientation of the labor market and occupational information, the items selected for this study fell along a continuum. Items 1, 3, 6, 7, 8, 9, 10, and 11 resulted in data that were more person centered, or reflecting inference about the abilities of a client. That is, these items were oriented from the perspective of primarily making an assessment of the client’s abilities to match those to the demands of work. Items 2, 4, and 5 were oriented toward the requirements of work and then matching those to the abilities of the individual. By including the universe of RSI-R items, the researchers verified that both data orientations of person-centered abilities and work-centered requirements involving occupational and labor market information were included in this study.
Results
Sample Demographics
Tables 2 and 3 contain the responses to the 11 selected demographic variables from the 2011 RSI-R for the 2011 study sample. Those demographic variables contained in Table 2 are distinct to data collected exclusively with the RSI-R, of which there is no directly comparable demographic data collected for the CRCC population database. Differences in descriptive statistics between this study and those reported by Leahy et al. (2011) are based on how each group of researchers chose to handle missing variables or grouped comments or qualitative responses. For example, the authors chose to include all responses to the RSI-R and to categorize missing data as such while Leahy et al. eliminated two respondents with incomplete responses.
2011 Selected Demographic Variables Responses Distinct to RSI-R.
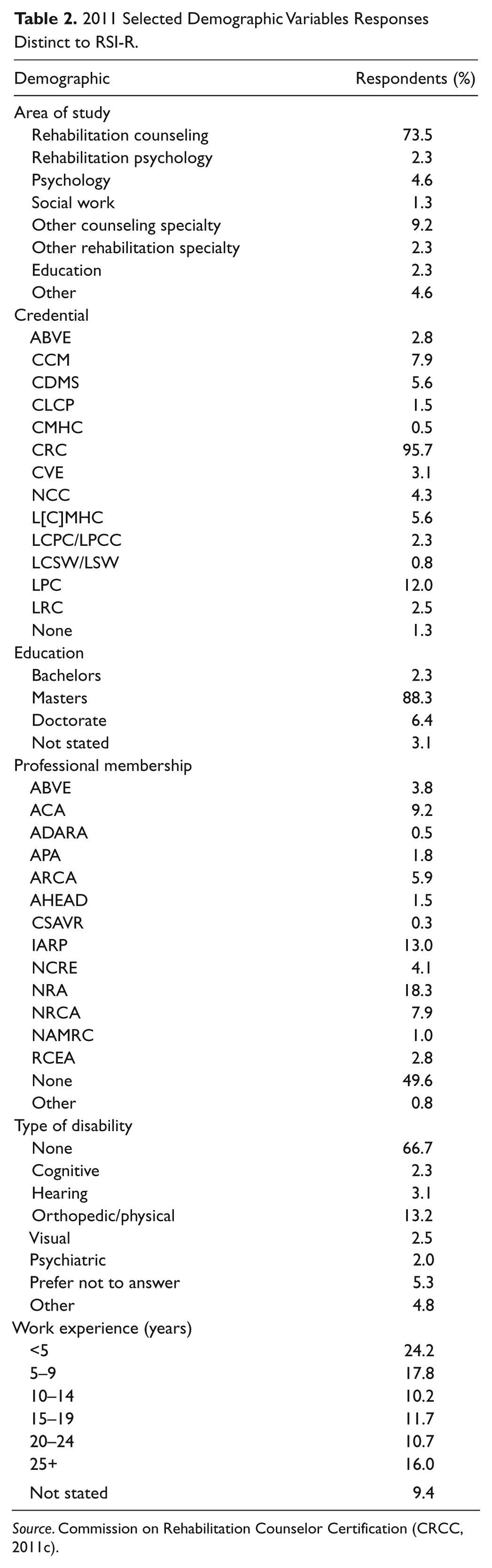
Source. Commission on Rehabilitation Counselor Certification (CRCC, 2011c).
Note. RSI-R = Rehabilitation Skills Inventory–Revised; ABVE = American Board of Vocational Experts Fellow/Diplomate; CCM = Certified Case Manager; CDMS = Certified Disability Management Specialist; CLCP = Certified Life Care Planner; CMHC = Certified Mental Health Counselor; CRC = Certified Rehabilitation Counselor; CVE = Certified Vocational Evaluator Specialist; NCC = National Certified Counselor; L[C]MHC = Licensed Clinical Mental Health Counselor/Licensed Mental Health Counselor; LCPC/LPCC = Licensed Clinical Professional Counselor/Licensed Professional Clinical Counselor; LCSW/LSW = Licensed Clinical Social Worker/Licensed Social Worker; LPC = Licensed Professional Counselor; LRC = Licensed Rehabilitation Counselor; ACA = American Counseling Association; ADARA = Professionals Networking for Excellence in Service Delivery With Individuals Who Are Deaf or Hard of Hearing; APA = American Psychological Association; ARCA = American Rehabilitation Counseling Association; AHEAD = Association of Higher Education and Disability; CSAVR = Council of State Administrators of Vocational Rehabilitation; IARP = International Association of Rehabilitation Professionals; NCRE = National Council on Rehabilitation Education; NRA = National Rehabilitation Association; NRCA = National Rehabilitation Counseling Association; NAMRC = National Association of Multicultural Rehabilitation Concerns; RCEA = Rehabilitation Counselors and Educators Association.
CRCC True Population Versus RSI-R 2011 Demographic Results.
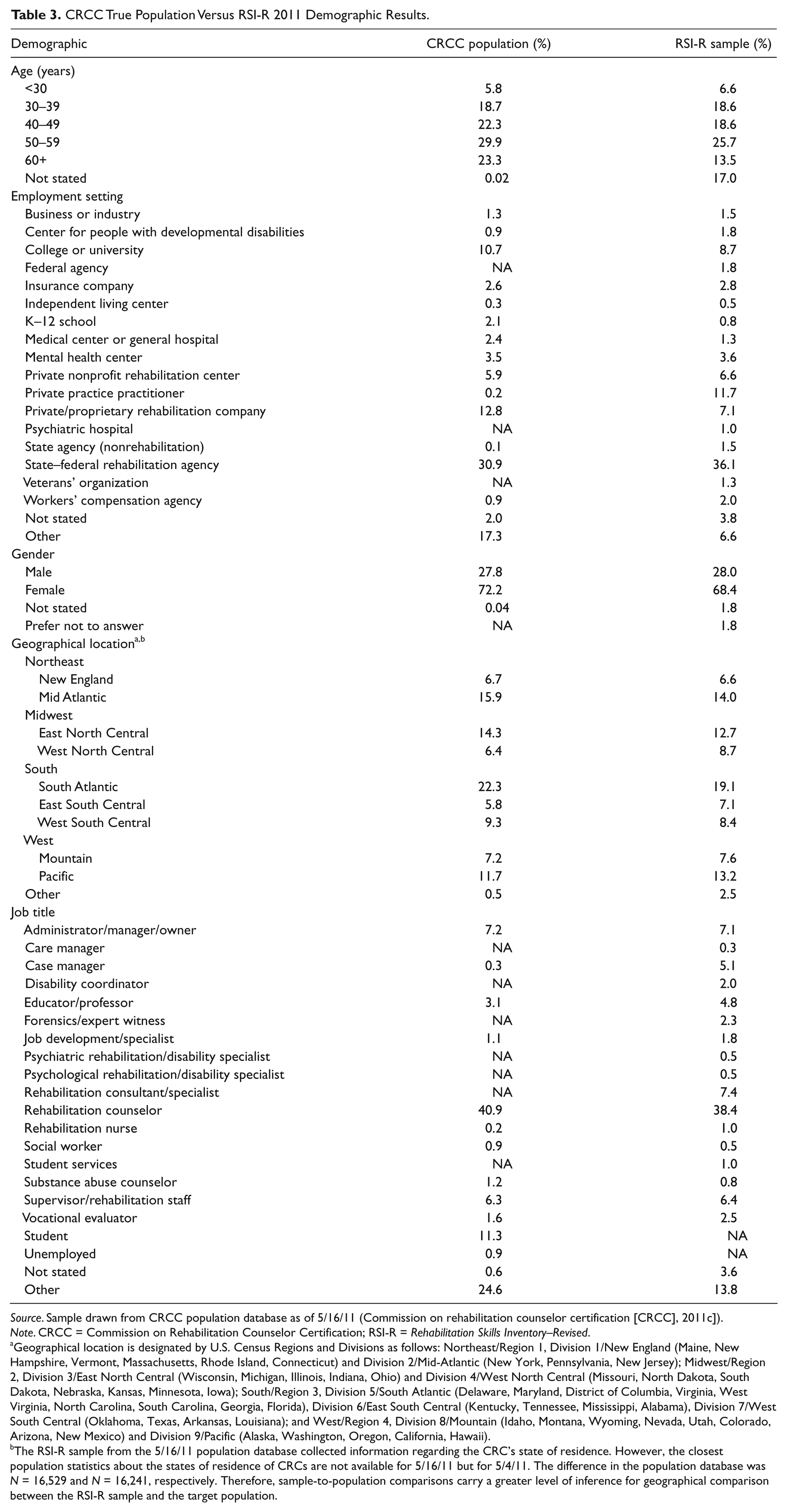
Source. Sample drawn from CRCC population database as of 5/16/11 (Commission on rehabilitation counselor certification [CRCC], 2011c]).
Note. CRCC = Commission on Rehabilitation Counselor Certification; RSI-R = Rehabilitation Skills Inventory–Revised.
Geographical location is designated by U.S. Census Regions and Divisions as follows: Northeast/Region 1, Division 1/New England (Maine, New Hampshire, Vermont, Massachusetts, Rhode Island, Connecticut) and Division 2/Mid-Atlantic (New York, Pennsylvania, New Jersey); Midwest/Region 2, Division 3/East North Central (Wisconsin, Michigan, Illinois, Indiana, Ohio) and Division 4/West North Central (Missouri, North Dakota, South Dakota, Nebraska, Kansas, Minnesota, Iowa); South/Region 3, Division 5/South Atlantic (Delaware, Maryland, District of Columbia, Virginia, West Virginia, North Carolina, South Carolina, Georgia, Florida), Division 6/East South Central (Kentucky, Tennessee, Mississippi, Alabama), Division 7/West South Central (Oklahoma, Texas, Arkansas, Louisiana); and West/Region 4, Division 8/Mountain (Idaho, Montana, Wyoming, Nevada, Utah, Colorado, Arizona, New Mexico) and Division 9/Pacific (Alaska, Washington, Oregon, California, Hawaii).
The RSI-R sample from the 5/16/11 population database collected information regarding the CRC’s state of residence. However, the closest population statistics about the states of residence of CRCs are not available for 5/16/11 but for 5/4/11. The difference in the population database was N = 16,529 and N = 16,241, respectively. Therefore, sample-to-population comparisons carry a greater level of inference for geographical comparison between the RSI-R sample and the target population.
The database for this study contained 393 responses. Of the respondents providing data on gender, 28.0% were males and 68.4% were females. More than one third (34.6%) of CRCs lived in the South, with the other respondents almost evenly distributed among the Northeast (20.6%), Midwest (21.4%), and West (20.9%) U.S. Census regions. The largest age group was between 50 and 59 years (25.7%). In addition, CRCs with less than 5 years of post-certification experience represented the largest group (24.2%) of respondents. This possibly reflects a change in the CRC exam from paper to computer-based testing in 2008 that allowed for more frequent and longer periods of administration; thus, its use as a comprehensive exam by graduate programs potentially captures a greater number of early entrants into the profession bolstering the numbers in this demographic group. Nearly all respondents had obtained graduate education (94.7%), with the majority of CRCs possessing a master’s degree (88.3%) with a major area of study either in rehabilitation counseling or rehabilitation psychology (75.8% together).
One third of respondents (66.7%) did not report a disability. The most frequent disability identified was orthopedic or physical (13.2%) followed by hearing (3.1%), visual (2.5%), cognitive (2.3%), and psychiatric (2.0%). Although 16 distinct employment settings were identified in the study, nearly half of CRCs (47.8%) either worked for state/federal rehabilitation agency programs or were in private practice. Of the 17 professional job titles identified by respondents, rehabilitation counselors and consultants/specialists made up nearly half (45.8%).
The CRC credential was identified as being held by over 95% of those responding to the survey. Although the sample was drawn from a complete CRC population database, the difference in those reporting having a CRC from 100% of the population could be attributed to nonanswers, the identification of secondary credentials and not claiming the CRC as being held concurrently, a lapsed credential in the 4-month period between when the sample was drawn and the RSI-R administered, or respondent error. Nearly half of CRCs (49.6%) did not belong to a professional organization. Of those who held membership, those organizations most frequently cited were the National Rehabilitation Association (18.3%), the International Association of Rehabilitation Professionals (13.0%), and the American Counseling Association (9.2%).
Importance and Use of Occupational and Labor Market Information by CRCs
Importance
As noted in Table 1, of the 11 labor market and occupational information items selected from the CRCC job analysis, all items had mean scores between important and extremely important for these competencies in rehabilitation counseling practice. Although conducting LMAs was in the lowest end of the mean range (M = 2.02, SD = 1.28) of the RSI-R items studied, it also had the highest standard deviation suggesting perhaps a greater level of variability among respondents compared with the other 10 survey items. The transferable skills that are assumed in the person/job match when considering occupational and labor market data were identified as very important to extremely important (M = 3.24, SD = 1.07), or the highest end of the range and having the lowest standard deviation among all items, suggesting less dispersion among CRCs as to their belief in its importance in practice.
Use by CRCs
When considering how frequently CRCs use the competencies involving occupational data in rehabilitation counseling practice, of which LMS could be a part, responses had a much broader distribution than the importance ratings. The responses ranged from close to very infrequent for conducting LMAs (M = 1.50, SD = 1.39) to very frequent for the identification of transferable work skills (M = 2.89, SD = 1.20). Again, these two items reflected the ends of the continuum of mean ratings for all 11 items. Although the mean for conducting LMAs was in the lowest end of the range, its standard deviation suggests that many CRCs may not perform this task in practice, whereas others may perform it very frequently.
Differences in the Use of LMS Among CRCs
To address the second research question, a one-way ANOVA was conducted for each demographic variable and the mean frequency of Item 2, “Conduct Labor Market Analyses” (LMAs). This item was thought by the researchers to be the most proximal of all the RSI-R survey questions to encompassing the collection of activities in primary labor market collection indicative of LMS per the definition identified in this research and the current literature. As indicated earlier in this article, the definition of LMA, which is synonymous with LMSea, is a model that includes LMR (secondary) and LMS (primary) data. Post hoc analyses were then performed to examine group differences. Specifically, the Games-Howell post hoc analysis was selected because it has been designed for situations in which population variances differ and is also accurate when sample sizes are unequal (Field, 2009)—both of which apply to this data set.
For Item 2, ANOVAs revealed significant differences at p < .05 among age, gender, education, area of study, geographic location, work experience, employment setting, and job title. No differences were found by disability status (p < .705). Each of these areas of significant difference was further examined.
Age
Individuals who indicated they were 60 or older reported conducting LMAs somewhat frequently as opposed to the other age groups who indicated they conducted them less frequently. There was a significant difference in the mean reported frequency of conducting LMAs between the 60 and above age group and those who fell into the below 30 (p < .025), 30 to 39 (p < .000), and 50 to 59 (p < .017) age groups. There was also a significant difference between the 30 to 39 and the 40 to 49 age ranges such that those in the 40 to 49 age group indicated performing this competency more frequently than those in the younger group (p < .038).
Education
Although the results of an ANOVA indicated a significant difference between one or more levels of education, the post hoc analyses did not reveal significance. The post hoc, by nature, controls for the number of tests and becomes more conservative as the number of groups compared increases. Consequently, it is possible to find group differences with an ANOVA that cannot be captured by subsequent post hoc analyses because of their level of conservativeness. It is also possible that this discrepancy could be the result of Type I error where the level of education may not truly be a significant factor despite the ANOVA.
Area of study
The CRCs who reported conducting LMAs with the highest frequency within area of study were those whose highest degree was in education (M = 3.11). There were statistical differences within major areas of study and the frequency with which these groups conducted LMAs. Individuals who indicated their highest degree was in education performed LMAs more frequently than those with their major area of study in rehabilitation psychology (M = 0.33) or other counseling specialties (M = 1.25) with a significance of p < .003 and p < .047, respectively. Rehabilitation counselors indicated they performed LMAs (M = 1.45) significantly more (p < .001) than those with a major area of study in rehabilitation psychology (M = 0.33). There was also a significant difference between the frequency with which those in rehabilitation psychology and those in psychology (M = 1.78) conducted LMAs (p < .020).
Further examination of individuals whose major area of study was education reveals that these individuals tend to be older with more than half of them being above 50 years of age. These CRCs also tended to hold the job title of rehabilitation counselor (33%) or rehabilitation consultant/specialist (33%), and has an extensive amount of work experience with all having a minimum of 10 years experience and nearly half (44.4%) having more than 25 years of experience. Two thirds of these individuals report being employed in either the private/proprietary rehabilitation setting (33.3%) or as a private practice practitioner (33%). It is important to note that the number of those indicating education was their major area of study was small (n = 9). However, it is also important to note that one of the primary reasons the Games-Howell post hoc analysis was chosen was its ability to account for small ns and a difference in ns when comparing groups. As we review the demographics of this group, this result is also consistent with the earlier finding that individuals who were older tended to report conducting LMAs more frequently than younger groups of individuals.
Geographic location
Individuals residing in the West/Pacific region reported the highest mean frequency of conducting LMAs (M = 2.33), which was significantly more than the following geographic areas: Northeast/Mid Atlantic (M = 1.20, p < .005), Midwest/East North Central (M = 1.26, p < .004), South/South Atlantic (M = 1.37, p < .012), and South/East South Central (M = 1.04, p < .004). No other differences by geographic location were found.
Work experience
Individuals who reported having post-CRC work experience of 20 to 25 years also reported the highest mean frequency of conducting LMAs (M = 2.19) and were significantly different from the individuals with the least amount of work experience, specifically, those respondents with less than 5 years (M = 1.24, p < .010) and with 5 to 9 years of post-CRC work experience (M = 1.23, p < .015). The group with the highest amount of post-CRC work experience of more than 25 years had the second highest mean of the group at 1.81.
Gender
A significant difference (p < .038) between men and women was revealed, with men (M = 1.80) conducting LMAs more frequently than women (M = 1.37). Although the largest percentage of both groups tended to be employed as rehabilitation counselors within the state/federal rehabilitation system, when we examined the data more closely, we found significant differences on many demographic variables by gender.
The men in this sample were significantly older (p < .000) with an average age of 40 to 49 years and with 27.3% of all men falling in the 50- to 59-year age range. The mean age for women in this sample was 30 to 39 years, with nearly 30% of the women falling into this age range or into younger age ranges. In addition, men tended to have more work experience post-CRC than women (p < .001), with 25.5% of men having more than 25 years of experience and 39.1% having 20 or more years of experience. In contrast, the largest percentage of women (26.0%) fell into the under 5 years work experience post-CRC group, and nearly half (46.0%) reported having 9 years or less of work experience post-CRC. These findings are consistent with earlier results in this study revealing that older and more experienced professionals tended to conduct LMAs more frequently than other groups in the course of their job.
Employment setting
Those CRCs whose employment setting was reported as an independent living center noted the lowest mean frequency for conducting LMAs (M = 0.00). Analyses suggested a significant difference between this group and several other groups that reported a higher frequency for performing LMAs in the following employment settings: college or university (M = 1.00, p < .005), private/nonprofit rehabilitation center (M = 1.23, p < .005), private practice practitioner (M = 2.15, p < .000), private/proprietary rehabilitation company (M = 2.79, p < .002), and state/ federal rehabilitation agency (M = 1.39, p < .005).
Two other employment settings that had high mean frequencies for LMAs, private practice practitioner (M = 2.15) and private/proprietary rehabilitation company (M = 2.79), had significantly higher mean frequencies than several of the other employment settings. Specifically, private/proprietary rehabilitation company was the employment setting with the highest mean frequency of all employment settings for LMAs and was significantly higher than the following settings: center for developmental disabilities (M = 0.43, p < .000), college or university (M = 1.00, p < .000), private nonprofit rehabilitation company (M = 1.23, p < .007), psychiatric hospital (M = 0.25, p < .001), state/federal rehabilitation agency (M = 1.39, p < .001), and other (M = 0.81, p < .000). Private practice practitioner was the second highest employment setting in terms of mean frequency of conducting LMAs, and post hoc analyses revealed the mean frequency of this employment setting was significantly higher than those working in center for developmental disabilities (M = 0.43, p < .001), college or university (M = 1.00, p < .030), psychiatric hospital (M = 0.25, p < .014), and other (M = 0.81, p < .006).
Job title
An ANOVA revealed a significant difference between one or more pairs of job titles and the frequency with which they report performing LMAs (p < .000). The group with the highest mean frequency was forensic/expert witness (M = 3.22) and the group with the next highest mean frequency was rehabilitation consultant/specialist (M = 2.48). There were two groups with the lowest mean frequency—psychiatric rehabilitation/disability specialist and career counselor—both groups had a mean frequency of 0.00. Post hoc analyses revealed that the group with the highest mean frequency, forensics/expert witness, reported conducting LMAs more frequently than career counselors (p < .001), educator/professor (p < .032), disability coordinator (p < .001), psychiatric rehabilitation/disability specialist (p < .001), substance abuse counselor (p < .042), supervisor (rehabilitation staff; p < .019), and other (p < .003). The two groups with the lowest mean frequency (psychiatric rehabilitation/disability specialist and career counselor) conducted LMAs significantly less than the following groups: administrator/manager/owner (p < .002), case manager (p < .042), educator/professor (p < .012), forensics/expert witness (p < .001), rehabilitation consultant/specialist (p < .000), rehabilitation counselor (p < .000), supervisor (rehabilitation staff; p < .001), and other (p < .002).
Differences in CRC Use of Other Occupational and Labor Market Data
Although conducting LMAs was examined more closely given the proximity of that RSI-R item to the purpose of this study and definition of LMS, the 10 other survey items selected as the universe of items on occupation and labor market data and applications on the instrument for examination were likewise studied at the level of demographic areas of significance. ANOVAs demonstrated that all 10 other items were significant for demographic variables involving employment setting and job title. Age was only significant for the items involving the identification of transferable skills in analyzing clients’ work history and functional assets and limitations (Item 6) and identifying hidden job leads and customizing jobs/employment opportunities (Item 5). Education and area of study demographic variables were significant for Item 9 that involved making logical job, work area, or adjustment training recommendations based on comprehensive client assessment information. The work experience demographic variable was significant for Item 1, applying labor market information influencing the task of locating, obtaining, and progressing in employment. Finally, gender was significant when examining the use of local resources to assist with placement (Item 11). The demographic variables that were not found to be significant across any of the 10 items studies included education, type of disability, and location.
Generalizability of This Study to CRCC Target Population
Information regarding the population from which the RSI-R sample was drawn found that of the 11 demographic variables, 4 included in the sample could be compared with the CRCC target population for purposes of generalizability, which is important in a benchmarking study to determine how well the sample reflects the true target population from which it was drawn and to which it generalizes. As mentioned earlier, the other demographic variables collected in the RSI-R sample are not likewise kept for the CRCC database, thereby not allowing for a direct comparison. The demographic variables in Table 2 detail RSI-R demographic content that was exclusively collected for the sample and thus could not be directly compared with the CRCC database. In the instance of the CRCs’ work experience, the way the question was asked for the sample differed from the way it was asked for the population; however, this did not seem to have a significant impact on the distribution of the data across experience ranges between the sample and the population. Table 3 details the comparison between the sample demographics and those of the target population, where there is a direct comparison. Examining the data for variables where there was greater than a 5% difference between the sample and the population, it appears that in those 60 years of age and older, the CRCC population was reported at 23.3%, whereas the sample was at 13.5%. This difference was largely accounted for by the manner in which respondents answered this question for both sets of data; that is, only .02% of the CRCC population did not provide data on age while 17.0% of the sample did not report their age.
There was also a relative difference when comparing the statistics between the population and sample for the private/proprietary rehabilitation company and state–federal rehabilitation agency practice settings. The 5.7% lower share of those in the private/proprietary rehabilitation company respondents to the RSI-R survey than in the population was almost completely offset by the 5.2% higher difference in the state/federal rehabilitation agency respondents. Given the research by Neulicht et al. (2007) and Barros-Bailey and Heitzman (2011) on the use of LMS in forensic activities, and the results of this study as to the significant difference of use of LMAs by CRCs in these practice settings, this relative difference between the sample and the population could have resulted in an underreporting of the importance and use of occupational data by CRCs. There were significantly less (10.7%) respondents in other practice settings categorized for the job analysis than those noting practicing in other settings within the population database.
In comparing the RSI-R sample with the CRCC population (N = 16,259), a post hoc power analysis performed on the sample (N = 393) suggests that the study had good power, with a margin of error of .04889 at a 0.95 confidence interval. Overall, markers that allow for comparability suggests that the 2011 RSI-R sample seems to generalize well to the population from which it was drawn.
Discussion
Limitations and Delimitations
There were several limitations to this study. Although the purpose of this research was to examine and benchmark the use of LMS, none of the survey items in the RSI-R directly queried respondents as to their attitudes of the importance or their frequency of use of LMS. Consequently, the 11 items selected for this study from the data collection instrument resulted in each item having different levels of inference as to how distal or proximal it might be to the core purpose of the study along a continuum of the collection and application of primary labor market data that define LMS. However, the items selected from the instrument involved the universe of the use of occupational and labor market data in rehabilitation counseling and fit broadly the selection criteria for the study. The items were also consistent with whether they reflected primary or secondary data sources, of which LMS could be a component. Because of the potentially confounding effect of LMS being included and subsumed into the terms defining the collection or application labor market or occupational data, respondent bias or error might have been introduced by those who could have assumed different concepts, meanings, and definitions of LMA to include or exclude LMS, or other selected items.
There were three primary delimitations in this study involving the inferential statistical examination of the data. First, only respondent answers to the frequency query were examined, with the LMA question singled out of the 11 items for further examination by each of the demographic variables because it was thought by the researchers to likely contain responses more directly associated with primary data collection reflective of LMS. The other 10 variables did not receive as detailed a review in the between-group analysis. Second, the researchers did not perform ANOVAs involving respondent attitudes toward the importance of each of these items to practice because this was not determined to be within the primary scope of this study. Finally, because of the manner in which the data were collected, the demographic variables associated with Credentials and Professional Organizations variables produced confounding results that did not lend themselves to inferential statistical analysis.
Conclusion
Rehabilitation counselors use labor market and occupational information in practice as expected, given the competencies outlined in credentialing (CRCC, 2011a) and accrediting (CORE, 2011) standards. Although the RSI-R instrument does not have an item specific to LMS, it does contain 11 items that involve competencies using or collecting occupational and labor market information, of which LMS is a methodology for collecting primary data. The 11 items studied from the 2011 RSI-R administration constitute the universe of items relevant to this research.
This research suggested that LMAs were rated as important to extremely important by CRCs and performed along a range of very infrequent to very frequent. Among the 11 survey items studied, the importance and use of LMA was considered the lowest in importance and frequency of all items with the importance and use of such data for transferable skills analyses where information about occupations and labor markets is matched with individual characteristics being the highest form of application of such data. Overall, those CRCs reporting the highest frequency of use of LMA where older, male, possessed education in rehabilitation-orientated areas of study, had more than 20 years of post-CRC experience, were in the private/proprietary rehabilitation or private practice practitioner professional settings, and held the job title of forensic/expert witness or rehabilitation consultant/specialist. With a greater number of female entrants into rehabilitation counseling over the last 25 years, it is not surprising males who are within the older age cohort of the target population, who have greater experience, and who have gravitated toward the practice settings where LMS is most frequently performed would represent the demographic profile of CRCs reflected in this research. Considering all 11 items studied in this research, practice setting and job title were consistent as being significant across the entire universe of items where these data are collected or used in the rehabilitation counseling process. The practice setting and job title findings were consistent with those of Neulicht et al. (2007) and Barros-Bailey and Heitzman (2011), suggesting these were the same practice settings where the use of LMS is found extensively. These private sector practice settings were also identified by CRCs in the previous 2006 job analysis to be the areas of greatest growth in the profession (Barros-Bailey, Benshoff, & Fischer, 2009).
Implications and Suggestions for Future Research
This first benchmarking study attempted to provide data regarding the importance and use of LMS or related labor market and occupational data competencies across and among a variety of demographic variables for CRCs. As a benchmarking study, it is the foundation from which other studies could emanate and greater implications could be derived for rehabilitation counseling. The importance of labor market and occupational data knowledge and how prepared CRCs feel they are to use its merits further study because of its potential impact on education and training for those practicing in a sector of rehabilitation counseling that critically affects the lives of people with disabilities.
Given the use of labor market and occupational data in vocational exploration, rehabilitation plan development, job placement, and forensics, greater effort is needed to obtain more information on how CRCs define and use LMS and LMA across practice settings, including the methodologies used in data collection and reporting. The implications for the use of such data on client rehabilitation outcomes and the ramifications of its potential abuse merit more focused attention.
Beyond more dedicated study of the use of LMS and LMA in the private sector rehabilitation settings that garnered the greatest level of importance and use ratings by CRCs in this benchmarking study, the study of the use of labor market and occupational data in the state–federal rehabilitation agencies should also be further researched. As a single cohort, the state–federal program represents the largest number of CRCs. Although as a cohort the importance and use of labor market and occupational data was estimated to be lower in the public sector compared with CRCs in the private sector, the use of LMS or the general use of occupational and labor market data deserves further examination given the expenditure of public funds for the rehabilitation of individuals with disabilities and the importance of accurate use of such data in developing rehabilitation plans and in job placement efforts. For example, in 2011, one of the authors performed a LMS census of 153 employers in a single county area in a southwestern state for a specific job classification for a client undergoing training through the local state–federal system agency. Although the training plan had been justified and supported using federal secondary labor market data using its most recent release, there had been no attempt at gathering primary LMS data regarding the vocational goal. The LMS demonstrated that 66% of the businesses could no longer be located. Of the remaining businesses, none were hiring at the time of the calls, one had hired over the last year, and none planned to hire in the upcoming year. Those who hoped to be in a business position to hire in the future suggested they would draw from their pool of laid-off employees rather than seek new employees for any future hiring. Even a sample of the population of employers contacted, perhaps using a self-directed approach as suggested by Gilbride and Burr (1993), would have provided the state–federal agency counselor and client with decision-making information to supplement secondary information sources that tend to be older, more aggregated, and less sensitive to the realities of the local labor market, and effect better decision making in plan development, thus a better use of tax dollars.
The results of this research and of future research in this area will surely benefit rehabilitation counseling programs, educators, and students of rehabilitation counseling. All accredited rehabilitation counseling programs are required to teach competency standards involving occupational and labor market information in the rehabilitation counseling process to meet the criteria for and to maintain accreditation. Competencies in the use of labor market information and occupational data, of which LMS and LMA are a part, are important. There has never been a comprehensive examination of rehabilitation counselors in all practice settings and demographics that benchmarks the use of LMS, and little research exists on the use and practice of utilizing LMS in rehabilitation counseling and disability services (Barros-Bailey, 2011, in press; Neulicht et al., 2007).
Although this study included descriptive statistics as to the importance of ratings by CRCs on the 11 survey items, inferential statistics only examined the use of these competencies due to the purpose of this research. No information is available from a national sample as to how CRCs collect and use these data across practice settings or other demographic variables. Therefore, an inferential study of importance ratings for competencies and knowledge ratings by CRCs could be an area for further study. Other research could apply the methods used in this study to another credentialing organization’s role and function database containing survey items with labor market and occupational information constructs to determine how those certificants are benchmarked for the same or similar competencies.
The CRCC job analysis study is descriptive cross-sectional research that captures data about a CRC’s role and functions at a specific point in time when the survey is performed. As a cross-sectional survey research, it is limited by the snapshot that it takes at any given moment. The RSI-R was originally created 25 years ago and has captured over time the ratings among rehabilitation counselors about the use of LMS and occupational data. A longitudinal comparison on the items used in this study could provide some valuable information for future education and training efforts.
This research begins to fill a significant gap in our professions’ research and knowledge base by providing benchmarking information on a critical and required area of practice. It provides a foundation for future research that could eventually lead to the establishment of best practices in the area of LMS. These results provide a base of information to inform researchers and educators in rehabilitation counseling and consequently, their students. This information will not only benefit researchers, educators, and practitioners in the field of rehabilitation counseling but also students of these programs by increasing their knowledge and skills in the practice of conducting and utilizing LMS. Perhaps most importantly, it will ultimately get rehabilitation counseling closer to better serving persons with disabilities by utilizing evidence-based practices in LMS when primary data are needed in service delivery decision making.
Footnotes
Acknowledgements
The authors would like to thank the Commission on Rehabilitation Counselor Certification (CRCC) for permission to study the data of the 2011 job analysis specific to this research, and in particular Cindy Chapman and Susan Stark for all their assistance. In addition, we would like to thank Dr. Michael Leahy for sharing data from the overall 2011 CRCC job analysis.
Authors’ Note
For more information about this research, contact Mary Barros-Bailey, Intermountain Vocational Services, Inc., P.O. Box 7511, Boise, ID 83707-1511,
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.