
Abstract
Despite medical advancements that have significantly improved the health outcomes of people living with HIV (PLWH), many do not achieve optimal health outcomes due to psychosocial barriers. This 5-year retrospective longitudinal study draws upon the International Classification of Functioning, Disability, and Health (ICF) framework to conceptualize the relationships between personal and environmental factors and health and retention outcomes among a sample of 704 PLWH in Pennsylvania. A generalized estimated equations (GEE) model was used to model retention in care outcomes (at least one medical visit every 6 months) and a general linear mixed (GLM) model was used to analyze immune system health outcomes (CD4%). This exploratory study reveals that gender, age, race, use of antiretroviral (ARV) medications, use of case management service, mental health diagnosis, and alcohol use were significantly associated with retention in care, whereas race, ethnicity, gender, mental health treatment, use of ARV medications, use of case management services, and retention in care status were significantly associated with the immune system health outcome of CD4%. The results suggest a need for rehabilitation interventions to address key psychosocial issues, as rehabilitation counselors have a unique skill set to address the medical case management needs of individuals with HIV. Implications for rehabilitation counselors and educators are discussed.
Keywords
Introduction
The National HIV/AIDS Strategy (NHAS) was issued in 2010 by President Obama as the first national strategic plan to address the domestic HIV epidemic (White House Office of National AIDS Policy, 2010). The NHAS includes three primary goals: (a) reducing new HIV infections, (b) increasing access to care and optimizing health outcomes, and (c) reducing HIV-related health disparities and inequities (White House Office of National AIDS Policy, 2010). To meet these goals, facilitating access to and retention in antiretroviral (ARV) treatment has become a primary effort in HIV care. Effective treatment can lead to viral suppression indicating that the amount of HIV virus (i.e., viral load) in the blood is undetectable. When viral suppression is maintained, the risk of onward HIV transmission is negligible, even without other prevention methods such as condom use (Rodger et al., 2016).
To monitor progress toward achieving the goals of the NHAS, the Centers for Disease Control and Prevention (CDC; 2017) uses the HIV Care Continuum framework to track HIV incidence and treatment rates at critical points from initial diagnosis through successful viral suppression. National data (CDC, 2016a) revealed that only 87% of the estimated 1.2 million individuals living with HIV in the United States were aware of their HIV status, even fewer (74.5%) were linked to HIV medical care within 1 month of HIV diagnosis, only 56.5% were retained in care, and just more than half (54.7%) achieved viral suppression (viral load < 200 copies/mL on the most recent test; CDC, 2016b). These statistics underscore that a large proportion of people living with HIV (PLWH) do not achieve optimal health and retention outcomes, which poses a significant threat to the nation’s ability to end the AIDS epidemic.
Fleishman et al. (2012) found that 21.7% of the 22,984 adults living with HIV never established HIV treatment after their initial medical appointments. These findings underscores the urgent need to facilitate early linkage and retention in care in HIV treatment (Gardner, McLees, Steiner, del Rio, & Burman, 2011; Heckman, Catz, Heckman, Miller, & Kalichman, 2004; Lourenço et al., 2016). Retention in care is often defined as having at least two medical appointments in a year, which were 3 months apart (Health Resources and Services Administration [HRSA] HIV/AIDS Bureau [HAB]; HRSA HIV/AIDS Programs, 2013). Research has shown that retention in care is highly associated with improved biological health outcomes (i.e., increased CD4 counts and viral suppression; Mugavero et al., 2012; Yehia et al., 2014), increased survival rate (Mugavero et al., 2009), reduced transmission rate (Metsch et al., 2008), and decreased HIV-related complications (Yehia et al., 2014).
There are a wide range of psychosocial barriers to retention in care among PLWH, including HIV-related stigma, mental health concerns, racial and ethnic minority status, lack of insurance, work schedule conflicts, lack of housing stability, low motivation, injection drug use, and lack of access to HIV treatment (Fleishman et al., 2012; Hwang & Nochajski, 2003; Lourenço et al., 2016; Mizuno et al., 2015; Mugavero et al., 2009; Myezwa, Buchalla, Jelsma, & Stewart, 2011; Paterson et al., 2000; Syed et al., 2016). In a qualitative study, Kempf et al. (2010) found that many contextual factors were the primary barriers to retention in care among women living with HIV, including the quality of the patient–provider relationship, transportation, and health care facility location. Similarly, Sevelius, Keatley, and Johnson (2014) identified that service providers play a key role in PLWH’s treatment engagement. These findings illustrated how personal and contextual factors, as well as service factors, are all critical in the HIV continuum of care.
Case management (CM) has been identified as an essential HIV service by the HRSA HAB (HRSA HIV/AIDS Programs, 2013). The Ryan White HIV/AIDS Treatment Modernization Act (2006) defined Medical CM as a core service and allowed nonmedical CM services to be funded under support services. Medical CM is a proactive and long-term approach that addresses PLWH’s complex health and psychosocial needs (e.g., housing, nutrition, and employment needs; New York State Department of Health [NYDOH], 2006). Studies show that CM services increase the likelihood of early linkage and engagement in HIV medical care, as well as early linkage to psychosocial services (Craw et al., 2008; Gardner et al., 2005; Willis et al., 2013). Unfortunately, the number of longitudinal empirical studies examining the association of CM service and retention in care is more limited. Gaining a better understanding of the use and impact of CM services on retention in care and immune system health outcomes over time will help to inform service organizations, stakeholders, and professionals about key factors to consider when providing these services.
As HIV/AIDS has shifted from an acute disease to a chronic illness, which can lead to a disability (Conyers, Chiu, Shamburger-Rousseau, Johnson, & Misrok, 2014; Swendeman, Ingram, & Rotheram-Borus, 2009), rehabilitation counselors and educators have responded to the needs of individuals with HIV through education, research, and practice (Conyers, 2005; Hergenrather, Geishecker, Clark, & Rhodes, 2013; Hergenrather, Rhodes, & McDaniel, 2005; Jung, Schaller, & Bellini, 2010; Kohlenberg & Watts, 2003). One reflection of this increased need for rehabilitation services was the 67% increase in the numbers of consumers with HIV exiting the public vocational rehabilitation (VR) program from 2002 through 2007 (Jung & Bellini, 2011). In a study of public VR counselor attitudes about serving consumers with AIDS, Hergenrather et al. (2005) reported that 55.6% of respondents noted that they served consumers with AIDS. It is likely that the HRSA data underestimate the numbers of PLWH who used VR services, as many qualify under other primary/secondary (e.g., mental health, visual impairment) disability categories (S. DeRobertis, personal communication, August 26, 2016). With respect to impact of VR services on public health outcomes, Conyers and Boomer (2014) found that use of VR services was associated with access to care and reduced health risk behaviors. Traditionally, most rehabilitation counselors have worked in public VR agencies; however, as the field of rehabilitation counseling has evolved, there are more rehabilitation counseling professionals working in private nonprofit and private for-profit sectors (Barros-Bailey, Benshoff, & Fischer, 2009; Zanskas & Strohmer, 2011).Within these varied settings, rehabilitation counselors can play an important role in facilitating retention in care of PLWH, as CM has been identified as an essential skill of rehabilitation counselors (Leahy, 2012).
Conceptual Framework: The International Classification of Functioning, Disability, and Health (ICF)
The World Health Organization (WHO) developed the ICF in 1980 (updated in 2002) to provide a universal framework and classification for health-related conditions. The ICF places an emphasis on one’s health and functioning, rather than disability, reflecting the core values of the rehabilitation profession. Individual functioning is viewed as interactions between one’s health conditions (e.g., disorder, disease, injuries) and contextual factors (i.e., environmental and personal factors). The ICF can be used to guide intervention or outcome studies as it addresses individual outcomes in a specific context (WHO; 2002). In this study, we applied the ICF as a framework to understand how personal and environmental factors affect PLWH’s immune system health outcomes and retention in care. We discuss the rationale of selecting each variable using the ICF framework below.
Individual Functioning: Outcome Indicators
Using the ICF framework, we discuss HIV as a complex health condition that can be associated with a disability status to the extent to which it affects individual level of functioning in the domains of body function and structure, activity limitations, and participation restrictions (WHO, 2002). Activity refers to tasks or actions a person conducts in his or her major life areas; participation refers to the level of involvement in a life situation (WHO, 2002). Retention in care is a key indicator of the level of participation in treatment, which is directly related to PLWH’s health outcomes and functional levels (CDC, 2016b). As mentioned earlier, HRSA HIV/AIDS Programs (2013) defined retention in care as having at least one medical service visit in each 6-month period of the 12-month measurement period with a minimum of three or more months between each visit. This study applied a more conservative outcome measure: whether a client had at least one medical service visit in each 6-month period of the 12-month measurement period.
With respect to HIV, immune system functioning is key to PLWH’s bodily functions (e.g., psychological and physiological function of one’s body systems), and a weakened immune system associated with HIV can lead to significant impairments of body structure (e.g., limbs and organs). Two key measures of immune system health are the CD4 count (the number of CD4 cells in a sample of an individual’s blood) and CD4% (the percentage of CD4 cells of the total white blood cells). When HIV attacks a person’s immune system, CD4 cells (often called T cells) are slowly destroyed and, as the body loses more and more CD4 cells, the ability to fight off infections and diseases is substantially compromised. The CD4 count of a person without HIV typically ranges from 500 cells/mm3 to 1,200 cells/mm3 (Malaza, Mossong, Bärnighausen, Viljoen, & Newell, 2013). When a PLWH’s CD4 count becomes lower than 200 cells/mm3 or the CD4% is below 14%, he or she meets the criteria for an AIDS diagnosis (CDC, 2016b). Higher CD4 count and CD4% is associated with better health; with effective ARV treatment, PLWH can increase their number of CD4 cells and achieve CD4 levels within the normal range. We chose CD4% as our outcome measure in this study. CD4% is a more stable measure of HIV health because the absolute number of CD4 cell counts can fluctuate due to stress, time of day, and non-HIV concurrent infections (Claassen, Diener-West, Mehta, Thomas, & Kirk, 2012; Hulgan et al., 2007). CD4% is also often viewed as a better indicator of health for PLWH who are in medical care and have CD4 counts above 200 cells/mm3 or adults who are HIV negative; the CD4% typically ranges from 24% to 64% with an average of 45% (Malaza et al., 2013).
Environmental Factors
Environmental factors refer to any physical, social, and attitudinal barriers or facilitators in altering, mediating, and enhancing one’s functioning (Chapireau, 2005; WHO, 2002). These factors range from architectural characteristics, climates, policies, and regulations, to service delivery systems. Studies have shown that many environmental factors were associated with PLWH’s health outcomes, including family support, quality of health care professionals, societal attitudes, policies, service systems, and technology (Hwang & Nochajski, 2003; Myezwa et al., 2011). In the current study, receipt of HIV medical CM services was used as a primary environmental factor because it has become one of the essential services to PLWH (Gardner et al., 2005; HRSA HIV/AIDS Programs, 2013).
Previous studies demonstrated a positive impact of CM services on PLWH’s treatment outcomes. Kushel et al. (2006) found that of PLWH who were homeless or marginally housed and those who received CM services achieved better ARV therapy adherence and more gains in CD4 counts, compared with those who did not receive CM services. Brennan-Ing et al. (2016) found that PLWH who were enrolled in a Comprehensive Case Management Medicaid Program had significant improvements in their CD4 count over time, compared with those who never enrolled. Notably, little research has been done to examine the association between intermittent use of CM services on changes in PLWH’s immune system health and retention in care outcomes over time.
Clinic location was another environmental factor included in this study. Researchers found that individuals’ health behaviors and outcomes differ geographically due to demographic, local economic, and sociocultural factors (Heckman et al., 2004). Cesnales (2012) noted that PLWH who live in rural and semirural areas experience unique challenges to remaining in medical and psychosocial services due to lack of access to accessible and affordable health care as well as other social resources. According to CDC (2008), large metropolitan areas are those with populations greater or equal to 500,000; medium metropolitan areas are those with a population ranging from 50,000 to 499,999; nonmetropolitan areas are those with populations fewer than 50,000. This current study grouped the treatment sites that are in large and medium metropolitan areas as urban settings and those in nonmetropolitan areas as rural settings to compare the effect of urban/rural setting on the outcomes of interest.
Personal Factors
Within the ICF framework, personal factors include race, ethnicity, gender, education level, family, and other personal characteristics that could influence one’s experience of a health condition (WHO, 2002). Research has identified many personal factors that are associated with HIV treatment outcomes, including demographic factors (e.g., age, race, ethnicity, gender), ARV medication adherence, retention in care, use of drug or alcohol, mental health status, and overall health status (Fleishman et al., 2012; Lourenço et al., 2016; Mizuno et al., 2015; Paterson et al., 2000; Syed et al., 2016). We selected the major demographic factors of gender, race, ethnicity, and age. The demographic information was collected at the intake assessment. We also used other key individual health-related information, collected at key time intervals over the study period, as personal factors: use of ARV medication, mental health diagnosis, mental health treatment, drug use, and alcohol use.
Gaining a better understanding of the impact of medical CM services on PLWH is important as this is an area in which rehabilitation professionals can make an impact to improve public health outcomes. Understanding the impact of various personal and environmental factors on PLWH’s health outcomes can also help to inform rehabilitation and health care policy and practice to improve individual and public health outcomes. To this end, the following two research questions were investigated:
Method
Study Design
A retrospective longitudinal study design was implemented to examine the association of personal (demographic characteristics, use of ARV medications, mental health diagnosis, mental health treatment status, drug and alcohol use) and environmental factors (use of CM, rural vs. urban treatment sites) on PLWH’s health and retention outcomes. The two key outcome measures were repeated measures of retention in care status (defined as having at least one medical visit within the previous 6 months) and CD4% (defined as the percentage of CD4 cells in one’s blood).
To conduct the analyses, we used a secondary de-identified patient data set from a multisite HIV clinic in Pennsylvania that serves patients in both rural and urban areas. To treat patients across this large geographical area, the main clinic operates seven satellite clinics that use the same medical record database. For the purpose of this analysis, sites were classified as being in urban or rural settings.
Sample Characteristics
The study data set included de-identified records of 704 patients diagnosed with HIV. Data were extracted from the clinic database based on those who received medical services at the HIV clinic and its satellite sites between January 2010 and March 2016. The data set included demographic information and quarterly health and service variables for each patient for visits from January 2012 through March 2016 for a total of 17 time points. The number of eligible participants in the data set increased over the study period as new patients enrolled (see Table 1) and, because this was a retrospective study, there was no attrition.
Number of Eligible Participants in the Data Set by Year.
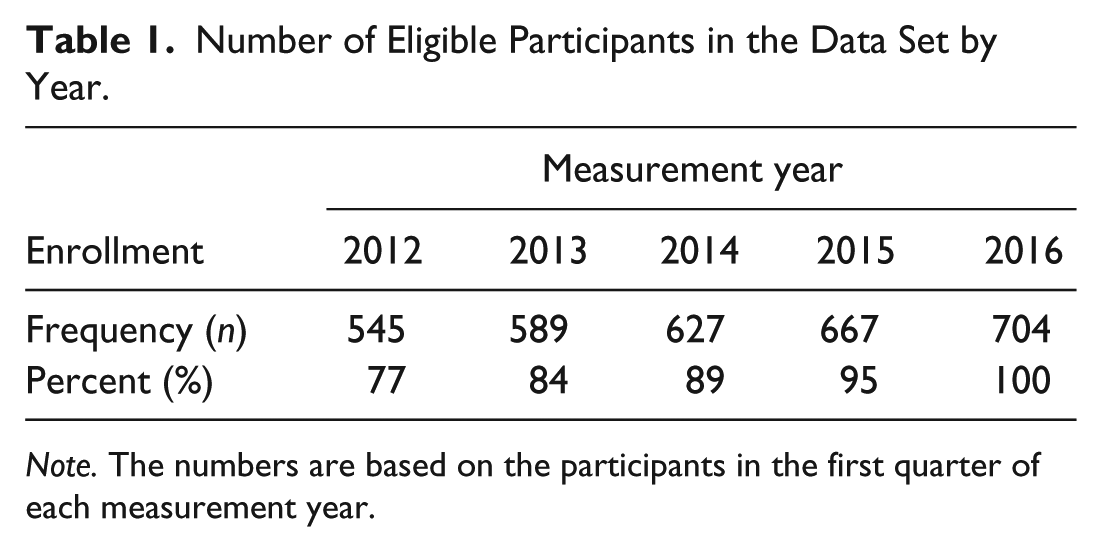
Note. The numbers are based on the participants in the first quarter of each measurement year.
The selection criteria included patients with an HIV diagnosis, who were at least 18 years old as of January 2010, who remained alive throughout the study period, and who were not incarcerated. Children and youth were excluded because they may not have been enrolled in HIV medical care or CM voluntarily. Because our primary environmental factor is CM services, and incarceration and death would preclude the services, these individuals were excluded from the current analysis. For a more detailed description of sample characteristics, please see Table 2.
Baseline Demographic Information (N = 704).
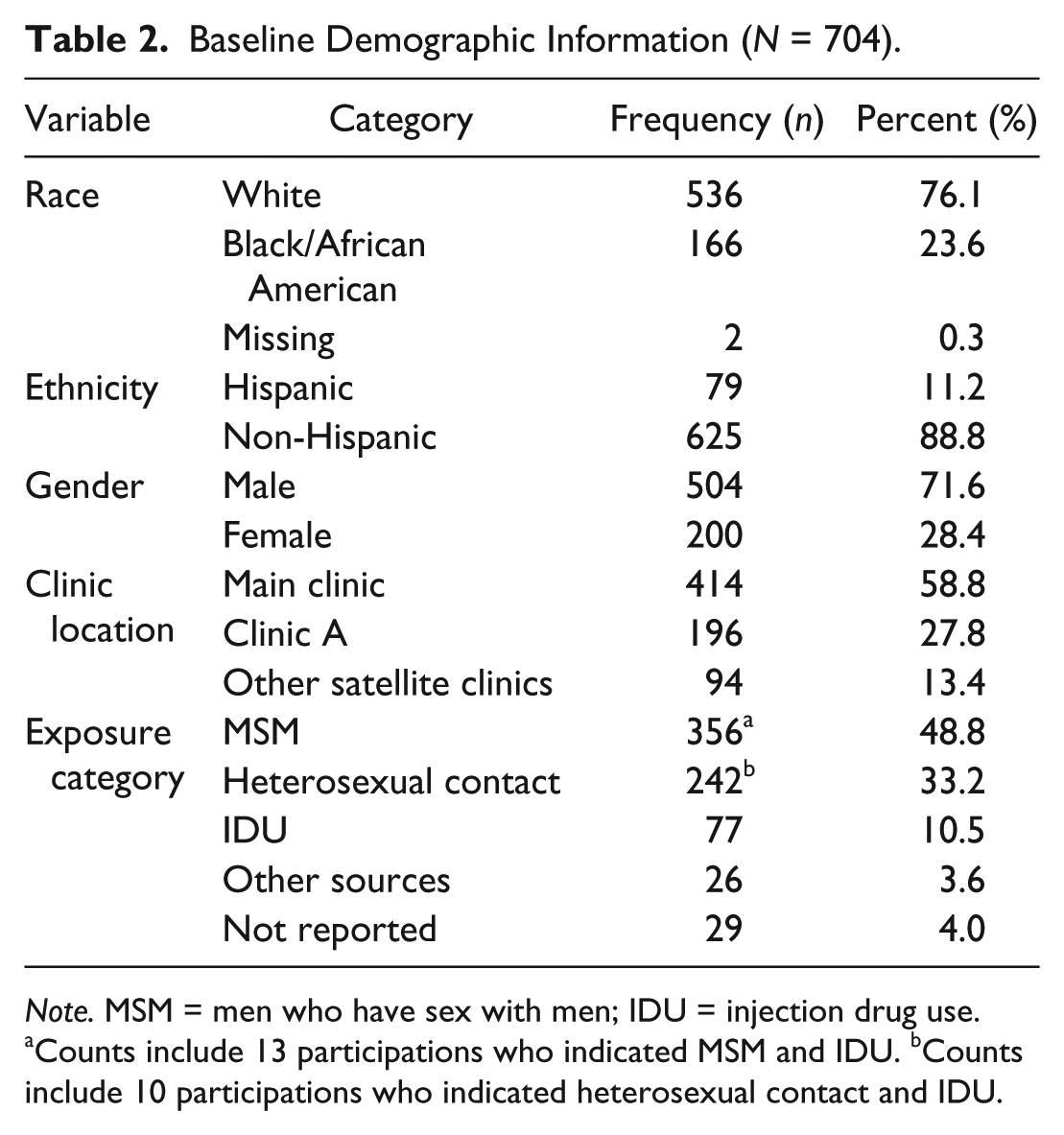
Note. MSM = men who have sex with men; IDU = injection drug use.
Counts include 13 participations who indicated MSM and IDU. bCounts include 10 participations who indicated heterosexual contact and IDU.
The repeated-measures dichotomous time-varying variables at the beginning and conclusion of the study period are presented in Table 3. Each variable represented the patient status in the previous 3 months. The percent of individuals who used CM during the previous 3 months gradually increased over time, from 17.6% (n = 96) using CM in the first quarter of 2012 to 36.4% (n = 256) in the first quarter of 2016. This finding shows that the majority of the sample did not use CM services consistently across the 5-year period. The CM variable used in analyses herein indicates whether a subject used such services within a 3-month calendar quarter.
Descriptive Statistics of Categorical Time-Varying Variables (N = 704).
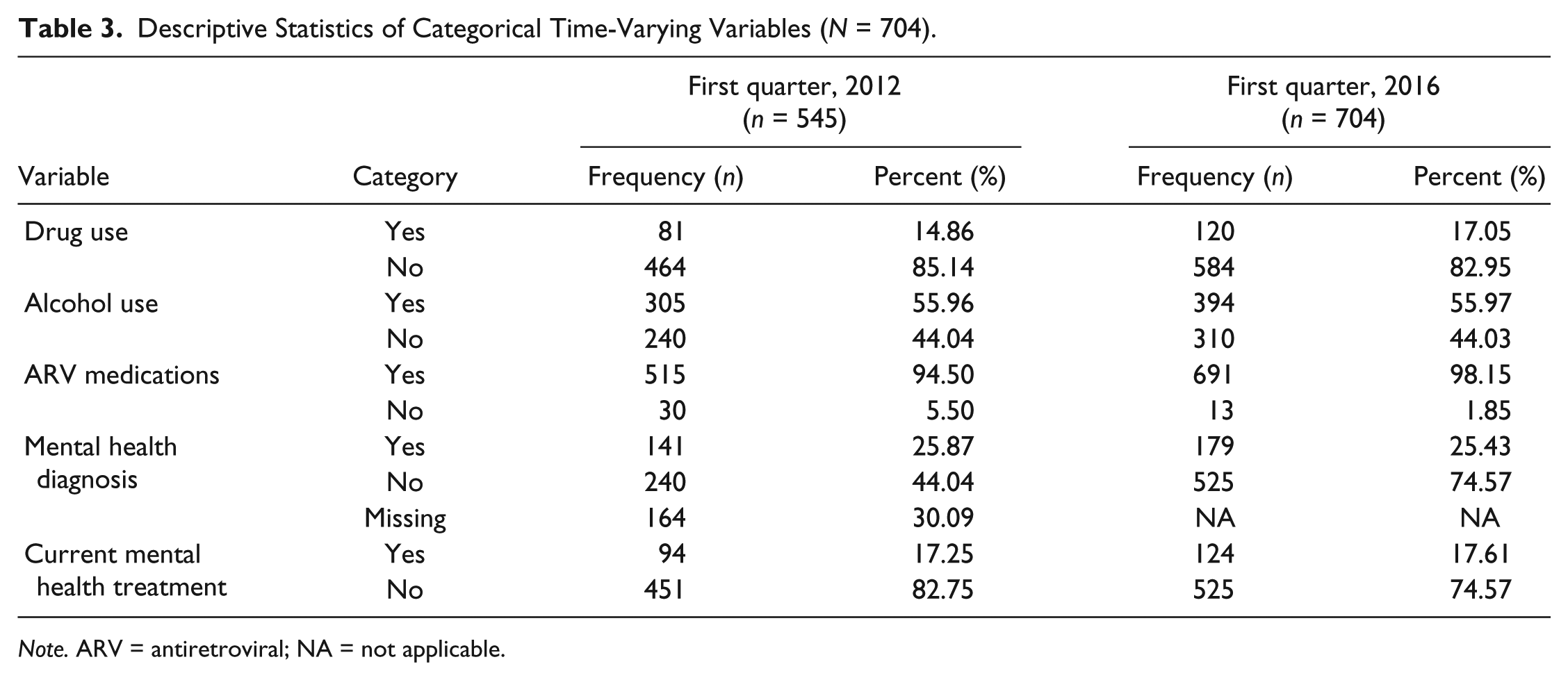
Note. ARV = antiretroviral; NA = not applicable.
Data Analyses
In this longitudinal analysis, a generalized estimated equations (GEE) model was used to model retention in care and a repeated-measures general linear mixed (GLM) model was used to analyze biological health outcome (CD4%). Both analyses used an autoregressive covariance structure to model the correlation of responses over time. Analyses were conducted in SAS/STAT® software, v13.1 (Copyright, 2013). Both models were fit with a backward elimination approach in which insignificant terms were removed one at a time until the best fitting model was obtained. Many participants did not report their mental health treatment, mental health diagnosis, drug use, and alcohol use at each time point (see Table 3). During CM, fields were primarily updated when a change in status was noted, according to the case manager. To account for these missing data, the last observation carried forward (LOCF) approach was used to impute a current observation based on the most recently recorded measurement (Cao, Li, & Fine, 2016).
Results
Retention in Care Outcomes
After controlling for correlated outcome data and other covariates within the GEE model (see Table 4), participants who did not use CM during the previous 3 months were 60% more likely, on the odds scale (95% confidence interval [CI] = [1.45, 1.76], p < .001), to remain in care, compared with those who did use CM during the previous 3 months. The odds that an individual on ARV medications during the previous 3 months remained in care were 5.28 times greater than for someone not on ARV medication during the previous 3 months (95% CI = [4.39, 6.35], p < .001). Women were 24% more likely, on the odds scale, to remain in care than men (95% CI = [1.03, 1.49], p = .026) and Whites were 36% more likely, on the odds scale, to remain in care than non-Whites (95% CI = [1.14, 1.62], p < .001). Those who reported alcohol activity during the previous 3 months were 58% more likely, on the odds scale, to remain in care, than those with no reported alcohol use during the previous 3 months (95% CI = [1.40, 1.79], p < .001). The odds that an individual without a mental health diagnosis remains in care were 50% greater than those for an individual with a mental health diagnosis (95% CI = [1.28, 1.79], p < .001). Age is a continuous variable that was positively associated with retention in care; for 1-year increase in age, the odds of remaining in care increased by 2% and for 10 years increase in age, odds increased by 24% (p < .001). The results indicated no significant effect on retention in care due to clinic location (p = .330), ethnicity (p = .832), treatment (p = .253), and drug use (p = .3256).
GEE Results for Retention in Care Outcome.
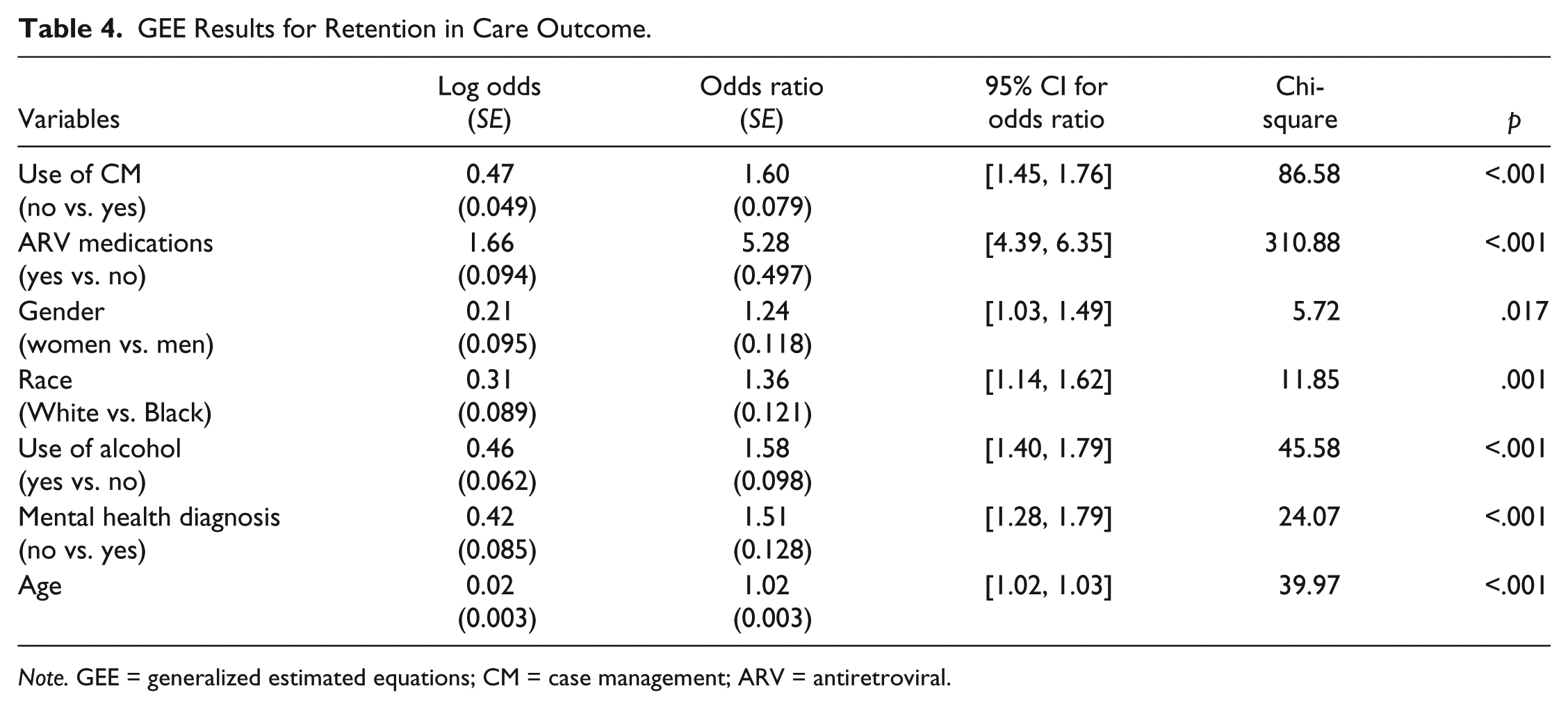
Note. GEE = generalized estimated equations; CM = case management; ARV = antiretroviral.
Immune System Health Outcome
Participants who had a medical appointment during the previous 6 months have a significantly higher mean CD4% than those who did not remain in care (p < .001). Participants who are White (p < .001), women (p = .003), non-Hispanic (p = .001), who did not receive CM services in the previous 3 months (p = .01), who did not receive mental health treatment in the previous 3 months (p = .036), or who used ARV medication during the previous 3 months (p < .001) also had a significantly higher mean CD4% over time (see Table 5). Age (p = .331), mental health diagnosis (p = .145), drug (p = .289) or alcohol (p = .451) use, or clinic setting (p = .119) had no significant effect on the mean CD%.
Least Squares Means of the Mixed Model for CD4%.
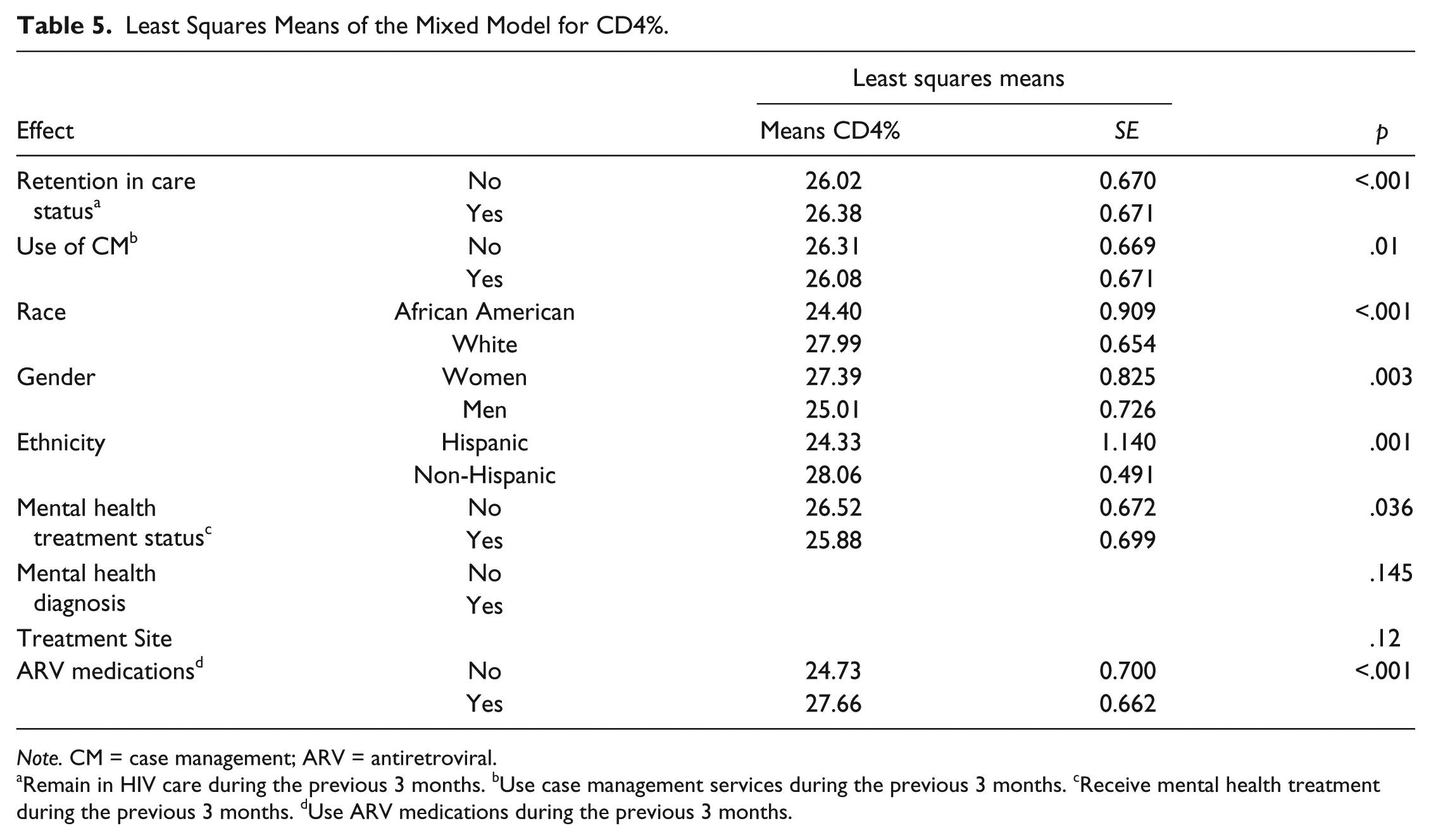
Note. CM = case management; ARV = antiretroviral.
Remain in HIV care during the previous 3 months. bUse case management services during the previous 3 months. cReceive mental health treatment during the previous 3 months. dUse ARV medications during the previous 3 months.
Discussion
This study applied the ICF to conceptualize the impact of personal and environmental factors on PLWH’s retention in care and immune system health (CD4%) outcomes. Each factor that was associated with these outcomes is discussed in greater detail below along with implications for rehabilitation counselors and educators.
Environmental Factors Associated With Retention and Health Outcomes
Contrary to our initial hypotheses, individuals who did not use CM services within the quarterly assessment period were more likely to remain in care. In addition, clinical setting was not associated with either retention in care or immune system health outcome.
Use of CM services
Based on previous research findings indicating that use of CM was associated with retention in care outcomes (Brennan-Ing et al., 2016; Craw et al., 2008), we hypothesized that participants who used CM would be more likely to remain in care. The results of this study, however, indicate that use of CM was negatively associated with PLWH’s retention in care status; that is, individuals who had not used CM during the past 3 months were more likely to remain in care. Upon reflection, it appears that our longitudinal study design, which examined intermittent use of CM services among the same population over time could help account for our results being different from previous research studies. Unlike other studies, that either compared the outcomes between different populations such as CM-funded organizations and non-CM-funded organizations (Willis et al., 2013) or participants who used CM services to a control/comparison group of participants who either (a) did not use CM at all (Craw et al., 2008; Metsch et al., 2015) or (b) used a different type of CM service (Brennan-Ing et al., 2016), our study measured the intermittent use of CM by the same population over time. Because our study focuses on fluctuations in CM use, it is likely that our participants would use CM services primarily at points in their lives where they encountered significant challenges and that these challenges would also increase their vulnerability to loss to care.
It makes sense that during these times of CM need, our participants would also be at heightened levels of vulnerability and potential loss to care, which underscores the unique context of providing CM for individuals with intermittent disabilities. Any kind of significant life change such as loss of employment or decrease in health can precipitate risk of loss to care and increase the actual loss to care without rapid intervention. Johnson, Polansky, Matosky, and Teti (2010) conducted a study to identify psychosocial factors relating use of publicly funded CM services among PLWH who did not have primary medical care, and found that individuals who request basic services (e.g., transportation and food) were more likely to use CM services than those who did not use these services. This finding underscores that those who use CM services face more significant barriers to care than patients who did not need CM. Similar to the retention in care outcome, we found that PLWH who did not receive CM services during the previous 3 months had significant higher gain in CD4%, meaning they achieved better health outcomes. However, the difference in CD4% was only 0.23 percentage points, which may be too small to be practically significant. The relatively small difference in outcomes in CD4%, despite the greater level of challenges that participants using CM services likely encountered, highlights the potential role that CM services may have on minimizing negative health outcomes during periods of increased threats to loss to care.
Clinic location
Geographic location and context is known to play a key role influencing the extent to which PLWH engage in care (Cesnales, 2012). However, this study did not demonstrate significant differences in either retention in care or immune system health outcomes between PLWH who received HIV treatment at urban sites and those who received treatment at rural sites. One explanation for this outcome in our study is that most of the physicians and nurses at the main site also travel to rural sites to provide services on a regular basis. Within this service delivery model, the quality of the care is more uniform, which helps to explain the lack of expected differences among urban and rural treatment sites in our study.
Personal Factors Associated With Retention and Health Outcomes
Personal factors that were significantly associated with retention in care status were use of ARV medications, gender, race, use of alcohol, mental health diagnosis, and age. With respect to immune system health outcomes, factors that were significantly associated with an increase in CD4% were retention in care status, race, ethnicity, gender, use of ARV medications, and mental health treatment status. We discuss each of these factors in greater detail below.
Race and ethnicity
Racial and ethnic disparities often contribute to health inequities due to structural barriers, including perceived and objective discrimination. Research indicates that racial and ethnic minorities living with HIV are less likely to access ARV medications, to adhere to ARV medications, and to achieve viral suppression (Pence, 2009; Silverberg et al., 2009). In light of this, it makes sense that, in the current study, both race and ethnicity were significant predictors associated with gains in CD4%. More specifically, participants who were White and non-Hispanic achieved more gains in CD4% than racial and ethnic minorities on average. This finding is consistent with Weintrob and colleagues’ (2009) study, which found that African Americans were less likely to achieve viral suppression, even with equal access to ARV medications. ARV treatment adherence is often a critical issue among racial and ethnic minorities living with HIV, associated with medical mistrust (i.e., provider, medical system, and treatment mistrust), discrimination, and other psychosocial factors (Bogart, Wagner, Galvan, & Klein, 2010; Dale, Bogart, Wagner, Galvan, & Klein, 2016). Our findings underscore the need for additional research and services for the most vulnerable populations. To address this need, the updated NHAS (Office of National AIDS Policy of the Obama White House, 2015) specifically recommends (a) expansion of services to young Black gay and bisexual men, Black females, and those who live in the South; and (b) integration of services and research that focus on evidence-based approaches to address HIV-related health disparities.
Gender
The results of our study indicate that, on average, women had more gains in CD4% than men; and, women were also more likely to remain in care. Fleishman et al. (2012) found that successful establishment in HIV treatment was more likely to happen for women than men. Research has identified gender differences in help-seeking behaviors; for example, Tedstone Doherty and Kartalova-O’Doherty (2010) found that women were more likely to seek help from general health practitioners compared with men. Several studies have found that among those who received antiretroviral therapy (ART) treatment, women were more likely to achieve viral suppression (Kipp et al., 2010). Possible explanations for better health outcomes among women include higher plasma concentrations of ARV medications in women compared with men (Cressey & Lallemant, 2007; Umeh & Currier, 2006) and less alcohol consumption among women, as use of alcohol has a negative impact on ART treatment outcomes and medication adherence (Rebeiro et al., 2013).
Age
The results of our study show that older participants were more likely to remain in treatment, although there is no statistically significant effect on gains in CD4% related to age. Our findings are consistent with other studies that found that older PLWH were more likely to use HIV medical services (Craw et al., 2008; Fleishman et al., 2005) and to achieve higher retention rates (Rebeiro et al., 2013); younger people were more likely to drop out of treatment (Ulett et al., 2009). Fleishman et al. (2012) noted that older adults were more likely to remain in care because they have more experience navigating the health care systems and have greater sense of responsibility. However, research suggests that adolescents and young adults often experience more risks of falling out of care due to unstable life conditions, immaturity, and other challenges (Craw et al., 2008). In a qualitative study, Fortenberry, Martinez, Rudy, and Monte (2012) found that many barriers to linkage to care for newly diagnosed HIV-positive youth were structural (e.g., available linkage services, transportation, health insurance, and youth friendly services), rather than youth characteristics. Researchers have also noted that psychosocial services such as counseling services (Naar-King et al., 2007) and CM services (Fortenberry et al., 2012) were critical in helping youth living with HIV link to and remain in treatment. These findings highlight the importance of designing youth-specific services to increase the potential effectiveness of prevention and treatment outcomes among youth living with HIV.
Use of ARV medications
Use of ARV medication was significantly associated with both retention in care and immune system health outcomes in this study. Use of ARV medication is a critical indicator of access to HIV care as one has to engage in medical treatment to have access to ARV medications. National data from the North American AIDS Cohort Collaboration on Research and Design suggested that receipt of ARV medications at baseline increased the probability of retention in care over time (Rebeiro et al., 2013). That use of ARV medications was also significantly associated with positive gain in CD4% in this study is not surprising, given that the main function of ARV medications is to improve immune functioning. Similarly, that retention in care status was associated with significant gains in CD4% was also expected, given the wealth of research that demonstrates the effect of retention in care on health outcomes (Fleishman et al., 2012; MacKellar et al., 2010; Mugavero et al., 2012; Yehia et al., 2014). Our finding underscores the need for ongoing funding of ARV medications and the key role that Ryan White Care Act plays, as a major source of funding for HIV medical care, in contributing to improved health and HIV prevention outcomes.
Mental health and substance use
Overall, this study was limited in its capacity to contribute to research related to the association between health outcomes and mental health concerns (including mental health diagnosis, mental health treatment, use of alcohol, and use of drugs). Our study indicates that individuals who had a formal mental health diagnosis and who were in mental health treatment had poorer health outcomes (decreased odds of remaining in care and had lower gains in CD4%). Given the longitudinal research design and the intermittent nature of mental health, it is possible that receipt of mental health treatment during any quarter of data collection is a reflection of increased severity of the mental illness symptoms at that point in time. In this current study, we were not able to compare the effect of mental health treatment on PLWH’s health outcomes as many participants received mental health treatment intermittently. That PLWH who are experiencing greater mental health concerns have poorer health outcomes is consistent with previous studies that identified the negative impact of mental health diagnosis and substance abuse disorders on biological outcomes with decreased ARV treatment adherence and higher mortality rates (DeLorenze, Weisner, Tsai, Satre, & Quesenberry, 2011; Stoff, Mitnick, & Kalichman, 2004).
Our study did not demonstrate a significant association between drug use and retention in care or changes in CD4%, which is inconsistent with previous research that found that PLWH who use injection drugs were less likely to remain in care and to achieve optimal treatment outcomes (Giodano et al., 2015). With respect to alcohol use, we found that participants who reported use of alcohol were more likely to remain in care, whereas alcohol use was not significantly associated with immune system health outcomes. One potential reason why use of alcohol was associated with health outcomes whereas use of drug was not could be because of the percentage of participants who reported substance use in each of these categories. Approximately half of the participants reported alcohol use (55.97%), whereas the percentage of those who reported drug use was relatively low during the same time period (17.05%). This could be because that alcohol use is not illegal and a common social practice. It would be more informative if we could have compared the different level of alcohol use and their retention in care status, as heavy alcohol use is also known to be associated with biological and behavioral changes related to disease progression (Hahn & Samet, 2010). In addition, previous research indicates that retention and health outcomes can vary depending upon the type of substances being abused and the nature of the abuse (Mugavero et al., 2009; Rebeiro et al., 2013). Unfortunately, our study did not capture this level of detail regarding the level of alcohol use and type of substance use and more research is needed to better understand these relationships.
Limitations
Because the study sample was drawn from a single multisite clinic in Pennsylvania, our findings should not be generalized to other PLWH populations. Furthermore, because our study is an observational retrospective study using an existing data set, PLWH were not randomly assigned into CM services, no causal inferences can be made. As an exploratory study, this study primarily focused on use of CM services over time as documented in the patient database. It could be possible that some patients may have received services elsewhere that were not documented. To minimize this risk, the current clinic director confirmed that the data provided a good reflection of the patient population. In addition, the data set did not capture the intensity of CM services each individual used, which limits the depth of understanding related to any potential variation within the services provided. Although beyond the scope of the current study, it would be helpful for future studies to include a more comprehensive assessment of CM services to better assess whether different CM strategies or characteristics (e.g., intensity, integrated service team) could affect the key outcomes.
Another limitation is that individuals who were deceased and who were incarcerated during the study period were excluded from the current analysis. The baseline health status of these individuals could be highly related to environmental and personal factors (i.e., individuals who were deceased could be due to lack of CM services and poor retention in care status). For future research, researchers could focus on the association of environmental and personal factors and mortality using other longitudinal approaches. As discussed earlier, many participants did not report their mental health diagnosis, mental health treatment status, and drug and alcohol use status consistently. The missing data on these items could also be related to the higher levels of stigma associated with substance abuse and mental health issues. In addition, our data did not include formal substance abuse diagnoses as participants only reported whether they used alcohol or drugs and not the extent of alcohol or drug consumption. Future research in this area should include more systematic documentation of types of psychiatric treatments, including information on intensity of services and treatment adherence.
Implications for Rehabilitation Practice, Education, and Research
This study highlights the unique challenges of PLWH by addressing barriers to retention in care and optimal health outcomes related to the episodic nature of HIV. Implications for rehabilitation counselors, educators, and researchers are discussed.
Implications for Rehabilitation Counseling Practice
Rehabilitation counselors have a tremendous depth of knowledge and expertise in the medical, psychosocial, and vocational aspects of disability that can help PLWH reduce barriers, achieve optimal treatment outcomes, and enhance quality of life. Rehabilitation counselors are trained specifically to work with people with different types of disabilities across the life span, including physical disabilities, psychiatric disabilities, and chronic illness. Therefore, rehabilitation counselors can use their expertise to work with PLWH. In addition, conceptualizing client issues using the ICF framework is an important skill set of rehabilitation counselors, as psychosocial factors often affect the level of functioning and treatment outcomes among people with disabilities and chronic health conditions. Rehabilitation counselors can work with PLWH to identify personal and environmental factors that are associated with their treatment outcomes and to facilitate optimal changes. One study found that use of VR services was associated with positive public health outcomes for PLWH in terms of increased access to care and reduced health risk behaviors (Conyers & Boomer, 2014). Therefore, assisting PLWH to achieve employment goals is another area where rehabilitation counseling professionals can use their expertise to apply the ICF framework to identify PLWH’s barriers and facilitators to employment.
Rehabilitation counselor professionals can also serve as consultants and provide training related to disability stigma, policy, VR, and the medical and psychosocial aspects of chronic illness and HIV. For example, rehabilitation counselors could work with public health stakeholders to provide training related to psychosocial factors associated with intermittent disability, alcohol and substance abuse assessments, work-readiness assessments, and culturally sensitive counseling for staff within AIDS organizations. Making recommendations to expand access to rehabilitation and mental health services to policy makers could also be an area where rehabilitation professionals could contribute.
Implications for Rehabilitation Counselor Education
In light of the contributions that rehabilitation counseling professionals can provide to help address public health needs of PLWH, rehabilitation counselor educators can encourage students who are interested in working in the HIV field to become familiar with the service delivery system and how rehabilitation counselors can contribute to personal and public health outcomes. Given that specific coursework accreditation (e.g., Council for Accreditation of Counseling and Related Educational Programs [CACREP], 2016), ethical code (i.e., Commission on Rehabilitation Counselor Certification [CRCC], 2017), and certification (i.e., Rehabilitation Counselor Certification) require demonstration of multicultural sensitivity and expertise in both medical and psychosocial aspects of disability (including knowledge of chronic and episodic illness), it is important for rehabilitation counselor educators to address both the medical and psychosocial needs of the diverse cultural groups, including PLWH. As noted in this study’s results, rehabilitation educators will need to ensure coverage of the unique considerations when working with individuals with episodic disability and chronic illness (Koch & Rumrill, 2016).
In 2016, CACREP introduced a new specialty area of clinical rehabilitation counseling, which requires educators and students in clinical rehabilitation counseling programs to be familiar with rehabilitation services within the continuum of care. Students are required to understand the diverse rehabilitation service delivery systems, including CM systems, housing programs, mental health services, and VR systems (CACREP, 2016). Importantly, knowledge of employment and disability issues is a helpful asset when addressing the psychosocial needs of PLWH as public health research indicates that downward employment trajectories (e.g., those leading to loss of employment) are associated with increases in health risk behaviors (Liukkonen et al., 2009).
Implications for Rehabilitation Counseling Research
Given that HIV/AIDS is a relative new area in the field of rehabilitation counseling, more research is needed. It is important to investigate how personal and environmental factors affect PLWH’s health outcomes, so practitioners can better assist individuals to remove the barriers and to achieve optimal outcomes. For instance, examining the relationships between accessibility to HIV treatment and PLWH’s health outcomes in a range of different rural and urban geographic settings could help professionals understand how to reduce disparities in different contexts.
Conyers (2011) pointed out that HIV is categorized as an episodic disability as PLWH often experience fluctuation in health over time. For future research, it is critical to take the episodic nature of the illness into consideration and examine the impact of each factor on the long-term health trajectories, not only the overall outcomes. For example, additional research is needed to further assess the impact of the intermittent use of CM on health outcomes. Cohort studies using repeated-measure approaches could be useful in tracking the longitudinal outcome. Given that our study data set did not include variables on self-reported health perception and psychosocial needs, it would be important to include these factors in future research. Additional psychosocial variables should also be included in future studies. For example, Johnson et al. (2010) identified that insurance and housing status were associated with use of CM services. In addition, building employment-related items in intake and reassessment questionnaires could help researchers and practitioners better understand PLWH’s employment status and the impact on their health outcomes. Currently, many AIDS organizations do not provide on-site vocational services and do not assess PLWH’s employment status or needs across time. Incorporating vocational and other psychosocial variables into public health data sets can facilitate the collaboration between the fields of VR and public health.
Conclusion
This study was undertaken to fill the knowledge gap in the existing literature by applying the ICF to conceptualize the influences of personal and environmental factors on PLWH’s retention in care and immune system health outcomes. The results indicate that gender, race, ethnicity, age, use of ARV medications, use of alcohol, mental health diagnosis, and mental health treatment were significantly associated with these health outcomes. HIV-related health disparities often contribute to health inequities due to structural barriers and stigma. It is important for rehabilitation counselors to address these disparities and to facilitate access to quality treatment among vulnerable populations. Rehabilitation counselors and rehabilitation counselor educators can play important roles in helping to train the HIV workforce to facilitate optimal client and public health outcomes. Rehabilitation researchers, educators, and practitioners have a long history of evaluating, educating, and providing services for individuals with a wide range of episodic and emerging disabilities such as HIV, multiple sclerosis, and psychiatric disability (Conyers, in press; Koch & Rumrill, 2016; Vick, 2013). As such, the integration of rehabilitation models and practices into medical CM and initiatives to address the goals of the NHAS is recommended.
Footnotes
Acknowledgements
We would like to thank Dr. John Zurlo, medical director of the Department of Infectious Disease at Penn State Hershey Medical Center who provided the clinic data set and consultation for this study. Dr. Tonya Crook and Mr. Michael Witmer at the clinic also shared their rich clinical experiences that allowed us to interpret the study results in a practical way.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.