
Abstract
Sexual minority persons (i.e., lesbian, gay, bisexual, queer [LGBQ]) are at risk for developing chronic illness(es) and/or disabilities (CID); however, there is a dearth of information regarding the practices used by rehabilitation counselors working with this population. This modified grounded theory study aimed to understand the effective practices that rehabilitation counselors reported exhibiting when working with sexual minority persons living with CID. A total of 12 certified rehabilitation counselors were individually interviewed. Interviews were transcribed and recursively analyzed with a research team. Trustworthiness and credibility were ensured via in-depth member checking, researcher triangulation, and collection of rich descriptions from participants. A substantive model of rehabilitation counseling was constructed from the interviews, with Affirmative Intersectionality as the core category. Four supporting categories were also constructed, including professional attributes, alliance, intersectional sensitivity, and intersectional interventions. Details regarding the model are provided, as well as discussion on educational and supervision implications, study’s limitations, and future research implications.
Intersectionality is a framework that considers the experience of possessing multiple intersecting identities, as well as any socially reinforced advantages and disadvantages associated with multiple group membership (Cole, 2009). Although intersecting identities can create opportunities of privilege (e.g., being a White man or a physically able bodied woman), there also exist instances of oppression that might exacerbate the experience of stigma for an individual with multiple marginalized identities (Parent, DeBlaere, & Moradi, 2013; Warner & Shields, 2013). Invisible identities, such as sexual minority identity (i.e., lesbian, gay, bisexual, queer [LGBQ]), must also be considered within the intersectionality framework (Balkin, Watts, & Ali, 2014; Bernert, Ding, & Hoban, 2012; Purdie-Vaughns & Eibach, 2008), especially as LGBQ identity can intersect with other identities that shape the development of certain psychosocial experiences (Babbitt, 2013; Chen, Androsiglio, & Ng, 2010). In particular, one combination that has received sparing attention in the rehabilitation counseling literature is the intersection of sexual minority identity and identifying as having one or more chronic illnesses and/or disabilities (CID; Centers for Disease Control and Prevention [CDC], 2011; Harley, Hall, & Savage, 2000; Harley, Nowak, Gassaway, & Savage, 2002).
Despite the longtime awareness of these intersecting identities in the counseling, psychological, and disability literature (American Psychological Association [APA], 2012a, 2012b; Fine & Asch, 1988; Greene, 2007, 2000), sexual minorities are at significant risk for experiencing psychological and behavioral health-related disparities, such as anxiety, depression, substance use disorders, smoking, and suicidal behaviors (Cochran, 2001; Poteat, Aragon, Espelage, & Koenig, 2009). In addition, sexual minorities are more likely to report physical health-related disparities, such as activity limitations, asthma, risk for cardiovascular disease, as well as being overweight and obese (Cochran & Mays, 2007; Conron, Mimiaga, & Landers, 2010). Using CDC population data and the Behavior Risk Factor Surveillance System (BRFSS) from the state of Washington, Fredriksen-Goldsen, Kim, and Barkan (2012) embarked upon a study to understand disability-related prevalence rates among sexual minorities. They concluded that the prevalence of disability was significantly higher among sexual minority adults and that they were significantly younger when compared with heterosexuals. Consistent with other reports (e.g., Cochran, 2001; Cochran & Mays, 2007; Conron et al., 2010), Fredriksen-Goldsen et al. (2012) also found that sexual minorities were more likely to experience health disparities such as arthritis, obesity, poor physical health, HIV, and frequent mental distress.
The significant discrepancies of health-related disparities are found not only among sexual minority adults but also among sexual minority youth (Duke, 2011). With a sample of more than 18,000 adolescents living in the United States, Cheng and Udry (2002) calculated that boys living with physical disabilities were 4.8 times more likely to report a same-sex attraction, while girls living with physical disabilities were 4.5 times more likely to report a same-sex attraction when compared with their counterparts not living with physical disabilities. In another study among college students living with CIDs (e.g., attention-deficit/hyperactivity disorder [ADHD], learning, sensory, mobility, psychiatric, and speech/language disabilities), Bernert et al. (2012) reported that approximately 1,276 gay and lesbian identified young adults were living with one or more CID, while approximately 1,147 bisexual identified individuals were living with one or more CID conditions. Although majority of the sample identified as heterosexual, the percentage of students living with CID who identified as gay/lesbian (24.2%) or as bisexual (34.2%) were significantly higher than students who were heterosexual identified (16.1%).
As persons living with CID already receive fewer preventive health services, sexual minorities living with a CID may be at danger of experiencing multiple health risks due to the lack of adequate health care services that are also afforded to sexual minorities (Fredriksen-Goldsen et al., 2012). Disparities also exist in the workforce, as both sexual minorities and persons living with CID are at higher risk for lower wages, being underemployed or unemployed, and more likely to experience workplace violence and discrimination (Fassinger, 2008; Houtenville, Sevak, O’Neill, & Cardoso, 2014). It is likely that health- and employment-related disparities endured by sexual minorities living with CID are partially the combined result of societal stigma, historical and institutional discrimination, as well as the psychological stress of oppression, such as internalized heterosexism and ableism (Conyers, Smal, & Chiu, 2014; Fassinger, 2008; Meyer, 2003).
Deficient knowledge regarding sexual minorities living with CID poses significant implications for rehabilitation counselors, especially as they are expected to ethically address issues of cultural diversity and CID (Commission on Rehabilitation Counselor Certification [CRCC], 2010). Rehabilitation counselors are trained to consider both multicultural and identity-related factors in the rehabilitation and vocational counseling process and are challenged to consider innovative ways of serving diverse persons living with CID (Gilbride & Stensrud, 2003; Millington, 2012; Sue & Sue, 2008). Despite the existence of guidelines and competency standards regarding counseling and assessment practices with sexual minorities (APA, 2012b; Association for Lesbian, Gay, Bisexual, and Transgender Issues in Counseling [ALGBTIC], 2012), sexual-minority-related issues have been considerably neglected in the rehabilitation counseling literature (Harley et al., 2000; Harley et al., 2002; Hunt, Matthews, Milsom, & Lammel, 2006). Furthermore, a significant number of certified rehabilitation counselors fail to receive adequate training regarding sexuality-related issues (Kazukauskas & Lam, 2009), which calls into question the current state of affirmative practices used by certified rehabilitation counselors working with sexual minorities living with CID.
Guidelines that have been established by ALGBTIC (2012) and APA (2012b) encourage practitioners and scholars to engage in affirmative practices with sexual minorities. Affirmative practice with sexual minorities includes exercising appropriate ethical mandates by one’s respective profession (e.g., CRCC, APA), being aware of one’s own worldviews, values, and suspending any biases and judgments (Constantine, Hage, Kindaichi, & Bryant, 2007; Greene, 2007; Israel, Gorcheva, Walther, Sulzner, & Cohen, 2008). In addition to professional character traits, practitioners must never assume that any of their clients are heterosexual. According to Matthews (2007), when practitioners assume heterosexuality, they “reinforce the marginality that LGB clients experience and add turmoil to the therapy process by forcing clients to either keep an important secret or take a significant risk in raising the issue of sexual orientation” (p. 203).
Affirmative practice is also extended to persons living with CID, with one of the most notable approaches being disability affirmative therapy (DAT; Olkin, 2001). Practitioners of DAT use an affirmative systemic approach when addressing societal barriers, empowerment, coping, and disability adaptation. Although not overtly described as a form of affirmative practice, Smart and Smart (2006) proposed several recommendations for counselors working with persons living with CID that could be implied as affirmative. Their approach encompasses the need for practitioners not to impose personal values and beliefs, diffusing power differentials, not making assumptions about certain client experiences, and acknowledging multiple identities (Smart & Smart, 2006). A review of the literature suggests that an integration of affirmative practices with both groups can take place and be holistically applied to sexual minorities living with CID.
Present Study
Given the reported rates of CID and other health-related disparities among sexual minorities (Cochran, 2001; Fredriksen-Goldsen et al., 2012), relevant psychosocial experiences of both sexual minorities and persons living with CID (e.g., discrimination, stigma, minority stress; Conyers et al., 2014; Houtenville et al., 2014, Meyer, 2003), and literature concerning affirmative practice (Greene, 2007; Matthews, 2007; Olkin, 2001; Smart & Smart, 2006), there remains a lack of data regarding the counseling practices used by rehabilitation counselors with this population. Whereas some scholars have provided important conceptual contributions to rehabilitation counseling with sexual minorities living with CID (Harley et al., 2000; Harley et al., 2002), the objective of this study was to develop a substantive model, grounded in data, that outlined specific practices that rehabilitation counselors considered effective when working with sexual minorities living with CID. The research inquiry guiding this study was as follows:
Method
Participants
Pseudonyms, individual ages, cisgender identity, sexual orientation, race/ethnicity, primary work setting during the time of the interviews, and primary CID conditions that participants reported working with are displayed in Table 1. Geographically, all participants came from the United States, including the Northeast (n = 2), Mid-Atlantic (n = 2), Southeast (n = 6), Midwest (n = 1), and West coast (n = 1). All participants possessed certifications as rehabilitation counselors and master’s degrees from Council on Rehabilitation Education (CORE)–accredited programs. In addition, in conjunction with a master’s degree, one participant had an educational specialist degree, one participant received a second master’s degree in social work, and two participants possessed doctoral degrees.
Demographic Information for all Study Participants (N = 12).

Note. CID = chronic illness(es) and/or disabilities; VA = Veteran’s Affairs.
Participants reported having an average of 9.33 years (SD = 5.10, range = 5–23 years) of experience providing rehabilitation counseling services to sexual and gender minorities. Given that the Department of Labor (2014) has reported the diverse workplace settings in which rehabilitation counselors are employed, it was essential to sample rehabilitation counselors from a variety of rehabilitation counseling settings. Participants reported providing (and having experience providing) services, such as vocational rehabilitation (VR) counseling, vocational placement, job coaching, clinical mental health counseling, academic counseling, appraisal and testing, crisis interventions, case management, family and couples counseling, as well as supervision and training.
Research Methodology
Given the scarcity of data on the topic, a qualitative research methodology was used. Qualitative methodologies are especially suitable when addressing counseling processes (Morrow, 2007) and multicultural counseling issues (Atkinson, Bui, & Mori, 2001), and when developing contextualized counseling approaches and models from the experiences of practicing counselors and psychotherapists (Fragkiadaki & Strauss, 2012; Oddli & Halvorsen, 2014). Similar to Noonan et al. (2004), a modified grounded theory (GT) methodology (Charmaz, 2006; Strauss & Corbin, 1998) was used to guide the study and to develop a substantive model that could be used by rehabilitation counselors working in diverse practice settings. Modifications consisted of using a smaller sample size than is typical with GT studies, relying primarily on one form of data collection (i.e., interviews), and administering the same semi-structured interview protocol to all participants. Constructivism was both the epistemological and the theoretical perspective that informed the GT methodology of this study. Consistent with Charmaz’s (2006) perspective on constructivism and GT, (a) data were viewed as value-laden perspectives created by the social interactions of rehabilitation counselors, (b) analyses were viewed as social-based constructions, and (c) the constructed model was viewed as a plausible account of rehabilitation counseling practice with this particular population rather than an objective-based claim.
Researcher as instrument
Research team members (n = 7) identified as cisgender women (n = 4), cisgender men (n = 3), heterosexual (n = 4), gay (n = 2), and queer (n = 1). Concerning racial/ethnic identification, research team members identified as White/European American (n = 4), biracial (n = 2), and African American (n = 1). All research team members were born U.S. citizens, and raised in the southeast United States (n = 6) and the northeast United States (n = 1). Regarding educational backgrounds, research team members were either completing graduate degrees (n = 6) or possessed a master’s in rehabilitation counseling and doctorate in counseling psychology (n = 1).
Research team members reflectively documented, discussed, and bracketed any personal biases, dispositions, and assumptions throughout data collection and analyses (Lincoln & Guba, 2000). The following themes were identified and discussed throughout the extent of the study, as research team members exposed and processed their (a) feelings toward sexual stigma, ableism, and other forms of discrimination toward diverse sexual minority persons; (b) beliefs on how religious, family, and cultural systems reinforced certain forms of oppression in U.S. society; (c) etic and emic viewpoints in relation to sexual minority populations, CID, and being a counseling professional; (d) ethnic, cultural, sexual, and gender identities; (e) personality and cultural factors that could influence their interviewing and analyzing abilities; (f) beliefs on what constituted effective affirmative rehabilitation counseling practice with sexual minority persons; (g) diverse rehabilitation counseling practices; and (h) identification as sexual and gender minority persons and allies. In addition, there were several conversations to facilitate the diffusion of power dynamics between the principal investigator (the primary author) and the research team members.
Interview protocol
A semi-structured interview protocol was created for this study (refer to the appendix for the protocol). The content of the interview protocol was constructed by members of the research team and reviewed by two certified rehabilitation counselors (not interviewed for this study) who possessed more than 15 years of experience in multicultural and diversity issues. Personal demographic information, such as age, identified gender, sexual orientation, and CID status, was collected from each participant. In addition, data regarding current and previous work experiences, education and training, years as a rehabilitation counselor, and possession of any certifications and licenses were gathered. The same semi-structured interview protocol was used with each interviewed participant; however, follow-up probes differed depending on the responses participants gave. Follow-up probes allowed for a collection of in-depth and rich data regarding the phenomenon under inquiry, and allowed us to capture nuances among the differing experiences of our participants.
Procedures
An Institutional Review Board at a large urban university located in the southeast United States approved all procedures. As a goal of qualitative research is to understand the richness of experiences under inquiry, a criterion-based/maximum variation sampling procedure was adopted (Fassinger, 2005). This purposeful and gradual sampling procedure allowed for the selection of heterogeneous cases to gain information-rich and diverse experiences from the research participants (Morrow & Smith, 2000). In particular, a chain sampling procedure was used (Charmaz, 2006), with the primary author utilizing professional contacts to find the first few volunteers. In addition, requests for participating were sent to professional counseling listservs.
Although there is no agreed upon number on how many participants should be used when employing qualitative research design, the recommendation is to collect as many cases until no new information emerges or there is redundancy in the data (Fassinger, 2005; Morrow & Smith, 2000). Redundancy, or theoretical saturation (Gordon-Finlayson, 2010), can be achieved either by having multiple interviews with the same participants or with a group of 8 to 15 participants in a study (Morrow & Smith, 2000). Upon consensus of the research team, saturation was reached at 10 participants. To confirm that theoretical saturation was met (Johnston et al., 2010), 2 additional participants were added.
Eligibility standards were established prior to data collection and required participants to (a) be certified rehabilitation counselors, (b) have a minimum of 5 years post-master’s experience in the counseling field, (c) have experience providing rehabilitation counseling services to sexual and gender minority persons, and (d) express interest, expertise, and training with multicultural issues in the field of rehabilitation counseling.
Those who expressed interest in participating were provided the informed consent form via email, and verbal consent was accepted over the phone. Participants were engaged in semi-structured focused interviews that lasted anywhere between 60 and 120 min. Ten interviews were conducted over the phone by three separate research team members, while two were completed face-to-face by the first author. All interviews were audio recorded. After each interview, members of the research team debriefed any biases, concerns, or thoughts pertaining to the interview and discussed any themes. Members of the research team then transcribed each interview verbatim, and copies of interview transcripts were emailed to each of the participants. Participants were also asked to provide any corrections or clarifications upon reviewing the transcripts (n = 2 provided textual corrections). No further clarifying responses were provided by participants.
Data analysis
Data collection and analysis took place simultaneously and lasted approximately 12 months. Utilizing a constant comparative method, the research team compared themes and concepts across incidents, cases, and participants (Gordon-Finlayson, 2010). GT specifically employs the use of a three-level thematic coding process: open coding, axial coding, and selective coding (Strauss & Corbin, 1998). The initial coding process, open coding, focused on specific concepts and themes that emerged line-by-line from the first two transcribed interviews. All members of the research team coded the two interviews independently and then came together to discuss the codes. During our meeting, research team member agreement was necessary to apply the code to the data. After this, we generated the initial coding manual that reflected the relationships among the codes.
Given that the coding process requires that the researchers constantly compare concepts and themes across the interviews, the research team then proceeded to engage in axial coding. During this phase, the research team began identifying salient categories (Fassinger, 2005; Gordon-Finlayson, 2010). Research team members continued to individually code each interview and then gathered in a group to discuss their findings. Again, research team member agreement was necessary to apply the codes. The coding manual was slightly amended after each research meeting to reflect any changes in the identification of concepts. Members of the research team then engaged in selective coding, which required the construction of a core category and finalizing the coding manual (Holton, 2007). Members of the research team then proceeded to recode all 12 interviews with the finalized coding manual, core category, and respective subcategories.
Trustworthiness and credibility
Trustworthiness of the data was ensured via iterative questioning throughout the interview process, collecting rich descriptions from participants, frequent debriefing sessions before and after interviews, as well as reflective and analytic notes (i.e., memos) by research team members (Shenton, 2004). Trustworthiness was further established by triangulating across researchers—that is, utilizing several different members during the analysis process (Lincoln & Guba, 2000). In addition, negative case analysis was used by intentionally finding contradictions in the major findings for purposes of code and model refinement (Morse, 2007). As major themes were constructed from the data, research team members would review the narratives of all participants to see how their experiences fit or vary within the developing themes (Morrow & Smith, 2000). For instance, several participants reported disclosing their sexual orientation and CID status to clients as part of building an affirmative working alliance. During interviews and analysis, members of the research team intentionally looked for instances that participants did not self-disclose, and this allowed for the code to be refined as intentional self-disclosure. Credibility was established through the use of in-depth member checks, such as providing participants with copies of the transcribed interviews and asking for any corrective feedback. Study participants were also asked for feedback on the codes and categories. Participants reported that the final results were consistent with their experiences. They offered no other feedback with regard to the results, and thus, no other changes were made.
Results
Core Category: Affirmative Intersectionality
In GT, the core category is the central and stable narrative that relates to all other categories that were constructed from the data, while also taking into account the variation in observed incidences or behaviors (Fassinger, 2005; Holton, 2007). Affirmative Intersectionality was constructed as the core category in this study and is conceptualized as a dynamic means of delivering rehabilitation counseling services to sexual minorities living with CID. As a core construct, it considers the various forms of oppression that are associated with possessing both a sexual minority identity and CID, while supporting and encouraging a sense of pride for possessing both identities simultaneously. Furthermore, affirmative intersectionality was the mechanism fueling our participants’ overt and covert cognitive, affective, and behavioral processes when delivering professional services to sexual minorities living with CID. It was viewed as the facilitating agent exercised by our participants to promote action and change with their clients, whether the counseling goals of the client were vocational, psychological, or health related. As such, affirmative intersectionality was viewed as an approach that takes into account (a) aspects directly related to the counselor and the rehabilitation counseling process; (b) expectations of achieving outcomes that enhance the vocational, health, and psychosocial lives of sexual minority persons living with CID; and (c) diverse sexual minority persons across different developmental ages within different systemic contexts.
Four additional categories were constructed in support of affirmative intersectionality: (1) professional attributes, (2) alliance, (3) intersectional sensitivity, and (4) intersectional interventions. Within the core category of affirmative intersectionality, the salience of each supporting category is viewed as equivalent to the next, with each uniformly contributing to the practice of affirmative intersectional rehabilitation counseling with sexual minorities (see Figure 1 for visual depiction of the model). Each supporting category also possesses its own subcategories, which are discussed more fully below. The importance and inclusion of the constructed subcategories were determined via research team consensus and became salient during the comparative and recursive analysis process. In addition, the total number of participants who endorsed each code is provided.
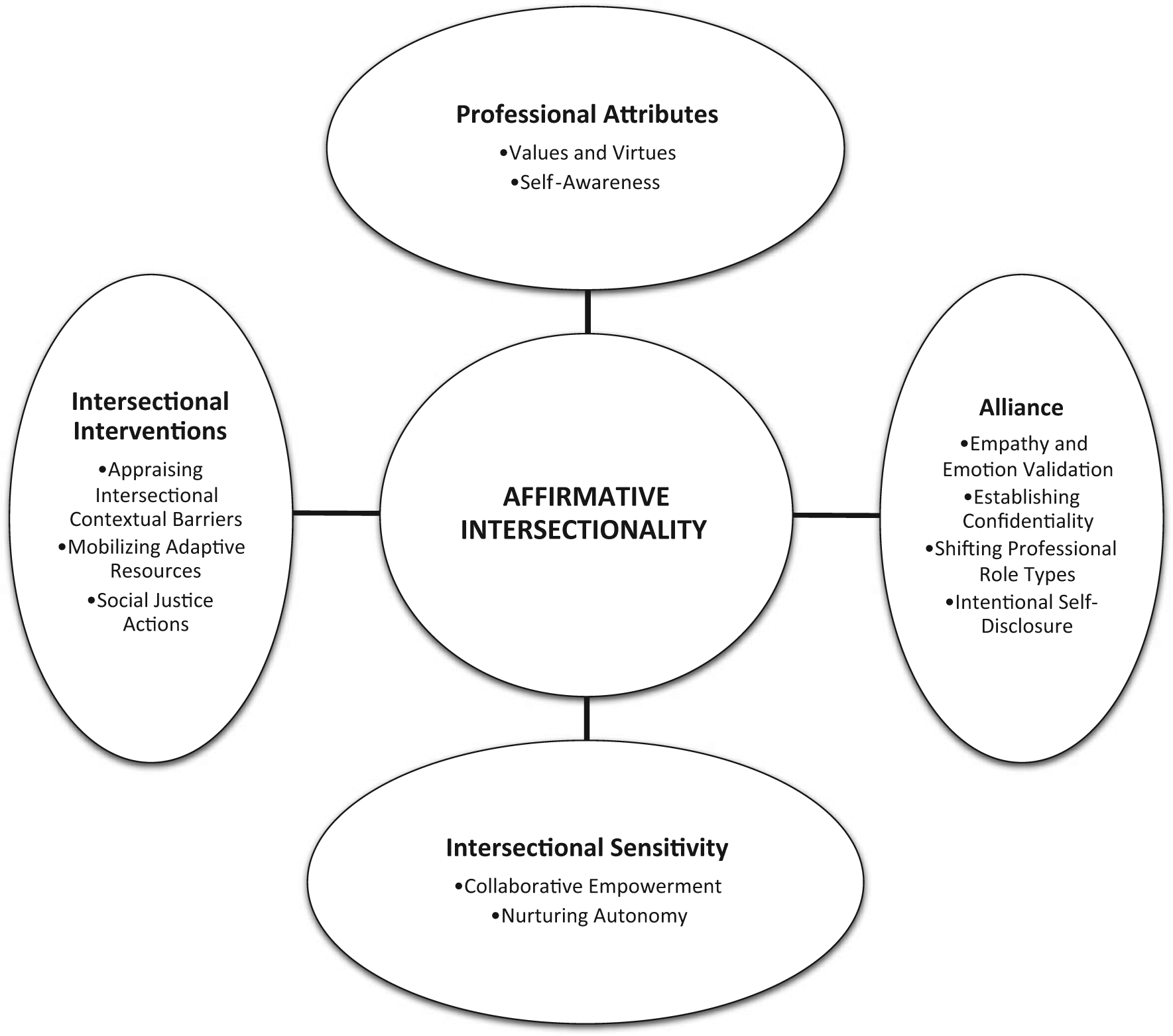
Model of affirmative intersectional rehabilitation counseling with sexual minorities.
Category 1: Professional Attributes
All participants identified and discussed self-perceived attributes and character traits that they believed contributed to their affirmative facilitation of rehabilitation counseling with sexual minorities living with CID. The most consistently expressed attributes and traits were (a) values and virtues (n = 12) and (b) self-awareness (n = 11). These self-perceived attributes and traits helped the participants in this study rely on their own personal strengths when utilizing an affirmative approach with sexual minority persons living with CID.
Subcategory 1a: Values and virtues
Among our participants, we asserted that values and virtues were the possession of righteous and benevolent beliefs that facilitated the desire to provide affirmative rehabilitation counseling to sexual minority persons. As Paula stated with regard to her values, “I believe in people. I value the human spirit, as a whole. People are important. Professionally, I think it’s guided by my virtues and ethics.” In relation to values and virtues, participants discussed possessing a sense of compassion, genuineness, acceptance, empathy, openness, being nonjudgmental, and happiness to describe themselves as rehabilitation counselors. Lisa stated, “I really believe I’m a genuine person. I’m not in the place of judgment, because we must always accept people in the context of what they’re coming from.” Colin reported, “It’s about being gentle and compassionate—that is something that I value. I’m happy to work with individuals the best I can to help them achieve their personal goals.”
Subcategory 1b: Self-awareness
Participants consistently des-cribed themselves as taking the time to be reflective, cognitively flexible, and self-understanding. We deemed that these personal awareness traits assisted with ethical service delivery when working with sexual minorities living with CID. Nicole, who maintained a private rehabilitation counseling practice, reported, I possess awareness, as rehabilitation counselors are trained to have. I try to keep a very strong awareness when I’m working with someone who is addressing his or her LGBT identity. I also try to be very aware of my limitations. My job is to improve the quality of their life and to be mindful of the fact that we are working on a particular treatment goal, and I must constantly check to see if I can help that person meet those treatment goals.
As demonstrated by the participant above, having a sense of self-awareness helped facilitate their rehabilitation counseling work with sexual minorities living with CID. This participant, like many other participants, experienced his or her interventions to be more goal directed as a result of being more aware of his or her own beliefs, limitations, biases, and even interests. As demonstrated by Danielle, “Internally, there are aspects about me that leave me hungry for information about people. I feel that my professional relationships with clients have really been strengthened because of my own awareness of my need to know more.” Some participants even connected their sense of self-awareness with their own professional development, competency, and growth as a rehabilitation counselor. As Shary stated, “It’s important for me to be conscious of my biases, and trying to counteract those biases with my counseling education, exposure, and experience.”
Category 2: Alliance
All participants described the need to foster and create an affirmative working alliance to achieve optimal outcomes with sexual minority clients living with CID. Optimal outcomes were subjectively evaluated and based on successful terminations, transitions, gainful employment, or the adoption of adequate vocational and health management strategies. The participants interviewed for this study identified a series of approaches related to establishing an affirmative working alliance, which included the following: (a) empathy and emotion validation (n = 12), (b) establishing confidentiality (n = 8), (c) shifting professional role types (n = 8), and (d) intentional self-disclosure (n = 6).
Subcategory 2a: Empathy and emotion validation
Participants expressed the importance of engaging in the stories of their clients with empathy and emotional validation. Participants encouraged their clients to explore their feelings, would consistently reflect emotions during counseling to emphasize understanding, and did so for the purposes of strengthening the counseling bond. Paula, who worked as a counselor in an urban prison, poignantly stated, I’m always focused on the client. I’m sensitive to where they are, and I meet the client where they are at. I validate the person and the world that they live in. It’s about validating my client’s feelings and concerns, and really making that known to them as much as possible. I reflect back to make sure I am understanding what they were saying. I emphasize their feelings. I want to connect with them and their world.
Julia indicated, “Once you develop rapport, a client will reveal more. Getting to understand their world means they talk about familial issues, they talk more about economic issues, and they open up.” Adopting an empathic worldview further allowed counselors the opportunity to establish rapport and genuinely appreciating their clients’ emotions, with the intention of strengthening the alliance to allow the client to disclose more personal information.
Subcategory 2b: Establishing confidentiality
Participants emphasized the importance of establishing confidentiality during the rehabilitation counseling process, especially because they were working with individuals who experienced marginalization as a result of both their sexual minority and CID identities. Bonnie indicated, “Some of my clients have had really bad experiences because of disclosing information about their personal relationships.” Participants relayed that their clients reported being discriminated against by physicians, potential employers, family members, schoolteachers, supplemental security income/supplemental security disability income workers, and VR personnel. When speaking of confidentiality at a state VR agency, Colin mentioned, We certainly talk about confidentiality. It comes into play because in a lot of instances my clients don’t necessarily want to disclose that they identify as lesbian, gay, or bisexual to employers, to friends, or to family. Sometimes, they haven’t even disclosed their sexual orientation to those people.
As such, focusing on confidentiality became an important aspect to the counseling practices of our participants, especially given the multiple systems that their clients would navigate. Spending time during the first or second counseling session to establish confidentiality especially allowed for the co-creation of safety. As noted by Lisa, who worked at a medical hospital, We talk about confidentiality because one of the biggest goals that I have is creating a safe space. When there’s safety, we are open to explore. It goes across the board, but especially my gay, lesbian, and bisexual clients, especially in the South, especially to those who are coming from other parts of the country. That makes me even more so aware of wanting to engage in a very transparent and very safe way to engage with that interpersonally.
Subcategory 2c: Shifting professional role types
Given the diversity of work settings and presenting concerns of their clients, participants discussed shifting the way they viewed their counseling roles when interacting with their sexual minority clients living with CID. Participants personified the need to be educators, advocates, mediators, facilitators, case manager, coaches, and supporters. Fiona stated, “I am a facilitator. As a facilitator, I can honestly say that my clients felt heard, understood, didn’t feel judged,” while Danielle mentioned, “My role is to be a cheerleader, of sorts. I use strength-based counseling for my clients, and I find that that works to help them identify their strengths and then build on that to greater functioning.” When asked about professional roles, Nicole clearly reported several different roles, “Sometimes I am a sounding board. Sometimes I am a supporter, I am a listener, I am a guider, and at times a teacher. Other times, I am a confronter.” As another example, Shary mentioned, A big part of my role is advocacy for the patients. There can be times where they’re not being heard, and so I can act as the mediator, especially because there are so many different personnel working—playing the advocate role specific to the rehabilitation setting.
Shifting their professional roles provided our participants an innovative means of forming strong working alliances and bonds. As a result, participants believed that their clients were heard, understood, and possessed the hope to achieve their personal goals.
Subcategory 2d: Intentional self-disclosure
Some participants discussed utilizing an appropriate level of self-disclosure to construct a trusting bond between themselves and their sexual minority clients living with CID. In some instances, participants chose to intentionally disclose some personal aspect related to their sexual orientation and CID status, or they disclosed aspects related to personal loved ones (e.g., family, friends) who identified as sexual minorities or persons living with CID conditions. Gaston stated, “I’m pretty open with my sexuality. I think that by me being open, it helps break down barriers or helps take away some stigma that can be attached with being gay.” Given the experiences related to her own disability, Julia discussed how she used self-disclosure with one of her clients, I was working with one individual who has a physical disability. This individual’s caretakers know that my client identifies as a member of the LGB community, but they don’t accept it. This creates difficulty because my client relies on these caretakers for transportation. So, while they will bring my client to school, they will not under any circumstance take my client on to a date, or to meet with other LGB identified people. I don’t drive myself. So, I would talk with my client about how I navigated issues of getting to and from school and I also talked about the different resources that I used.
It is important to note that there were participants who reported not disclosing their sexual orientation or a CID to clients, but the choice of not disclosing was also done intentionally. Either way, the intentionality surrounding self-disclosure was done to enhance the working alliance between the client and the counselor and was deemed beneficial by our participants.
Category 3: Intersectional Sensitivity
Given that this study focused on rehabilitation counseling practices among sexual minorities living with CID, participants from this study specifically addressed the need to approach the intersection of multiple marginalized identities with tactful care. Fiona mentioned, “I have to approach different aspects of people, together. I have to approach their sexual orientation and their disability.” Participants reported doing so via (a) collaborative empowerment (n = 8) and (b) nurturing autonomy (n = 8).
Subcategory 3a: Collaborative empowerment
Having acknowledged the degree of prejudice and discrimination that their clients encountered during their daily lives as a result of their multiple marginalized identities, participants discussed investing time to collaborate on the development of dignity, strength, and power in the lives of their clients. When describing her counseling approach, Julia stated, “We try to look at this as a collaborative relationship. It is very important to provide my clients the skills to generate respect in the world, and be able to live their lives in a way that’s honest and safe.” Bonnie, who worked at a state VR agency, reported, I have a very empowering counseling style. Some individuals will come to their VR counselor and expect labor market information to be printed out for them and being told what to do and where to go. I collaborate with my clients to have them take the first step in the career process, like having them do an informational interview, or self-directed search, or going home to do their own labor market research, then coming back to me to talk about their research. I have an empowering approach, and I am pretty open about boundaries and my expectations for a consumer.
The rehabilitation counseling process was viewed by most of our participants as a means of developing tools that could be used by their clients to advocate for honest expression of their multiple marginalized identities. In addition, our participants collaboratively empowered their clients to help them achieve a sense of mastery over their personal goals.
Subcategory 3b: Nurturing autonomy
As a result of the unfair treatment from possessing multiple marginalized identities, participants discussed the importance of respecting and fostering the free will and independence of their clients during the counseling process. Fiona indicated, One of the things I do is try to allow the individual to be as autonomous as possible. So if the person calls with a concern or question, I’m not recommending or telling them they need to do something. I discuss things with them and I give them as much information as possible so my client can make informed decisions themselves. I think that really helps.
In some instances, participants talked about the limited autonomy experienced by their clients as a result of their CID, and as such, participants were further committed to nurturing the development of their clients’ sense of independence. In relating a particular incident with a sexual minority client living with HIV-related vision impairments, Nicole, who also worked in a private practice reported, My client had a family member that blocked me from direct contact, and was overly possessive and guarding in ways that did not promote my client’s autonomy. I believe my client was grateful to have an advocate in this family member and signed full release for me to communicate through this family member. However, I always tried to make the effort to get past the family member and into direct engagement with my client, hoping always to increase my client’s independence even when it wasn’t easiest to do so.
As evident by the quotes above, autonomy was operationalized as the ability to make one’s own decision, being informed, and free from external forces that could distract or overpower one’s own implementation of independence. Participants were committed to respecting this principle for the genuine betterment of their clients.
Category 4: Intersectional Interventions
Participants disclosed the importance of being affirmative and theoretically intentional when conceptualizing and implementing their rehabilitation counseling interventions and specifically identified several interventions that they believed were effective with sexual minorities living with CID. Three subcategories were constructed: (a) appraising intersectional contextual barriers (n = 11), (b) mobilizing adaptive resources (n = 10), and (c) social justice actions (n = 10).
Subcategory 4a: Appraising intersectional contextual barriers
With regard to their sexual minority clients living with CIDs, participants discussed needing to assess and identify obstacles that limited functioning or any progression toward personal goals. Working with youth and families in the foster care system, Danielle stated, I sit back and explore all aspects of a person’s life—both their sexual orientation identity and their disability. I want my clients to tell me what they think is important to them and what they feel I should know. I do this because it matters. I specifically focus on what are the unique barriers and support systems that they have in place that could affect their access to things in regards to their disability or sexual identity. I explore who in their life is safe and unsafe with regards to their disability and sexuality.
As evident by the quote above, participants specifically explored the perception and responses that their clients had of their respective environments. In particular, participants discussed attending to experiences of discrimination, isolation, loneliness, and homelessness as barriers relevant with this population. By far, stigma was the most prevalent contextual barrier that our participants focused on in their practice. When discussing incidents regarding a gay client living with HIV and mental illness at an outpatient psychosocial medical center, Virginia discussed, There is considerable stigma, a stigma related to both the disability and gay identity. Stigma is the number one barrier I’m assessing. The stigma doesn’t always have to do specifically with the LGBT identity, but a lot of it has more to do with ignorance as far as disabilities are concerned. You know, how disabilities are spread or not spread, what is contagious versus not contagious, and lack of knowledge of mental health issues.
Participants also discussed the need to appraise intrapersonal-related barriers, such as sexual minority stressors (e.g., internalized homophobia, concealing sexual orientation, anxiety) and internalized ableism. When discussing her approach of identifying barriers perceived by her sexual minority clients living with CID at a college student disability office, Hermione reported, I have seen clients have the perception that things are more likely to go wrong in their lives. Also, the level of worry and judgment are pretty high in the instances that I’m thinking. Those are the barriers. [Interviewer: Do you have a sense of why that may be?] Because of the way our society is when it comes to sexual minorities. Even though men are kissing each other on television, I don’t think society, as a whole, is ready for that. The way we are socialized impacts us and we internalize message of heterosexism. [Interviewer: Then, how do you address barriers in your counseling?] In session, I do. That’s the first thing I think about, “what are the barriers?” Because in my agency, barriers are what we’re trying to get out of the way so that my clients can progress with their goals and get on with their lives—whether it be barriers from their disability or sexual orientation. That’s the first thing I always remember, “What is that environmental barrier that keeps that person from moving forward?”
Participants made it apparent that a holistic focus was necessary when appraising intersectional contextual barriers, particularly interpersonal, intrapersonal, and environmental domains.
Subcategory 4b: Mobilizing adaptive resources
Participants discussed the importance of helping their clients assemble, organize, and utilize various psychological resources to optimize behavioral, emotional, and vocational functioning. Among our participants, activating coping resources to address stressors related to stigma was most apparent. Fiona discussed how she approached coping in her private rehabilitation counseling practice, I currently have a 40-year-old lesbian who is coming in regarding loneliness, relationship issues, and she has a severe psychiatric history. She is coping well. She is educated and has many year of experience. During our counseling, she is also much more aware of how stigma impacts her and we can talk about ways that she could use her coping to deal with the stigma. The 15-year-old teenager that I’m working with on the other hand, who is questioning his sexuality and seeing me for a learning disorder, talks about stigma and disability in a very different way. In my experience, I think my adolescent LGB patients struggle with stigma differently, and really need additional support in life. And if I could think of a population that needs more support I would go with teenagers because they don’t fully understand stigma and oppression. They don’t understand those things because they’re not developmentally there. But also because in my opinion, especially where I geographically live, it is just really hard. Some high schools are open and there is less stigma and oppression, but some schools are not. This is very hard on my part when working with those patients to address what they are comfortable with and talking to them about how they are going to cope with certain situations in school.
As with other participants, this particular quote exemplified the manner in which our participants altered and developmentally contextualized the manner in which they mobilized coping resources. Participants in the study also highlighted helping their clients implement adequate social supports for interpersonal coping and the use of creative outlets. Shary mentioned, We used art and creativity. Also humor was a big thing that each client had. Humor has played a big role, which sometimes can be a hindrance, but as for getting through the bumps and bruises, the creative outlet has been very helpful. I had clients who were into radio, acting, poetry, creating children’s plays. Those were the things that helped my clients thrive. Support is another important component. The people that were meaningful to my clients were supportive of them coming out and managing their health conditions. Those were the protective factors. Having a support system is crucial. Those who had that seemed to do better than those who were actively disowned.
Other participants also discussed the importance of bolstering logical reasoning and problem solving skills, guiding clients through the decision-making process, and positively reinforcing and encouraging adaptive behaviors. As demonstrated by Gaston, When it comes to my counseling work, I am all about helping my clients hear themselves, helping them generate a solution, problem solving that solution, weighing the pros and cons. I think I’m really good at that and it takes lots of patience.
Subcategory 4c: Social justice actions
Participants strongly identified as sexual minority allies and reported moments in which they personally took action to buffer against stigma-related offenses. Participants discussed the importance of maintaining professional relationships with other ally affirming professionals and being knowledgeable of community referrals and resources that provided services to both sexual minorities and persons living with CID conditions. In some instances, participants discussed being directly involved in social-justice-related advocacy efforts for their clients. As demonstrated by Danielle, who was working with a family who had a sexual-minority-identified adolescent, I have stepped in to speak to the school personnel, such as the principal and Special Ed teacher because I was not sure they were aware of issue going on with my client. And I do think that because I was a professional that they were more likely to listen to me more than they would listen to the parents. If it is what is needed for my client, then I will do it.
As demonstrated by the participant above, she took direct action and systemically intervened to advocate for her client. Fiona took action by the use of curious inquiry as a means of challenging policies and procedures that appeared stigmatizing against sexual minorities and persons living with CID: I have collaborated and worked in conjunction with other counselors and staff members that were either not comfortable with LGBT individuals or they just did not have the right professional skill set to approach things on a treatment level with an individual who was LGBT. In this one particular setting where I encountered this, we had group team meetings. When LGBT issues came up—or if that come up in individual supervision or peer supervision—I feel that part of my duty being a professional is to bring that up, but I would do it in a particular way. I would ask the person questions, “Are you having difficulty in that area?” “Have you ever seen it this way?” I acted like Colombo in the way I questioned.
Discussion
As far as we know, this is the first study to construct a substantive model, grounded in aggregated interview data from demographically and professionally diverse certified rehabilitation counselors working with sexual minorities living with CID. Affirmative intersectionality was infused throughout the various character traits of our participants, functioned as a facilitating force behind the interactional dynamics between the rehabilitation counselor and client, and directed the participants in this study to intentionally implement contextualized interventions with sexual minorities living with CID. Relatedly, there are elements of the model that are consistent with existing practices of counseling that warrant some discussion.
First, similar to existing recommendations for counseling and psychological practice with sexual minorities (e.g., APA, 2012a, 2012b; ALGBTIC, 2012), our participants promoted acceptance, honored differences, and recognized the unique benefits of possessing both sexual minority and CID identities. In conjunction with established counseling practices with sexual minorities (Greene, 2007; Israel et al., 2008; Matthews, 2007), affirmative intersectionality appeared to overlap with existing strengths-based counseling paradigms that encourage counselors to magnify intrinsic resiliencies, enhance intrapersonal strengths, and focus less on deficits when working with marginalized populations (Smith, 2006). In addition, participants in this study were exercising appropriate multicultural counseling competencies (Sue & Sue, 2008), as evidenced by the use of self-awareness, awareness of personal values and virtues, suspending heterosexist-bias, not making assumptions about the sexuality of their clients, and demonstrating acceptance in all aspects of diversity.
Second, affirmative intersectionality promotes that the psychosocial experiences of sexual minorities living with CID be considered in their respective developmental and environmental contexts. In line with bioecological approaches (Bronfenbrenner & Morris, 2006) and developmental contextualist (Chen et al., 2010) approaches to counseling, the participants in our study were well aware that development occurs in context, and that context occurs within multiple intersecting systems. As a result, our participants possessed a sense of agency that helped them implement relevant interventions that contextualized the intersecting identities of their marginalized clients. Participants in this study evaluated a multitude of contextual barriers (Smart & Smart, 2006), participated in social justice actions (Constantine et al., 2007), and mobilized culturally sensitive and adaptive resources to address oppressive-related stressors (Sue & Sue, 2008).
Third, in conjunction with Smart and Smart’s (2006) recommendations for counseling persons living with CID, the participants in this study viewed both sexual minority identity and CID being holistically integrated—never with significant importance placed on one identity at the expense of another. Even if the presenting concerns were not related to sexual orientation or CID, participants in the study displayed affirmative attitudes and behaviors toward both identities (Matthews, 2007). More specifically, participants implemented relevant interventions with the appropriate sensitivity toward intersectionality. As with other counseling approaches with persons living with CID, this was most evident among participants who reported focusing on empowerment and autonomy with their clients (Olkin, 2001; Smith, 2006).
However, our findings still offer some unique contributions. First, our results are specific to the practices of rehabilitation counselors in their diverse settings. Participants in this study were reconfiguring their practices to be more applicable with sexual minorities living with CID. This is important because rehabilitation counselors provide essential services that differentiate them from other counseling professions. As such, rehabilitation counselors may have to intervene differently with their sexual minority clients when compared with other helping professions. Second, the model from this study is not exclusively conceptual like other reported models (refer to Harley et al., 2000; Harley et al., 2002). Rather, the model was constructed from data, providing rehabilitation counselors the opportunity to use a form of evidence-based practice with such a vulnerable population. A third unique aspect of our findings is that our participants reported practices that were sensitive to the intersection of marginalized identities. As Israel et al. (2008) reported, much of the extant literature regarding counseling practices with sexual minorities has centered on characteristics, behaviors, and attitudes of counselors. The results of this study still encompass counselor attitudes, but it extends the current literature by delineating particular tactics that affirm both sexual minority and CID identities.
The working alliance was another significant component to the affirmative intersectionality model, especially given how quintessential it is to the practice of counseling (Wampold, 2001). In particular, participants from this study discussed using empathy and emotional validation, confidentiality, shifting roles, and intentional self-disclosure to help nurture the development of the working alliance. Whereas Millington (2012) identified a series of similar tactics (e.g., empathy, counselor disclosure) used by rehabilitation counselors, the results of this study revealed that our participants were reconfiguring these particular tactics to be more sensitive to the intersection of sexual minority and CID identities. Our participants recognized that to construct an emotionally collaborative bond, intentionally affirming both identities was necessary when establishing a working alliance.
Last, affirmative intersectionality demonstrates malleability and fluidity. Among our participants, affirmative intersectionality did not focus on any particular counseling theory or technique. Rather, our participants were already operating from diverse theoretical and empirically intentional counseling frameworks. As a result, the affirmative intersectionality approach lends itself to being pan-theoretical (Millington, 2012). Participants integrated components of their theoretical or empirical approaches in effort to refine their interventions among their sexual minority clients living with CID. This helped fortify their approach, while modifying and integrating professional standards to provide affirmative rehabilitation counseling.
Implications for Education and Supervision
The results of this study indicate some important implications for training, education, and supervision. First, it is important for rehabilitation counselor educators to consider an intersectionality framework in the multicultural counseling curriculum (Cole, 2009; Parent et al., 2013). Within the intersectionality framework, particular attention should be given to LGBQ persons, especially given the significant health disparities noted with this population (Cochran & Mays, 2007; Fredriksen-Goldsen et al., 2012). Second, rehabilitation educators and supervisors should continue helping rehabilitation counselors understand the impact that multiple marginalized identities have on the vocational, health, and developmental milestones of their sexual minority clients living with CID. In doing so, educators and supervisors should explore how to incorporate the experience of stigma and oppression in clinical case conceptualizations and consider contextualized interventions that could be used in both vocational and clinical settings. Last, educators and supervisors should intentionally continue to help rehabilitation counselors develop affirmative attitudes and could utilize this proposed model as a means of marking where rehabilitation counselors are with regard to their development.
Limitations
Although this study focused exclusively on the practices of rehabilitation counselors to inform the field of rehabilitation counseling, the results of our study have several limitations. Consistent with other qualitative research studies (e.g., Noonan et al., 2004), we were interested in exploring a scope of experience to generate a substantive model and thus limiting the generalizability of our results exclusively to rehabilitation counseling practices with sexual minorities living with CID. However, our results do provide a type of evidence-based framework that could inform rehabilitation counseling practices with this particular population. Second, although we were able to gather participants from diverse backgrounds (i.e., U.S. regions, racial/ethnic identities, sexual orientation, CID status), majority of our participants identified as cisgender women. Although some men expressed interest in the study, some declined to participate. It is unclear if this is indicative of recruitment concerns or if their decline to participate suggests potential gender effects on rehabilitation counseling practice with sexual minorities living with CID conditions. Third, given that we interviewed participants to discuss their experiences of effective practices and outcomes, our results are limited to the perceptions and beliefs of our participants. Although we used multiple analytic procedures to triangulate our analyses (e.g., multiple coders, various forms of member checking), we were unable to gather other sources to triangulate our data (e.g., relevant work samples, supervisor or client feedback).
Suggestions for Future Research
Of the upmost importance, given the current data on CID among sexual minority populations (e.g., Cochran, 2001; Conron et al., 2010; Duke, 2011; Fredriksen-Goldsen et al., 2012; Poteat et al., 2009), rehabilitation counseling scholars are highly encouraged to continue exploring sexual minority issues within the field. Rehabilitation counselors from a variety of work settings are encountering sexual minorities, and it is the duty of the profession to provide adequate scholarship and data that benefit the field of rehabilitation counseling. Furthermore, the results of this study suggest the necessity to assess the effectiveness of the emerged model under varying systematic methods of investigation (e.g., qualitative, quantitative, mixed-methods). Client outcomes should be assessed alongside the counseling model, particularly satisfaction with counseling, vocational-related variables, quality of life, client-life functionality, and health-related symptomatology. Furthermore, other plausible models of affirmative intersectional rehabilitation counseling could be proposed and tested. Last, the results of this study also imply the need for a systematic evaluation of rehabilitation counselors working with transgender persons across different rehabilitation counseling settings. Transgender persons are an important population and deserve specialized attention in the field of rehabilitation counseling.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.