
Abstract
This article updates, after 20 years, Hershenson’s systemic, ecological model for rehabilitation counseling by eliminating elements of the original model that proved to be superfluous and by reflecting current directions in the field.
This article updates Hershenson’s (1998) systemic, ecological model for rehabilitation counseling to reflect current conditions and practices. This model conceives of rehabilitation counseling as a system interacting with other systems that make up the macrosystem of disability and rehabilitation (Bronfenbrenner, 1979). The model indicates system-specific counselor functions and interventions.
The Updated Model
The updated model is presented in Figure 1. The large arrow on the left represents the disability (congenital or acquired) that organized and maintains this macrosystem. The consumer system is located at the center of the diagram. This system contains three components: personality (P), competencies (C), and goals (G). Personality includes the consumer’s self-image; motivational system; pattern of needs, interests, and values; and reaction to disability. Competencies include activities of daily living, interpersonal skills, work habits, job-related skills, and learning capacities. Goals include learning, working, living, and socializing. These components are connected by double-headed arrows representing their interactive nature. As illustrated in Figure 1, disability initially impacts competencies (at the tip of the arrow), and its effect then spreads to personality and goals through their interconnection.
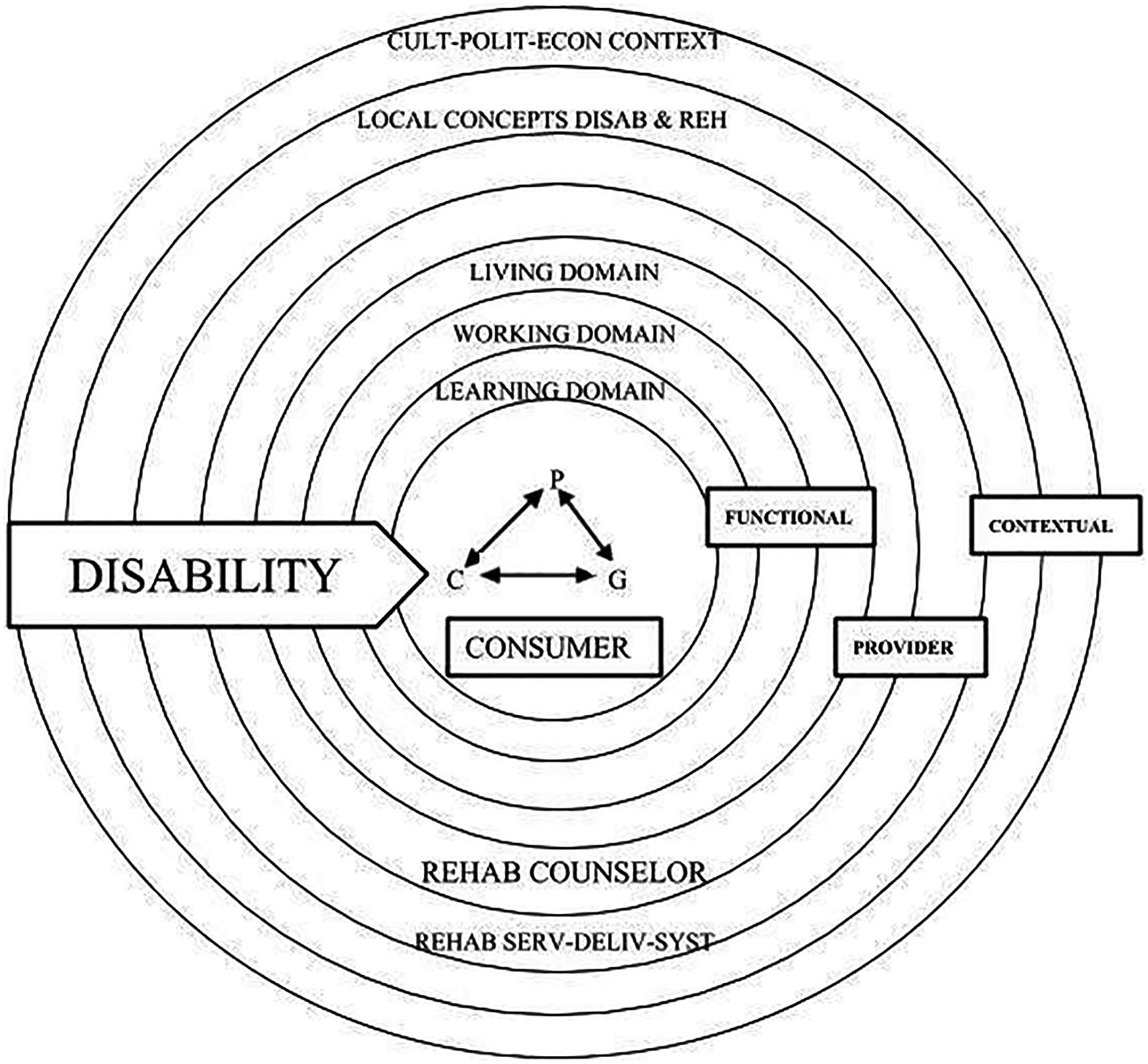
The macrosystem of disability and rehabilitation.
The three concentric rings surrounding the consumer system represent the domains of learning, working, and living. These domains form the functional system, as they are the environments within which the consumer functions (Anthony, Howell, & Danley, 1984). The living domain includes self-maintenance and community adjustment.
The provider system consists of the service delivery system (e.g., government and voluntary agencies) and the individual rehabilitation counselor. The service delivery system contains agency policies, practices, and resources. The counselor is treated as a separate subsystem because each counselor practices in her or his own way and has unique effects on consumers.
The outermost contextual system is an “exosystem,” that is, a setting that does not involve the consumer “as an active participant but in which events occur that affect [her/him]” (Bronfenbrenner, 1979, p. 237). Local normative conceptions of disability and rehabilitation largely determine how consumers will be treated. All systems are affected by the larger cultural–political–economic context (the outermost ring). Global economic trends (e.g., automation), national and state politics, and broader cultural norms (e.g., caring for the less fortunate, the work ethic) affect what, and to whom, rehabilitation services are provided. We shall next discuss the model’s implications for professional practice.
Application of the Updated Model to Rehabilitation Counseling Practice
How this model informs current practice is shown in Table 1. Each component of each system calls for a specific type of intervention, which is elicited by the counselor exercising a particular function. For example, to restore or replace impaired consumer competencies, the counselor must coordinate the range of services required (e.g., physical therapy, vocational evaluation, retraining, job coaching). To counter the effects of the disability on personality and goals, the counselor must employ the counseling function to help the consumer reintegrate her or his personality, become remotivated, and reformulate foreclosed goals. When a consumer encounters problems in a functional domain, the counselor acts as a consultant to restructure that domain (e.g., participate in transition planning, assist employers meet ADA [Americans with Disabilities Act] requirements, provide guidance to families). When conditions in a domain or in the contextual system present a physical or attitudinal barrier to consumer success, the counselor must act as a change agent, advocating on behalf of the consumer. Throughout her or his work, the counselor acts as case manager, organizing and directing all activities on behalf of the consumer as effectively as possible, consistent with the policies, practices, and resources of the agency. Finally, the counselor must continuously reexamine her or his professional practices to keep them maximally effective, up to date, and consistent with professional ethics.
The Rehabilitation Counseling Process (Revised).
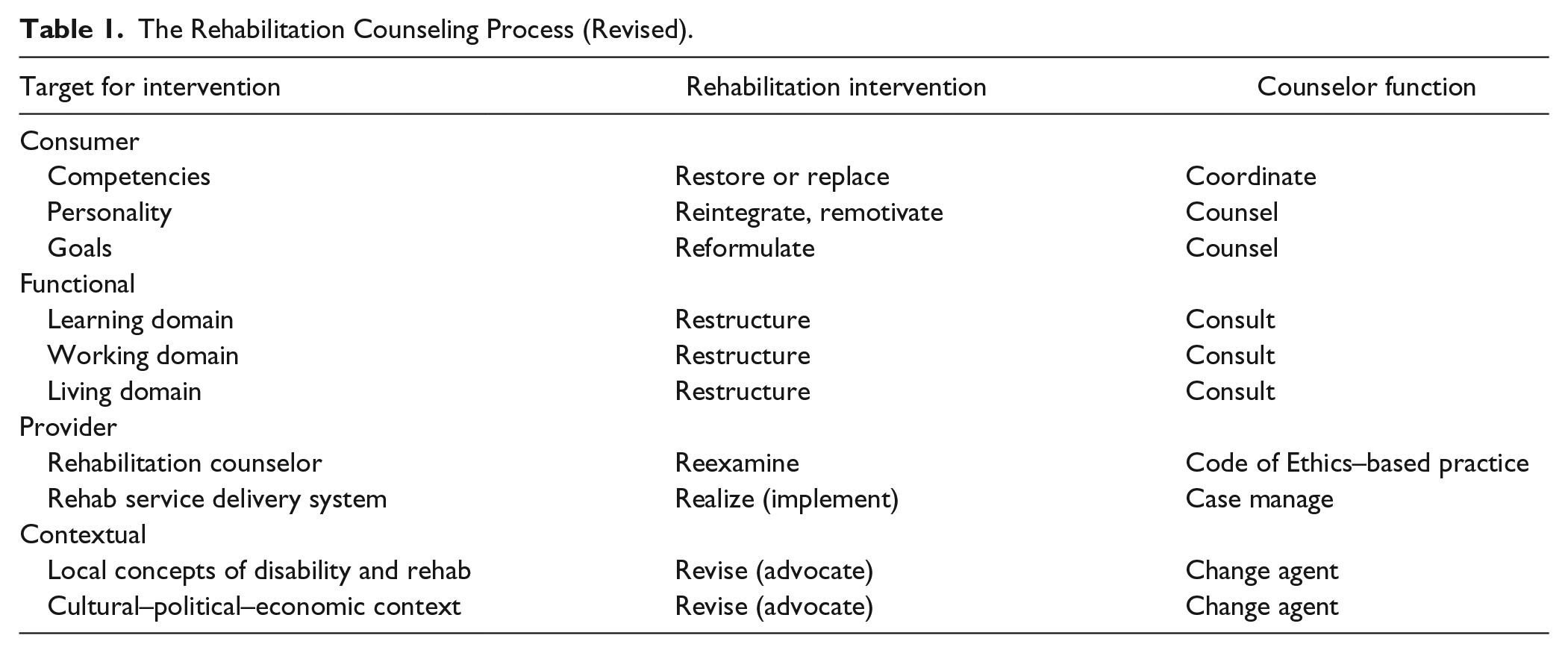
The role of the counselor is to determine, in conjunction with the consumer, which intervention or combination of interventions to employ at each point in the rehabilitation process. The counselor functions designated in Table 1 for addressing particular issues are generally the default option but not necessarily the only choice. In making that determination, the counselor must consider how each part of the macrosystem might impact the intervention to improve or diminish its effectiveness. Does any part of the macrosystem present value assumptions, behavioral expectations, skill demands, physical or attitudinal barriers, resources or supports, or opportunities or rewards that could facilitate or impede that intervention?
Changes From the Earlier (1998) Version of the Model
Major changes from the original model include adding the learning domain to the functional system and merging the family, school, and peer developmental environments (formerly in the consumer system) into the functional system. This permits clearer tracking of progress in each functional domain and reflects the increased attention to school-to-work transitioning in counseling practice. Given the increased emphasis on advocacy in recent iterations of the Code of Ethics (Waldmann & Blackwell, 2010) and in CACREP (Council for Accreditation of Counseling and Related Educational Programs) accreditation standards, change agent was added as a major counselor function. Counselor self-reexamination was changed to emphasize ethics as central to professionalization.
Finally, this exercise demonstrates the need to update theories that guide current practice.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.